PYCARD gene polymorphisms and susceptibility to periodontal and coronary heart diseases
Zina Ali Daily, Batool Hassan Al-Ghurabi, Ahmed Makki Al-Qarakhli

TL;DR
This study explores how variations in the PYCARD gene are linked to increased risk of periodontal and heart diseases in an Iraqi population.
Contribution
The study identifies specific PYCARD gene polymorphisms associated with susceptibility to periodontal and coronary heart diseases in an Iraqi cohort.
Findings
T and G alleles in PYCARD SNPs were more common in patients with periodontal and heart diseases.
CT, TT, and AG genotypes in PYCARD were positively correlated with the severity of periodontal disease.
The study highlights the potential of these SNPs as genetic risk markers for both diseases in Iraq.
Abstract
Numerous studies have established a link between gene variants within the inflammasome complex and the incidence of periodontitis and cardiovascular illness across various ethnic groups. This study investigated the association between PYCARD gene polymorphism and susceptibility to periodontal disease and coronary heart disease (CHD) and their correlation with clinical periodontal indices. A total of 120 participants were enrolled, categorized into four groups: 30 healthy controls (C), 30 patients with generalized periodontitis (P), 30 patients with atherosclerotic CHD but clinically healthy periodontium (AS-C), and 30 patients with both atherosclerotic CHD and generalized periodontitis (AS-P). We recorded demographic data, collected blood samples, and measured periodontal indices, including plaque index, clinical attachment loss, bleeding on probing, and pocket depth. The genomic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
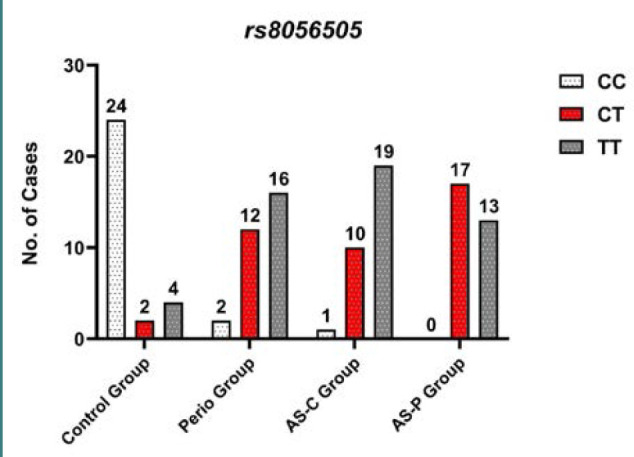 Figure 1
Figure 1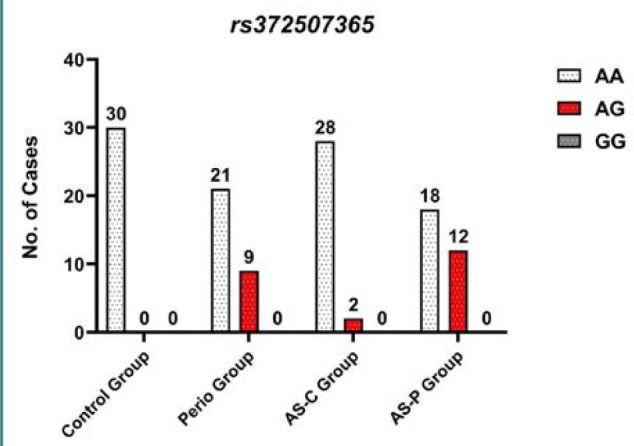 Figure 2
Figure 2| Group/ average ± SD | Control (C) | Periodontitis (P) | CHD with clinically healthy periodontium (AS-C) | CHD with periodontitis (AS-P) | Test results | |
|---|---|---|---|---|---|---|
| Age | 55 ± 6.71 | 53 ± 2.4 | 53.31 ± 3.88 | 54 ± 8.4 | 15.059 | 0.073 |
| BMI | 23.35 ± 0.85 | 23.17 ± 0.72 | 23.97 ± 0.31 | 23.24 ± 0.71 | 44.209 | 0.308 |
| Gender Male ( | 24 (80.0%) 6 (20.0%) | 24 (80.0%) 6 (20.0%) | 24 (80.0%) 6 (20.0%) | 23 (76.7%) 7 (23.3%) | 0.152 | 0.09 |
| PLI | 8.34 ± 0.84 | 53.41±0.31 | 7.35 ± 1.42 | 73.42 ± 1.73 | 403.728 | 0.02 |
| BOP | 4.93 ± 0.37 | 62.72 ± 0.38 | 6.82 ± 0.34 | 67.42 ± 1.84 | 611.493 | 0.01 |
| PPD | - | 5.12 ± 0.83 | - | 8.4 ± 0.62 | 13.534 | 0.01 |
| CAL | - | 7.12 ± 0.74 | - | 9.12 ± 0.32 | 10.057 | 0.04 |
| Genotype | Control | P | O.R (95% Cl) | AS-C | O.R (95% Cl) | AS-P | O.R (95% Cl) | |||
|---|---|---|---|---|---|---|---|---|---|---|
| CC | 24 80% | 2 7% | 0.00 | 56.0 (11.1-260.6) | 1 3% | 0.00 | 116.0 14.65-122 | 0 0% | 0.000 | 229.9 (12.335 -4285.42) |
