Recurrent, Severe Coital Headaches Associated With Bilateral Carotid Artery Aneurysms and the Effect of Endovascular Treatment
Emma L Martinez Arellano, Hannah Lu, George Ishac, Hashem Shaltoni, Ruiqing Sun

TL;DR
A 41-year-old woman with severe coital headaches was found to have carotid artery aneurysms, and her symptoms improved after endovascular treatment.
Contribution
This case highlights a rare association between coital headaches and carotid artery aneurysms, emphasizing the importance of thorough differential diagnosis.
Findings
Bilateral carotid artery aneurysms were identified as the cause of recurrent coital headaches in a patient with a history of migraines.
Endovascular stent placement led to significant improvement in headache frequency and resumption of normal sexual activity.
The case underscores the need to consider life-threatening causes when evaluating recurrent coital headaches.
Abstract
Headaches are one of the most common chief complaints in the outpatient setting. Distinguishing between benign and life-threatening headaches can be difficult, particularly in the setting of a pre-existing history of headaches. Here, we present a 41-year-old female with a past medical history of migraines and uterine leiomyoma status post hysterectomy about nine months ago who presented to the clinic for severe coital headaches and worsening migraines starting eight months ago. Computer tomography angiogram (CTA) head and neck demonstrated bilateral para-ophthalmic internal carotid artery (ICA) aneurysms (right, 7.5, left 6 mm). A diagnostic cerebral angiogram (DSA) was subsequently done and confirmed the CTA findings. The patient underwent left and right flow-diverting stent placement two and four months later, respectively. One week after the right ICA stent placement, her headaches…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
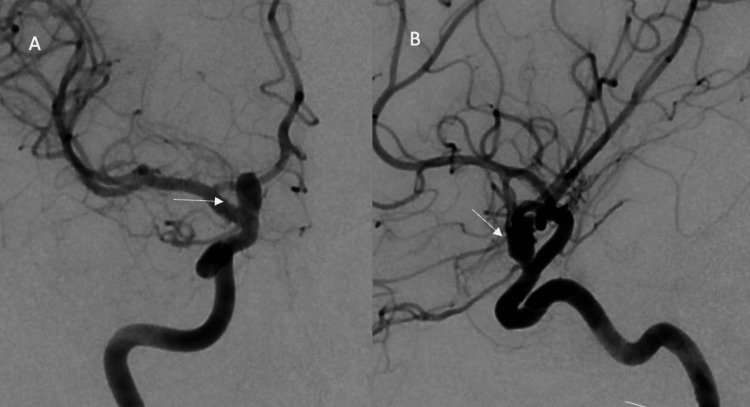 Figure 1
Figure 1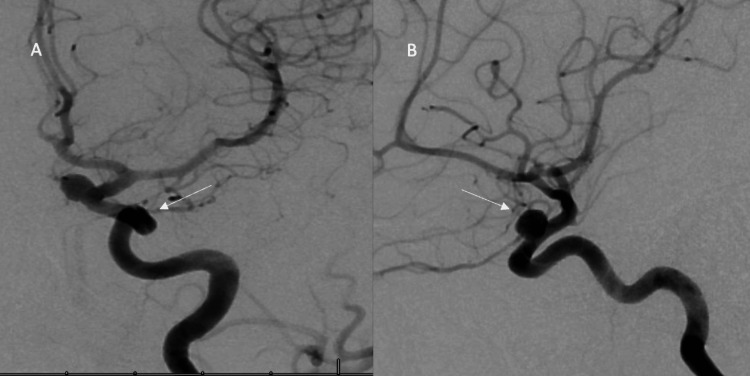 Figure 2
Figure 2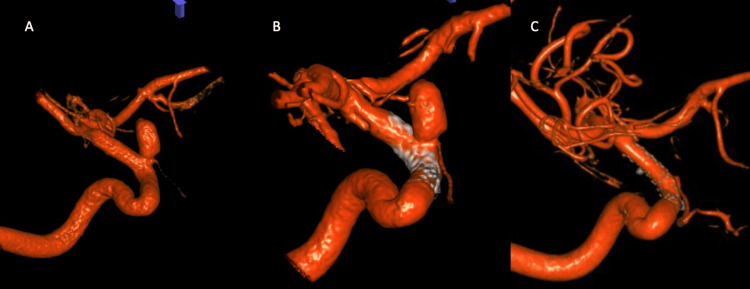 Figure 3
Figure 3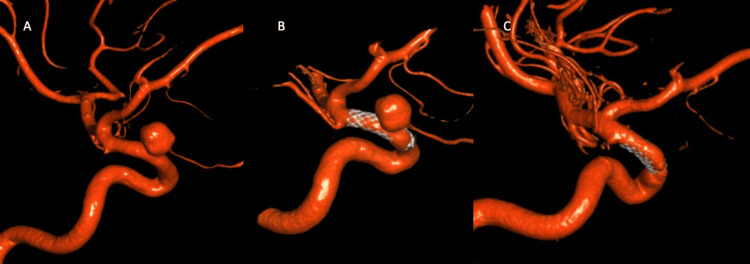 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMigraine and Headache Studies · Intracranial Aneurysms: Treatment and Complications · Cerebrovascular and Carotid Artery Diseases
Introduction
Headaches associated with sexual activity (HASA) are described as those that occur during sexual activity and are either abrupt in onset or intensifying with increasing sexual excitement [1]. Malignant coital headaches can present as acute emergencies involving hemorrhagic or ischemic events while others can present as insidious processes consisting of cerebral aneurysms, arteriovenous malformations, hydrocephalus, or reversible cerebral vasoconstriction. An estimated 3.8% to 14.5% of patients had an aneurysmal rupture resulting in subarachnoid hemorrhage immediately following sexual activity [2]. Thus, timely intervention and standardized diagnostic workup of associated comorbidities are instrumental in preventing fatalities. There are only two reported cases of recurrent coital headache related to an unruptured saccular aneurysm of the carotid artery and fusiform aneurysm of the vertebral artery respectively [3,4].
This case report was previously presented as a poster at the 2023 American Neurological Association meeting on September 10, 2023.
Case presentation
