A Study on the Prevalence of Laryngopharyngeal Reflux in Saudi Arabia
Ali A Ahbail, Hamzah Alhajuj, Tariq Alharbi, Abdulrhman M Alghamdi, Hosam Amoodi, Wed M Salah, Mariam Al Sheikah

TL;DR
This study found that 31.2% of people in Saudi Arabia experience laryngopharyngeal reflux, with higher prevalence among women and those aged 36-45.
Contribution
The study provides the first comprehensive assessment of laryngopharyngeal reflux prevalence in Saudi Arabia.
Findings
LPR prevalence was 31.2% in the Saudi population.
Females and individuals aged 36-45 were more likely to have LPR.
Region of residence and other demographics showed no significant association with LPR.
Abstract
Introduction Laryngopharyngeal reflux (LPR) is a condition characterized by the backflow of gastric contents rising through the esophagus, affecting the aerodigestive tract and leading to throat symptoms such as hoarseness, chronic cough, and throat clearing. LPR is recognized as a separate condition from gastroesophageal reflux disease, despite the fact that they both involve the backflow of the stomach contents as their primary pathology. Our study aimed to evaluate the prevalence of LPR within the population of Saudi Arabia. Methods A cross-sectional study was conducted using an electronic questionnaire from August to November 2023, involving participants from all five regions of Saudi Arabia. A total of 1140 participants completed the questionnaire, which included the Reflux Symptom Index (RSI) to assess the prevalence of LPR. Results LPR was found to be prevalent in 31.2% of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
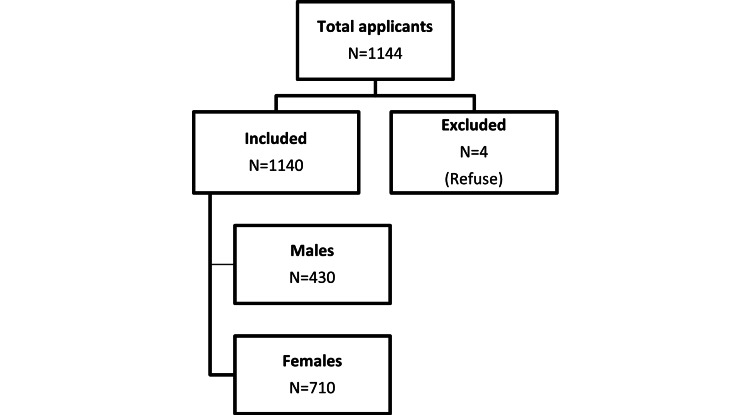 Figure 1
Figure 1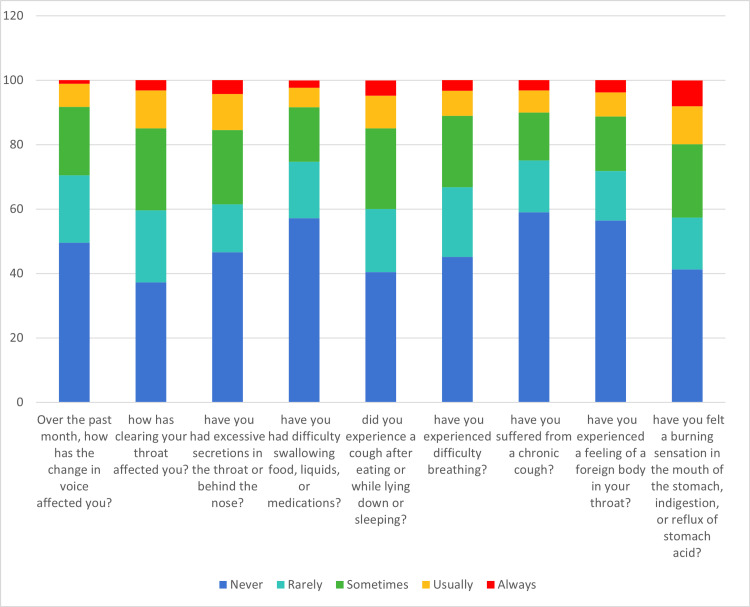 Figure 2
Figure 2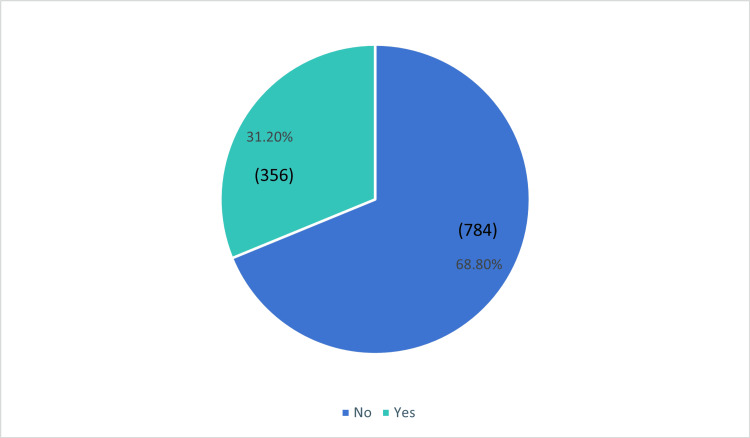 Figure 3
Figure 3| Sociodemographic data | Count | % | |
| Age | 18-25 years | 665 | 58.3% |
| 26-35 years | 164 | 14.4% | |
| 36-45 years | 124 | 10.9% | |
| 46-55 years | 92 | 8.1% | |
| More than 55 years | 95 | 8.3% | |
| Gender | Male | 430 | 37.7% |
| Female | 710 | 62.3% | |
| Nationality | Saudi | 1093 | 95.9% |
| Non-Saudi | 47 | 4.1% | |
| Region | Northern Region | 108 | 9.5% |
| Southern Region | 72 | 6.3% | |
| Eastern Region | 487 | 42.7% | |
| Western Region | 320 | 28.1% | |
| Central Region | 153 | 13.4% | |
| Marital status | Single | 697 | 61.1% |
| Married | 405 | 35.5% | |
| Widow | 9 | 0.8% | |