| CT | 2 7% | 12 40% | 0.0023 | 10.72 (0.02-0.470) | 10 33% | 0.0098 | 14.29 (0.029- 0.65) | 17 57% | 0.00 | 54.33 (0.0117 -0.2757) |
| TT | 4 13% | 16 53% | 0.001 | 13.47 (0.04-0.470) | 19 64% | 0.00 | 8.91 (0.029-0.31) | 13 43% | 0.0099 | 20.12 (0.06497 - 0.720) |
| C Allele | 0.8 50% | 0.26 16 | <0.000 | 13.75 (5.51-31.65) | 0.2 12% | 0.000 | 20.0 (7.49-47.73) | 0.3 17% | 0.000 | 12.65 (5.131 -29.64) |
| T Allele | 0.2 10% | 0.74 44% | <0.000 | 13.75 (5.51-31.65) | 0.8 48% | 0.000 | 20.0 (7.49-47.73) | 0.7 43% | 0.000 | 12.65 (5.131 -29.64) |
| HWE X2 | 0.00 | 0.00 | 4.646 | 0.00 | ||||||
| >0.9999 | >0.9999 | 0.098 | >0.9999 |
| Geno-type | Control | Perio | O.R 95% Cl | AS-C | O.R (95% Cl) | AS-P | O.R 95% Cl | |||
|---|---|---|---|---|---|---|---|---|---|---|
| AA | 30 100% | 21 70% | 0.004 | 13.3 (1.761- 149.7) | 28 94% | 0.2857 | 5.3509 (0.246-116.31) | 18 60% | 0.0005 | 20.0 (2.890-220.2) |
| AG | 0 0% | 9 30% | 0.004 | 7.12 (0.006-0.567) | 2 6% | 0.2857 | 1.869 (0.008-4.062) | 12 40% | 0.0005 | 5.83 (0.0454-0.3461) |
| GG | 0 0% | 0 0% | 1.00 | 1.0 (0.019-52.039) | 0 0% | 1.00 | 1.0 (0.019- 52.03) | 0 0% | 1.00 | 1.0 (0.0192-52.0394) |
| A Allele | 1.0 60% | 0.82 51% | 0.0018 | 10.59 (1.596- 117.9) | 0.97 58% | 0.0268 | 0.195 (0.041- 0.817) | 0.8 48% | 0.4711 | 1.4 ( 0.5560-3.441) |
| G Allele | 0.0 0% | 0.18 9% | 0.0018 | 10.59 (1.596- 117.9) | 0.03 2% | 0.0268 | 0.195 (0.041- 0.817) | 0.2 12% | 0.4711 | 1.4 (0.5560-3.441) |
| HWE X2 | 0.00 | 1.61 | 2.0 | 1.45 | ||||||
| >0.9999 | 0.4456 | 0.3679 | 0.4837 |
| SNPs | PLI | BOP | PPD | CAL | |||||
|---|---|---|---|---|---|---|---|---|---|
| Patients Groups | r Value | r Value | r Value | r Value | |||||
| PYCARD C/T (rs8056505) | P group ( | 0.231 | 0.220 | 0.447 | 0.013 | 0.399 | 0.029 | 0.672 | 0.000 |
| AS-C group ( | -0.024 | 0.898 | -0.237 | 0.208 | 0.00 | 0.00 | 0.00 | 0.00 | |
| AS-P group ( | 0.198 | 0.293 | 0.498 | 0.005 | 0.463 | 0.030 | 0.504 | 0.005 | |
| PYCARD A/G (rs372507365) | P group ( | 0.093 | 0.626 | 0.278 | 0.137 | 0.329 | 0.536 | 0.364 | 0.048 |
| AS-C group ( | 0.315 | 0.090 | 0.077 | 0.685 | 0.00 | 0.00 | 0.00 | 0.00 | |
| AS-P group ( | 0.014 | 0.940 | 0.128 | 0.499 | 0.332 | 0.073 | 0.536 | 0.004 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammasome and immune disorders · Streptococcal Infections and Treatments · Oral microbiology and periodontitis research
INTRODUCTION
Periodontitis is characterized by the progressive degradation of periodontal tissue associated with the buildup of certain oral microorganisms in the dental biofilm, triggering inflammation and abnormal responses within the body. Genetics, age, and lifestyle factors influence the susceptibility to this multifactorial disease, each contributing to the risk profile [1,2]. Coronary heart disease (CHD), which can precipitate myocardial infarction, results from cardiovascular dysfunction, predominantly due to atherosclerosis. This condition is exacerbated by excessive cell