A 41-year-old female with a past medical history of migraines, blood loss anemia, and uterine leiomyoma status post hysterectomy nine months ago presented to the clinic for severe coital headaches starting eight months ago. Her coital headache was sudden in onset and explosive in nature with gradual resolution of symptoms in varying timeframes (30 minutes to 2 hours). Simultaneously, she began having frequent, severe migraines about three to four times weekly that were refractory to medical management. Her baseline was two episodes of migraine headaches per month. Neurological examination on initial presentation was unremarkable. Computer tomography angiogram (CTA) head and neck demonstrated bilateral para-ophthalmic internal carotid artery (ICA) saccular aneurysms (right, 7.5, left 6 mm). A diagnostic cerebral angiogram was subsequently done and confirmed the CTA findings (Figures 1A, 1B, 2A, 2B).
(A) Anterior view of the right internal carotid artery (ICA) aneurysm diagnostic cerebral angiogram (DSA); (B) Lateral view of left ICA aneurysm DSA
(A) Anterior view of left internal carotid artery (ICA) aneurysm diagnostic cerebral angiogram (DSA); (B) Lateral view of the left ICA aneurysm DSA
The patient underwent left and right flow-diverting stent placement two and four months later, respectively (Figures 3B, 4B). One week after the right ICA stent placement, her headaches had improved to one to two times per week. Six months after stent placement, she resumed her normal sex life and her migraines returned to baseline. The patient underwent repeated cerebral angiogram after five months of a right ICA aneurysm intervention, which demonstrated complete obliteration of a right ICA aneurysm (Figure 3C) and left ICA aneurysm (Figure 4C) compared to pre-intervention (Figures 3A, 4A).
(A) 3D reconstruction of right internal carotid artery (ICA) aneurysm pre-treatment; (B) 3D reconstruction of right ICA immediately after flow-diverting stent placement; (C) 3D reconstruction of the right ICA six months after flow-diverting stent placement
(A) 3D reconstruction of the left ICA aneurysm before intervention; (B) 3D reconstruction of the left ICA immediately status post flow-diverting stent; (C) 3D reconstruction of the left ICA six months after flow-diverting stent placement
Discussion
Ruptured intracranial aneurysms are by far the most common cause of non-traumatic subarachnoid hemorrhage, which is a neurological emergency with potentially devastating consequences. There is evidence that some of the cerebral aneurysm rupture cases are precipitated by sexual intercourse and intense physical exertion, which increase the risk of aneurysm rupture by as much as 15-fold [5]. Coitus and physical exercise share some physiological similarities - hyperdynamic alterations in blood pressure, heart rate, respiratory rate, and muscle tone, which might be potential precipitants for cerebral aneurysm growth and rupture. However, Reynolds et al. demonstrate that sexual intercourse has a higher risk for aneurysm rupture than physical exercise alone [2]. During sexual intercourse, there is an increase in the transmural pressure across a preexisting aneurysm wall by increasing the mean artery blood pressure (MABP) and/or decreasing the intracranial cerebral pressure. In contrast, during physical exercise alone, the increase of MABP is counterbalanced by the increase of intracranial pressure. Rapid stretching of the aneurysm wall during intercourse might be the reason for HASA.