| Divorced | 29 | 2.5% | |
| Education | Primary | 12 | 1.1% |
| Intermediate | 23 | 2.0% | |
| High school | 336 | 29.5% | |
| Diploma | 129 | 11.3% | |
| Bachelor's | 581 | 51.0% | |
| Master's | 43 | 3.8% | |
| Ph.D | 16 | 1.4% | |
| Occupation | Unemployed | 602 | 52.8% |
| Employed | 366 | 32.1% | |
| Student | 100 | 8.8% | |
| Retired | 72 | 6.3% | |
| Income | Less than 5,000 Saudi riyals | 319 | 28.0% |
| Between 5,000 and 10,000 Saudi riyals | 320 | 28.1% | |
| Between 10,000 and 20,000 Saudi riyals | 295 | 25.9% | |
| More than 20,000 Saudi riyals | 206 | 18.1% |
| Never, n (%) | Rarely, n (%) | Sometimes, n (%) | Usually, n (%) | Always, n (%) | |
| Over the past month, how has the change in voice affected you? | 565 (49.6%) | 238 (20.9%) | 242 (21.2%) | 82 (7.2%) | 13 (1.1%) |
| During the past month, how has clearing your throat affected you? | 424 (37.2%) | 255 (22.4%) | 290 (25.4%) | 135 (11.8%) | 36 (3.2%) |
| During the past month, have you had excessive secretions in the throat or behind the nose? | 531 (46.6%) | 170 (14.9%) | 262 (23.0%) | 128 (11.2%) | 49 (4.3%) |
| During the past month, have you had difficulty swallowing food, liquids, or medications? | 651 (57.1%) | 201 (17.6%) | 193 (16.9%) | 70 (6.1%) | 25 (2.2%) |
| During the past month, did you experience a cough after eating or while lying down or sleeping? | 461 (40.4%) | 224 (19.6%) | 286 (25.1%) | 115 (10.1%) | 54 (4.7%) |
| During the past month, have you experienced difficulty breathing? | 514 (45.1%) | 247 (21.7%) | 252 (22.1%) | 89 (7.8%) | 38 (3.3%) |
| During the past month, have you suffered from a chronic cough? | 673 (59.0%) | 183 (16.1%) | 170 (14.9%) | 78 (6.8%) | 36 (3.2%) |
| During the past month, have you experienced a feeling of a foreign body in your throat? | 643 (56.4%) | 176 (15.4%) | 193 (16.9%) | 85 (7.5%) | 43 (3.8%) |
| During the past month, have you felt a burning sensation in the mouth of the stomach, indigestion, or reflux of stomach acid? | 470 (41.2%) | 185 (16.2%) | 259 (22.7%) | 135 (11.8%) | 91 (8.0%) |
| LPR status | P-value | |||||
| No | Yes | |||||
| Sociodemographic data | Count | % | Count | % | ||
| Age a | 18-25 years | 475 | 71.4% | 190 | 28.6% | 0.006 |
| 26-35 years | 118 | 72.0% | 46 | 28.0% | ||
| 36-45 years | 74 | 59.7% | 50 | 40.3% | ||
| 46-55 years | 59 | 64.1% | 33 | 35.9% | ||
| More than 55 years | 58 | 61.1% | 37 | 38.9% | ||