death, apoptosis, and inflammation, leading to a necrotic core within atherosclerotic plaques [3]. The PYCARD gene encodes an adaptor protein essential for the recruitment of caspase enzymes. The inflammasome complex, comprising proteins and PYCARD, initiates a significant inflammatory response by interacting with caspase-1, -8, and -9, potentially leading to apoptosis [4-6]. The inflammasome is activated when membrane pores, created by cleaved Gasdermin fragments, trigger pyroptosis, which subsequently results in the release of inflammatory mediators. Pyroptosis serves an essential role in eliminating pathobionts, facilitating the extracellular release of pathogens during neutrophil-induced cell death. However, it also plays a part in the pathogenesis of various diseases by inducing severe inflammatory responses [7,8]. Genetic polymorphisms within inflammasome genes have been extensively studied [9]. However, few reports have identified a link between PYCARD gene variations and cancer diseases [10,11]. To our knowledge, there has been no investigation into the association of PYCARD gene polymorphisms and an increased susceptibility to periodontal disease and/or coronary heart disease. Therefore, the current study aimed to investigate the relationship between PYCARD SNPs and the risk of developing periodontal disease and/or CHD and to assess the correlation between PYCARD SNPs and clinical periodontal indices.
MATERIAL AND METHODS
This case-control study was conducted across multiple centers in Karbala between March and December 2022. Inclusion criteria were as follows: patients who (a) consented to participate in the study; (b) retained at least two-thirds of their total dentition, free from decay; (c) were generally healthy, except for a cardiac catheterization-confirmed diagnosis of CHD; and (d) exhibited varying severities and rates of progression of periodontal disease. Exclusion criteria included patients with (a) systemic comorbidities, (b) periodontal therapy within the past 6 months, (c) current smokers, (d) use of anti-inflammatory or immunosuppressive drugs within the last 3 months, and (e) those pregnant during the study period.
The genetic markers of the study groups, specifically the polymorphisms in their PYCARD genes, were identified based on the prevalence of periodontitis and CHD observed in the primary outcomes of the pilot study. The sample size was calculated using an odds ratio (OR) analysis on the Epitools website, aiming for an 80% power of detection at an alpha level of 0.05. The study included 120 participants, with 30 healthy controls (C), 30 patients with generalized periodontitis (P), 30 patients with atherosclerotic CHD but clinically healthy periodontium (AS-C), and 30 patients with both atherosclerotic CHD and generalized periodontitis (AS-P). Participants were men and women aged 35 to 65, with a body mass index (BMI) less than 25 kg/m^2^.