Coitus was the immediately preceding activity in 3.8-14.5% of patients suffering from aneurysmal subarachnoid hemorrhage. Therefore, HASA may be an important harbinger of a cerebral aneurysm with the potential for future rupture. Early recognition and neurovascular imaging are warranted. When HASA first occurs, it is critical to exclude secondary causes of headache, which include cerebral aneurysm [4,5], subarachnoid hemorrhage [6], cerebral artery dissection [7,8], reversible cerebral vasoconstriction [9], and cerebral ischemic or hemorrhagic stroke [9-11]. Two existing case reports describe secondary sexual headaches associated with unruptured, unilateral aneurysms. HASA attributed to unruptured, bilateral, saccular aneurysms has yet to be reported in the literature. This case reports a patient with a longstanding history of migraine with new-onset HASA who was found to have bilateral ICA saccular aneurysms and was managed with flow-diverting stents successfully.
In our case, the endovascular intervention (bilateral flow diverting stent placement) not only resolved the coital headache but also improved the patient’s regular migraine. This is consistent with previous studies that demonstrated coil embolization of unruptured aneurysms resulted in a reduction of the severity of regular headaches in a majority of patients [12-14].
There is a high percentage of subarachnoid hemorrhage resulting from aneurysmal rupture immediately following sexual activity [2]; however, there are few case reports regarding unruptured cerebral aneurysm associated with coital headache, which raises the hypothesis that coital headache associated with an unruptured cerebral aneurysm is under-reported or under-diagnosed. Considering the good outcome of surgical intervention of cerebral aneurysms before a devastating hemorrhage occurs, it is evident that early diagnosis of intracerebral aneurysm associated with HASA is crucial.
Conclusions
We report a case of recurrent severe coital headaches associated with bilateral carotid artery aneurysm diagnosed by CTA and diagnostic cerebral angiogram. The patient was successfully treated with bilateral flow-diverting stent placement resulting in improvement of headaches and quality of life. When evaluating a patient with coital headaches, it is important to keep a wide arsenal of differentials in order to rule out potential catastrophes such as aneurysms. Timely diagnosis and intervention with endovascular flow diversion or coiling can prevent fatalities and improve outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Headache associated with sexual activity—a narrative review of literature Medicina (Kaunas) Ściślicki P Sztuba K Klimkowicz-Mrowiec A Gorzkowska A 7355720213444094110.3390/medicina 57080735 PMC 8400207 · doi ↗ · pubmed ↗
- 2Sexual intercourse and cerebral aneurysmal rupture: potential mechanisms and precipitants J Neurosurg Reynolds MR Willie JT Zipfel GJ Dacey RG 96997711420112054059910.3171/2010.4.JNS 09975 · doi ↗ · pubmed ↗
- 3Fusiform aneurysms of the vertebral artery: a hidden cause of exertional headache?Cephalalgia Mauri G Vega P Murias E Vega J Ramón C Pascual J 7157183220122268409910.1177/0333102412449928 · doi ↗ · pubmed ↗
- 4Recurrent coital headache associated with an unruptured carotid saccular aneurysm Headache Uterga JM de Garay MA de Luna IO Uribarri JB 123212334920091954915810.1111/j.1526-4610.2009.01479.x · doi ↗ · pubmed ↗
- 5Physical activity and subarachnoid haemorrhage: a population based case-control study J Neurol Neurosurg Psychiatry Fann JR Kukull WA Katon WJ Longstreth WT Jr 7687726920001108022910.1136/jnnp.69.6.768PMC 1737186 · doi ↗ · pubmed ↗
- 6Review of severe headache after sexual activity with a case presentation J Emerg Med Case Rep Ertok I Çelik GK Otal Y Erol E Sarıkaya P Gökhan S 11311652014 https://www.acarindex.com/journal-of-emergency-medicine-case-reports/review-of-severe-headache-after-sexual-activity-with-a-case-presentation-899908
- 7Expert opinion: sexual intercourse followed by headache and transient monocular visual loss Headache Evans RW Moore KL 6166204820081837738510.1111/j.1526-4610.2008.01065.x · doi ↗ · pubmed ↗
- 8Thunderclap headache with orgasm: a case of basilar artery dissection associated with sexual intercourse J Emerg Med Delasobera BE Osborn SR Davis JE 0743201210.1016/j.jemermed.2009.08.01219818575 · doi ↗ · pubmed ↗