| Gender b | Male | 312 | 72.6% | 118 | 27.4% | 0.032 |
| Female | 472 | 66.5% | 238 | 33.5% | ||
| Nationality b | Saudi | 752 | 68.8% | 341 | 31.2% | 0.917 |
| Non-Saudi | 32 | 68.1% | 15 | 31.9% | ||
| Region a | Northern Region | 75 | 69.4% | 33 | 30.6% | 0.286 |
| Southern Region | 40 | 55.6% | 32 | 44.4% | ||
| Eastern Region | 363 | 74.5% | 124 | 25.5% | ||
| Western Region | 200 | 62.5% | 120 | 37.5% | ||
| Central Region | 106 | 69.3% | 47 | 30.7% | ||
| Marital status a | Single | 498 | 71.4% | 199 | 28.6% | 0.013 |
| Married | 263 | 64.9% | 142 | 35.1% | ||
| Widow | 3 | 33.3% | 6 | 66.7% | ||
| Divorced | 20 | 69.0% | 9 | 31.0% | ||
| Education a | Primary | 5 | 41.7% | 7 | 58.3% | 0.360 |
| Intermediate | 15 | 65.2% | 8 | 34.8% | ||
| High school | 246 | 73.2% | 90 | 26.8% | ||
| Diploma | 82 | 63.6% | 47 | 36.4% | ||
| Bachelor's | 399 | 68.7% | 182 | 31.3% | ||
| Master's | 26 | 60.5% | 17 | 39.5% | ||
| Ph.D | 11 | 68.8% | 5 | 31.3% | ||
| Occupation a | Unemployed | 413 | 68.6% | 189 | 31.4% | 0.783 |
| Employed | 248 | 67.8% | 118 | 32.2% | ||
| Student | 77 | 77.0% | 23 | 23.0% | ||
| Retired | 46 | 63.9% | 26 | 36.1% | ||
| Income a | Less than 5,000 SR | 206 | 64.6% | 113 | 35.4% | 0.004 |
| Between 5,000 and 10,000 SR | 212 | 66.3% | 108 | 33.8% | ||
| Between 10,000 and 20,000 SR | 211 | 71.5% | 84 | 28.5% | ||
| More than 20,000 SR | 155 | 75.2% | 51 | 24.8% | ||
| Unstandardized coefficients | Standardized coefficients | t | Sig. | 95% CI | |||
| B | S.E. | Beta | Lower | Upper | |||
| Constant | 8.668 | 3.038 | 2.853 | 0.004 | 2.706 | 14.629 | |
| 18-25 years (Ref. Cat) | |||||||
| 26-35 years | 0.388 | 0.730 | 0.018 | 0.531 | 0.595 | -1.045 | 1.821 |
| 36-45 years | 2.244 | 0.852 | 0.092 | 2.634 | 0.009 | 0.572 | 3.916 |
| 46-55 years | 2.255 | 0.961 | 0.081 | 2.346 | 0.019 | 0.369 | 4.140 |
| More than 55 years | 4.160 | 1.184 | 0.152 | 3.512 | <0.001 | 1.836 | 6.484 |
| Male (Ref. Cat) | |||||||
| Female | 1.125 | 0.544 | 0.072 | 2.067 | 0.039 | 0.057 | 2.192 |
| Northern Region (Ref. Cat) | |||||||
| Southern Region | 2.701 | 1.145 | 0.087 | 2.358 | 0.019 | 0.454 | 4.948 |
| Eastern Region | -0.886 | 0.844 | -0.058 | -1.049 | 0.295 | -2.542 | .771 |
| Western Region | 1.015 | 0.845 | 0.060 | 1.202 | 0.230 | -0.642 | 2.672 |
| Central Region | 0.107 | 0.956 | 0.005 | 0.111 | 0.911 | -1.770 | 1.983 |
| More than 20,000 SR (Ref. Cat) | |||||||