Patients with periodontitis were diagnosed following the classification by Tonetti et al. [12]. Diagnosis involved identifying individuals with a generalized extent of interdental clinical attachment loss (CAL) at two or more non-adjacent teeth or at least 3 mm of CAL on either the buccal (facial) or lingual/palatal surfaces. Additionally, a probing pocket depth (PPD) greater than 3 mm at two or more teeth was required for classification into periodontitis stages III and IV, grades B and C. These stages indicate an unstable status, characterized by either a PPD of 4 mm or more with bleeding on probing (BOP) or a PPD greater than 5 mm, with or without BOP. [13]. Clinical symptoms such as dyspnea, chest pains, electrocardiogram (ECG) changes, elevated blood lipid profiles, and diagnostic percutaneous coronary intervention revealing atheromas exceeding 70% obstruction were used for CHD diagnosis [14-17]. Demographic data were recorded, and blood samples were collected from all participants. Clinical assessments were performed using a UNC-15 probe to measure periodontal indices, including plaque index (PLI) [18], BOP [19], CAL, and PPD. Blood samples comprised 2 ml of venous blood collected in ethylenediaminetetraacetic acid (EDTA) tubes. The genomic DNA was isolated from the blood samples utilizing a ReliaPrepTM Blood gDNA Miniprep System (Promega) kit following the instructions supplied by the manufacturer. DNA concentration was quantified with a Macrogen QuantiFluor dsDNA system. The lyophilized form was dissolved in nuclease-free water to obtain a working primer solution. The primer was examined to determine its optimum degree of heat for annealing. Next, the same pair of primers was used for amplification in the template of DNA, forward, TGTAAAACGACGGCCAG TGAGATGACATGCGTGATGAG, and reverse CAGGAAACAGCTATGACGGCTCTCACTGG GTTTATTG at annealing temperatures. The PCR products were then subjected to agarose gel electrophoresis and Sanger sequencing using a Macrogen ABI3730XL Automated DNA Sequencer. Intra-examiner reliability was verified through two calibration sessions involving five patients with periodontitis, conducted one hour apart. Kappa coefficient values for BOP and PLI were 0.87 and 0.92, respectively, while intraclass correlation coefficients for PPD and CAL were 0.93 and 0.87, establishing the reliability of the study.
Statistical analysis
Data analysis was conducted using GraphPad Prism version 8.0 (GraphPad Software Inc). Means and standard deviations for each variable were calculated, and inter-group differences were assessed using one-way ANOVA. Hardy-Weinberg equilibrium was tested for the SNPs in each group, followed by an analysis of allele frequency and genotype distribution using OR. Pearson's correlation coefficient was employed to examine the association between PYCARD C/T (rs8056505) and PYCARD A/G (rs372507365) gene polymorphisms and periodontal indices.
RESULTS
Demographic and clinical findings
The demographic data and clinical characteristics of the study groups are detailed in Table 1. There were no statistically significant differences between the groups in terms of age, gender, and BMI (P > 0.05). In the four study groups, the average ages were 55 ± 6.71 for the control group (C), 53 ± 2.4 for the periodontitis group (P), 53.31 ± 3.88 for the CHD with clinically healthy periodontium group (AS-C), and 54 ± 8.4 for the CHD with periodontitis group (AS-P). The male-to-female ratio was 80:20 across groups, with an overall average BMI of 23 kg/m^2^. However, the periodontitis groups (P, AS-P) had higher values for PLI, BOP, PPD, and CAL compared to the control group (C) (Table 1).
Polymorphisms in PYCARD gene and periodontal disease and/or coronary heart disease
This study investigated the association between variations (polymorphisms) within the PYCARD gene and an increased risk of developing periodontal disease and/or CHD. Two specific polymorphisms were analyzed: PYCARD C/T (rs8056505) and PYCARD A/G (rs372507365).
PYCARD C/T (rs8056505)
The PYCARD C/T (rs8056505) polymorphism showed a significantly higher frequency of the T allele and the TT genotype in individuals with periodontal disease (P and AS-P groups) compared to the control group (C) group (Table 2, P values < 0.05). This finding is supported by the elevated odds ratios (ORs) observed for the TT genotype in the disease groups (Table 2 and Figure 1). For instance, individuals in the periodontitis group with the TT genotype were 13.47 times more likely to have the disease compared to those with the CC genotype (OR, 13.47; 95% CI, 0.04-0.470). This finding aligns with existing research suggesting a higher prevalence of the T allele in Asian populations (0.69) compared to the global average (0.6) based on the Genome Aggregation Database (gnomAD) [20,21].