| Less than 5,000 SR | 1.542 | 0.720 | 0.092 | 2.144 | 0.032 | 0.131 | 2.954 |
| Between 5,000 and 10,000 SR | 1.028 | 0.706 | 0.061 | 1.455 | 0.146 | -0.358 | 2.414 |
| Between 10,000 and 20,000 SR | 0.301 | 0.701 | 0.017 | 0.429 | 0.668 | -1.075 | 1.677 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Respiratory and Cough-Related Research · Helicobacter pylori-related gastroenterology studies
Introduction
Laryngopharyngeal reflux (LPR) is also known as supra-esophageal reflux, extra-esophageal reflux, or silent reflux. It refers to a disease in which there is a backflow of gastric contents that rises through the esophagus affecting the aerodigestive tract and leading to throat symptoms, specifically those of the laryngopharynx [1]. In some patients, the gastroduodenal content may even reach the nasal cavities and ears through the Eustachian tubes, which can aggravate rhinitis, sinusitis, or otitis media [2-4].
LPR is considered a distinct condition from gastroesophageal reflux disease (GERD), although they share reflux of stomach contents as their main pathology [5]. LPR typically occurs during daytime, while upright, and is not linked to obesity [6]. Patients typically present with symptoms such as post-nasal drip, sore throat, chronic cough, dysphagia, hoarseness, excessive throat mucous, repeated throat clearing, and foreign body sensation within the throat [7]. The worldwide prevalence rate of laryngopharyngeal reflux disease (LPRD) ranges from 5% to 30% [8]. It has been observed that approximately 4-10% of all ENT outpatient clinic consultations are related to manifestations of LPR [9].
In 2022, research conducted on the Indian population revealed that the prevalence rate of LPR in the population was 11%. The prevalence rate of LPR was 11.2% in females and 10.6% in males [8].
In 2021, research conducted in the Chongqing area revealed that the prevalence rate of LPR in ENT clinics was 11.90%. The prevalence rate of LPR was 11.42% in females and 12.55% in males [10].
In 2012, research conducted on the English population revealed that the mean Reflux Symptom Index (RSI) was 8.3. A total of 30% had an RSI higher than 10, and of those, 75% exhibited symptoms of GERD (r = 0.646 at p = 0.01) [7]. Saudi data are not available about the prevalence of LPR. This study mainly aims to discover the same using the RSI score. This will assist in evaluating the burden of LPR disease in Saudi Arabia.