PYCARD C/T (rs8056505) genotype distribution among study groups
PYCARD A/G (rs372507365)
Furthermore, the PYCARD A/G (rs372507365) polymorphism revealed a higher distribution of the AG genotype, with significant odds ratios in the P group (OR = 7.12; 95% CI, 0.0066-0.5678), the AS-C group (OR = 1.869; 95% CI, 0.0086-4.0625), and the AS-P group (OR = 5.83; 95% CI, 0.0454-0.3461), compared to the control group (C). In addition, the GG genotype of the P group had a high OR = 1.0 (0.0192 to 52.0394), with 1.0 (0.0192 to 52.0394) for the AS-C group and 1.0 (0.0192 to 52.0394) for the AS-P group compared to the C group, as illustrated in Table 3 and Figure 2. The polymorphisms of the PYCARD A/G (rs372507365) increased the G allele frequency, which was 0.18 in the P group, 0.03 in the AS-C group, and 0.2 in the AS-P group compared to the A allele of the study groups shown in Table 3. The G allele frequency among the Iraqi population is slightly higher than in other Asian countries (0.001) and the global population allele frequency (0.00), according to data from the gnomAD database. This indicates that Asian populations exhibit a broader range of allele frequencies compared to other populations. PYCARD C/T (rs8056505) and PYCARD A/G (rs372507365) distribution of genotypes had no significant differences in HWE across the study groups (Tables 2 and 3). The association between the PYCARD genes and the clinical indices of periodontal disease for the four groups is shown in Table 4.
PYCARD A/G (rs372507365) genotype distribution among study groups
The association between PYCARD genotypes and periodontal clinical indices was assessed using the Pearson correlation coefficient. There was a significant positive correlation between the PYCARD C/T (rs8056505) and BOP, PPD, and CAL in the periodontitis group (P) and the CHD group with periodontitis (AS-P), respectively. A significantly positive correlation was also observed between PYCARD A/G (rs372507365) and CAL in the periodontitis group (P) and the CHD group with periodontitis (AS-P), respectively.
DISCUSSION
This study investigated the association between PYCARD gene polymorphisms (C/T rs8056505 and A/G rs372507365) and susceptibility to periodontal disease and coronary heart disease in an Iraqi population. The findings suggest that specific genotypes in these polymorphisms might be linked to an increased risk of these diseases. Furthermore, this study established a significant association between PYCARD gene polymorphisms and periodontal indices. The data in Table 2 shows that individuals with the TT genotype of the PYCARD C/T (rs8056505) polymorphism are significantly more likely to have periodontitis, CHD and CHD with periodontitis compared to those with the CC genotype (OR = 13.47; 95% CI, 0.04-0.470), (OR = 8.91; 95% CI, 0.029-0.31) and (OR = 20.12; 95% CI, 0.06497-0.720) respectively. C allele carriers have a lower chance of contracting both diseases, indicating that the PYCARD C/T (rs8056505) SNP is linked to an elevated risk of periodontal disease and atherosclerotic CHD. This suggests that individuals with the TT genotype are over 13 times more likely to have periodontitis, over 8 times more likely to have CHD, and over 20 times more likely to have CHD with periodontitis compared to those with the CC genotype. The AG genotype of the PYCARD A/G (rs372507365) polymorphism revealed a statistically significant association with periodontal disease and atherosclerotic CHD with periodontitis susceptibility (OR = 7.12; 95% CI, 0.0066-0.5678) and (OR = 5.83; 95% CI, 0.004540-0.3461) in this study population as compared to the AA genotype (Table 3). A allele carriers had a lower chance of contracting both diseases. This suggests the AG genotype is associated with an increased risk of periodontal disease and atherosclerotic CHD.