Materials and methods
Study design, setting, and population
A cross-sectional study was conducted in Saudi Arabia from August to November 2023. The sample size of 385 patients was calculated using an online calculator for cross-sectional studies (Raosoft Sample Size Calculator, Raosoft, Inc., Seattle, WA) [11] based on the total Saudi population of 32,175,224, aiming for a 95% confidence level with a 5% confidence interval. The study targeted both males and females aged 18 to 64 years. The questionnaire was distributed and collected randomly from five regions in Saudi Arabia: the Central Region (Riyadh), Eastern Region (Dammam, Qatif, and Al-Ahsa), Western Region (Makkah, Madinah, and Jeddah), Southern Region, and Northern Region.
Data collection method
An anonymous survey was distributed through Google Forms (Google, Mountain View, CA). The responses were kept anonymous, with no identifying information included. The survey had two sections: the first asked about personal data such as age, gender, region, profession, and marital status, while the second contained questions to evaluate LPR symptoms using the RSI [12].
Reflux symptom index (RSI)
This questionnaire was used to assess LPR symptoms. The validated Arabic version of the RSI was utilized [13]. The questionnaire consisted of nine inquiries, including hoarseness, clearing your throat, excess throat mucus or postnasal drip, difficulty swallowing, coughing after eating or lying down, difficulty breathing, chronic cough, foreign body sensation in your throat, and burning sensation in the mouth or stomach (indigestion or reflux of stomach acid). Each symptom was assigned a score from 0 to 5 based on its severity. The maximum total score was 45. A diagnosis of LPR is suggested if the total score is ≥13, as proposed by Belafsky et al. [12]. The RSI questionnaire was chosen for its established validity and reliability in assessing LPR symptoms.
Statistical analysis
The study employed descriptive statistics to summarize the data, presenting counts, proportions (%), and mean values with standard deviations, as appropriate. To explore the relationship between prevalence and participants' socio-demographic characteristics, statistical analyses were conducted using the Mann-Whitney U test and the Kruskal-Wallis test. A significance level of less than 0.05 (p < 0.05) was considered statistically significant. Additionally, statistical collinearity was assessed using the Shapiro-Wilk test and Kolmogorov-Smirnov test. All statistical analyses were performed using the IBM SPSS version 28 (IBM Corp., Armonk, NY), ensuring robust and reliable results.
Ethical approval
The study was approved by the institutional review board at the University of Jeddah, with application number UJ-REC-165. Prior to participating in the questionnaire, participants provided their consent after receiving a thorough explanation of the study's purpose and procedures.
Results
Data enrollment
A total of 1144 individuals applied to participate in the study. Out of these participants, four individuals were excluded, resulting in a final sample size of 1140 participants. The reason for exclusion was individuals chose not to participate and were therefore excluded from the study (Figure 1).
Data enrollment
Sociodemographic data
Based on the sociodemographic data, the majority of participants in the study were between 18 and 25 years old (58.3%), with females representing 62.3% of the sample. The vast majority (95.9%) were Saudi nationals, primarily from the eastern (42.7%) and western (28.1%) regions. In terms of marital status, 61.1% of participants were single, while 35.5% were married. Education-wise, the largest group had a bachelor’s degree (51.0%), followed by high school graduates (29.5%). In terms of occupation, 52.8% were unemployed, 32.1% were employed, and the remaining participants were students or retired. Regarding income, 28.0% earned less than 5,000 Saudi riyals (SR), while 18.1% earned more than 20,000 SR (Table 1).
Reflux symptom index
The data indicate symptoms such as a change in voice (7.2% usually, 1.1% always), clearing the throat (11.8% usually, 3.2% always), excessive secretions (11.2% usually, 4.3% always), difficulty swallowing (6.1% usually, 2.2% always), cough after eating or lying down (10.1% usually, 4.7% always), difficulty breathing (7.8% usually, 3.3% always), chronic cough (6.8% usually, 3.2% always), foreign body sensation in the throat (7.5% usually, 3.8% always), and burning sensation in the mouth or stomach (11.8% usually, 8.0% always) (Table 2 and Figure 2).
The percentage of Reflux Symptom Index items among study participants
Prevalence of laryngopharyngeal reflux in Saudi Arabia
Based on the data, we found 68.8% of the participants did not had LPR, while 31.2% had LPR (Figure 3).
Prevalence of laryngopharyngeal reflux in Saudi Arabia
Assessment of the demographic characteristics of laryngopharyngeal reflux disease patients
Several sociodemographic factors showed a significant association with LPR status. Regarding age, there was a significant association between age groups and LPR status (p = 0.006). The data indicated that individuals in the 36-45 years age group had a higher percentage of LPR (40.3%) compared to the overall population. Furthermore, gender was also found to be significantly associated with LPR status (p = 0.032). The proportion of females with LPR (33.5%) was higher than that of males (27.4%). Marital status showed a significant association with LPR status (p = 0.013). Lastly, income was found to have a significant association with LPR status (p = 0.004). Individuals with an income of less than 5,000 SR had a higher LPR prevalence (35.4%) compared to the overall population (Table 3).
The impact of independent variables on RSI: A linear regression analysis
The linear regression analysis revealed several significant associations between the independent variables and the RSI. Among the age categories, individuals aged 36-45 years, 46-55 years, and more than 55 years have significant positive effects on the RSI compared to the reference category of 18-25 years. Specifically, there was an average increase of approximately 2.244 (p = 0.009, 95% CI: 0.572-3.916), 2.255 (p = 0.019, 95% CI: 0.369-4.140), and 4.160 (p < 0.001, 95% CI: 1.836-6.484) units in the RSI, respectively. Additionally, being female compared to male was associated with a statistically significant increase of approximately 1.125 units in the RSI (p = 0.039, 95% CI: 0.057-2.192). In terms of region, individuals from the southern region have a significant positive effect, with an average increase of around 2.701 units (p = 0.019, 95% CI: 0.454-4.948). Lastly, income categories also showed significant associations, with individuals earning less than 5,000 SR having an average increase of about 1.542 units (p = 0.032, 95% CI: 0.131-2.954) compared to the reference category of more than 20,000 SR (Table 4).
Discussion
LPR has long been understudied, and its symptoms often indicate other diagnoses of respiratory tract disease. This misjudgment may be attributed to the lack of emphasis regarding this disease in the current literature. The purpose of our study was to assess the prevalence of LPR in the general population of Saudi Arabia. Across the globe, LPR prevalence varies significantly; our study results revealed a 31.2% (356 participants) prevalence rate, meaning that 31.2% of the sample scored ≥13 on the RSI. A different Saudi study introduced by Fahad Z. Alotaibi et al. revealed yet a considerably higher prevalence rate of 51.2% (85 participants) [14]. On the lower end of the LPR prevalence spectrum, Willybroad A. Massawe et al. reported a prevalence rate of 18.4% of their sample [15]. A study conducted over 2300 individuals in India revealed an LPR prevalence rate of 11% (253 participants) [8]. This discrepancy in prevalence rate should prompt the development and introduction of more sophisticated means of diagnosis.
Age and gender were notable demographic variables that illustrated varying results when contrasted against Fahad Z. Alotaibi et al.' paper, a recent Saudi article published in this regard. More than half of our sample fell in the 18-25 years old age group, and only about 10% were 36-45 years of age. Interestingly, our study results have indicated the latter group had a higher prevalence rate of LPR compared to the younger group. This pattern, however, was unobserved in Fahad et al.'s paper, and their results showed a higher prevalence of LPR, accounting for 36.5% amongst their 21-35 years age group and only about 29.4% amongst their 36-50 years age group [14]. Moreover, their results established lower odds of increased LPR risk in their younger group compared to the 1.3 times increased odds of LPR risk in the older group [14]. We think this observation of dissimilarity ought to encourage the following: (1) closely observing and recognizing age in upcoming research while providing a sufficient sample from each age group; (2) following a standardized age grouping system for LPR data to avoid overlapping results; (3) conducting analytic studies utilizing different tools of analysis to associate/disassociate age as a risk factor of LPR. Gender, on the other hand, proceeded in the same direction across the two studies, where we established LPR to be more prevalent amongst females, and Fahad et al. stated that males had lower odds of an increased LPR risk when compared to females [14]. At the current state of literature, we are unable to draw conclusions on either age or gender. However, our observations can stimulate and or formulate new hypotheses concerning LPR.