In summary, this study investigated PYCARD gene variations SNPs located in the promoter region, a crucial area of the 5' untranslated region (UTR) of DNA that contains regulatory elements like the proximal promoter. These regulatory elements influence gene expression in immune cells and tissue-resident cells. The SNPs might disrupt these elements, potentially leading to epigenetic modifier loss and altered expression of PYCARD proteins. This, in turn, could be linked to pyroptosis, a form of programmed cell death. Interestingly, similar associations between PYCARD variations and altered gene expression have been observed in various cancers, including lung cancer [22], breast cancer [23], schwannoma tumor [4], prostate cancer [24], and pancreatic ductal adenocarcinoma [10]. Polymorphisms in the PYCARD gene appear to be associated with slightly higher frequencies of T and G allele changes than those found in Asians and the global population of allele frequency based on the gnomAD [25]. The study identified specific PYCARD gene variations (high T and G allele frequencies) associated with an increased risk of periodontal and cardiovascular diseases in the Iraqi population. The HWE analysis of PYCARD SNPs revealed no significant deviation, confirming the reliability of the genotype and allele frequencies across each study group (P > 0.05). In this study, periodontal indices were greater in the periodontitis groups than in the control and AS-C groups. This finding aligns with research indicating that plaque biofilms, producing a variety of bacterial by-products, trigger inflammation and accelerate the degradation of periodontal tissues [14,17,26,27,28]. In the current study, PYCARD gene polymorphisms were positively associated with periodontal parameters with and without atheromatous CHD. This association may indicate the presence of fundamental inflammation and molecular processes in the pathophysiology of both diseases. This study established a relationship between PYCARD gene polymorphisms and the development and severity of disease, suggesting that further investigation into these links could enhance our understanding of various diseases. The exclusion of prevalent risk factors for both periodontitis and cardiovascular disease, such as obesity, diabetes, smoking, and hypertension, was done in order to avert bias. To our knowledge, this is the first study to explore the association of a PYCARD genetic variation with susceptibility to periodontal disease, regardless of the presence or absence of coronary heart disease.
CONCLUSION
Alterations in the T and G alleles within the TT, CT, and AG genotypes of the PYCARD gene were significantly associated with periodontitis and coronary heart disease, revealing complex genetic variations in the Iraqi population. The findings suggest that these specific PYCARD variations might influence susceptibility to both diseases, potentially through shared underlying pathways.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Laine ML Crielaard W Loos BG Genetic susceptibility to periodontitis Periodontol. 2000201258376810.1111/j.1600-0757.2011.00415.x 22133366 · doi ↗ · pubmed ↗
- 2Saliem SS Bede SY Cooper PR Abdulkareem AA Milward MR Abdullah BH Pathogenesis of periodontitis-A potential role for epithelial-mesenchymal transition Jpn Dent Sci Rev 20225826827810.1016/j.jdsr.2022.09.00136159185 PMC 9489739 · doi ↗ · pubmed ↗
- 3Herrera D Molina A Buhlin K Klinge B Periodontal diseases and association with atherosclerotic disease Periodontol 20002020831668910.1111/prd.1230232385870 · doi ↗ · pubmed ↗
- 4Ahmed SG Abdelnabi A Maguire CA Doha M Sagers J E Gene therapy with apoptosis-associated speck-like protein, a newly described schwannoma tumor suppressor, inhibits schwannoma growth in vivo J Neuro Oncol 201921785486610.1093/neuonc/noz 065PMC 662064130977509 · doi ↗ · pubmed ↗
- 5Mahmooda AA Abbas RF Association between Caspase-1, TNF-α Salivary Level and Their Diagnostic Potential to Discriminate Periodontitis from Healthy Control Oral Health Prev Dent 20232161683679477810.3290/j.ohpd.b 3904349 PMC 11619825 · doi ↗ · pubmed ↗
- 6Al-Ghurabi BH The Role of Soluble TLR-2 in the Immunopathogenesis of Gingivitis Int Med J 20212813739
- 7Li X Zhang P Yin Z Xu F Yang ZH Jin J Caspase-1 and Gasdermin D Afford the Optimal Targets with Distinct Switching Strategies in NLRP 1b Inflammasome-Induced Cell Death Research (Wash D C)20222022983834110.34133/2022/983834135958114 PMC 9343085 · doi ↗ · pubmed ↗
- 8Chen PC Jiang Z Jiang Q Dai W Shao Q Chen Q Wang Y Yang G Caspase-3 and gasdermin E detection in peri-implantitis J J Biochim Biophys Acta Mol Basis Dis 202118671110.1016/j.bbadis.2021.16621734273529 · doi ↗ · pubmed ↗