Limitations
Our study focused on two objectives: (1) the prevalence of LPR amongst the Saudi population and (2) the occurrence rates of demographic and symptomatologic variables in LPR. Consequently, we have stumbled upon a globally dissimilar disease distribution with no rational reasoning behind such rates. This may be the case with most topics with scarce analytical data. We have also come across an apparent shortage of demographic data. Therefore, we attempted to collect as much demographic data as possible without altering sampling techniques or risking bias while merely relying on an extended duration of data collection. Unfortunately, and in a similar fashion to current literature, our study also suffers from a disproportionate age group sample, where most of our sample (58.3%, 655 participants) belong to one age group, namely, 18-25 years of age. While practically valid, this decreases the potential of future hypotheses to be generated, knowing that other groups may need to be sufficiently emphasized. Gender has also been approached similarly, yet females still overtake their male counterparts with a 62.3% occurrence rate (710 participants) of the whole sample. Our study was limited by the absence of a precise validation of LPR diagnosis, such as laryngoscopy and pH monitoring, which would have offered more concrete evidence for our findings. However, the findings from our study can still provide valuable insights and generate hypotheses for further research on LPR demographics and symptomatology.
Conclusions
LPR's burden has shown to be evident across the globe. The current inconsistency in the disease's distribution, paucity in risk-outcome results, and vague symptomatology necessitate further assessment through upcoming endeavors. Research designs with causation and or risk-determining properties can be implemented on various elements in this topic. Such endeavors are encouraged and are expected to yield a satisfactory amount of information. All in all, we aspire to alleviate this disease’s burden through adequate research to guide one's diagnostic capability and consequently provide accurate treatment options.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laryngopharyngeal reflux: an update Arch Otolaryngol Head Neck Surg Kuo CL 132019
- 2Role of pepsin and pepsinogen: linking laryngopharyngeal reflux with otitis media with effusion in children Laryngoscope Luo HN Yang QM Sheng Y 0300124201410.1002/lary.2453824284944 · doi ↗ · pubmed ↗
- 3Laryngopharyngeal reflux and chronic sinusitis Curr Allergy Asthma Rep Weldon D 19720172007 http://link.springer.com/10.1007/s 11882-007-0072-51744833110.1007/s 11882-007-0072-5 · doi ↗ · pubmed ↗
- 4Correlation between allergic rhinitis and laryngopharyngeal reflux Biomed Res Int Alharethy S Baqays A Mesallam TA Syouri F Al Wedami M Aldrees T Al Qabbani A 2951928201820182976598110.1155/2018/2951928 PMC 5885348 · doi ↗ · pubmed ↗
- 5Prevalence and clinical predictors of LPR among patients diagnosed with GERD according to the Reflux Symptom Index questionnaire Saudi J Gastroenterol Mosli M Alkhathlan B Abumohssin A 2362412420182965203210.4103/sjg.SJG_518_17PMC 6080153 · doi ↗ · pubmed ↗
- 6Patients with isolated laryngopharyngeal reflux are not obese Laryngoscope Halum SL Postma GN Johnston C Belafsky PC Koufman JA 1042104511520051593351710.1097/01.MLG.0000162656.05715.57 · doi ↗ · pubmed ↗
- 7The prevalence of laryngopharyngeal reflux in the English population Eur Arch Otorhinolaryngol Kamani T Penney S Mitra I Pothula V 2219222526920122257624310.1007/s 00405-012-2028-1 · doi ↗ · pubmed ↗
- 8Prevalence of laryngopharyngeal reflux disease in Indian population Indian J Otolaryngol Head Neck Surg Mishra P Agrawal D Chauhan K Kaushik M 187718817420223645274510.1007/s 12070-020-01882-1PMC 9701933 · doi ↗ · pubmed ↗