Valuable Predictors for Non-measurability of Fractional Flow Reserve Derived From Coronary Computed Tomography Angiography
Hideaki Nonaka, Kazuyuki Yahagi, Kota Komiyama, Yuki Gonda, Yu Horiuchi, Masahiko Asami, Hitomi Yuzawa, Jun Tanaka, Jiro Aoki, Kengo Tanabe

TL;DR
This study identifies heart rate and coronary calcium scores as predictors of when FFRCT cannot be measured, offering ways to improve diagnostic accuracy.
Contribution
The study identifies heart rate and coronary calcium scores as independent predictors of FFRCT non-measurability and provides threshold values for clinical guidance.
Findings
FFRCT analysis was non-measurable in 6.8% of patients.
Higher heart rate and coronary calcium scores were independently associated with non-measurability.
Combining heart rate and calcium score thresholds provides a high negative predictive value for non-measurability.
Abstract
Background The fractional flow reserve (FFR) derived from coronary computed tomography (CT) angiography (FFRCT) is a variable tool for coronary disease diagnosis that non-invasively provides the value of FFR. It can add physiological information to coronary CT angiography (CCTA) and reduce unnecessary invasive coronary angiography (CAG). However, it cannot be analyzed in some cases, which is also called “non-measurability.” While FFRCT has become globally widespread, the current data on non-measurability are lacking. This study aimed to determine the rate of non-measurability and identify predictors thereof in routine clinical settings to explore potential approaches to reduce the non-measurability rate. Methods and results This retrospective observational single-center study included consecutive patients who underwent FFRCTanalysis in Japan. The mean age of the overall population…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
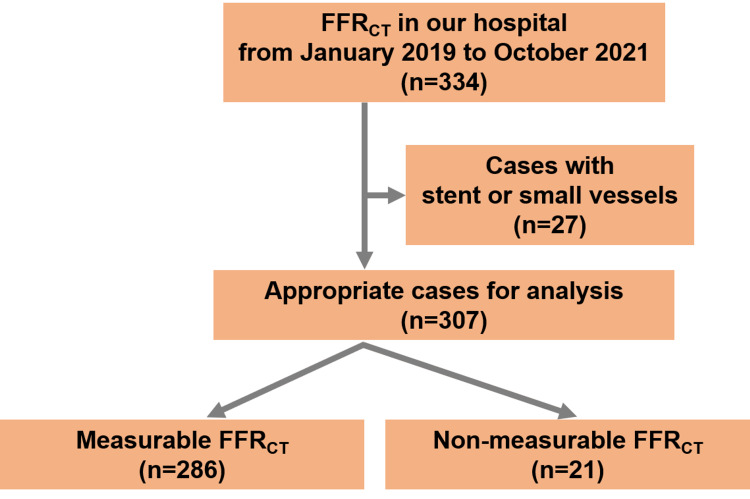 Figure 1
Figure 1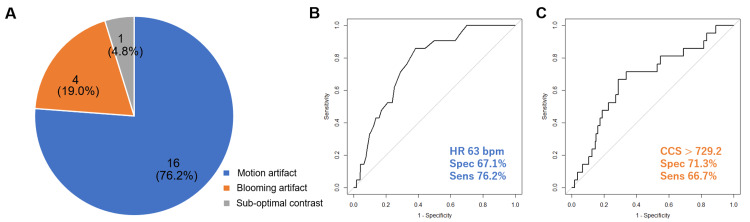 Figure 2
Figure 2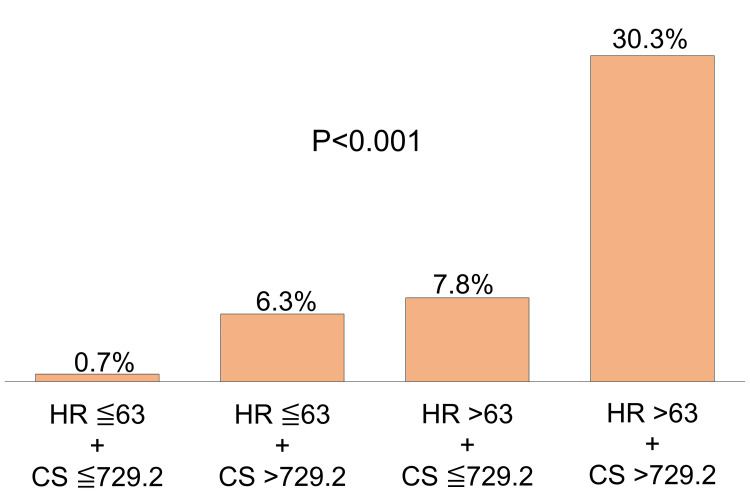 Figure 3
Figure 3| Overall (n=307) | Measurable FFRCT (n=286) | Non-measurable FFRCT (n=21) | P value | |
| Age (y) | 71.3 ± 10.6 | 71.0 ± 10.6 | 74.4 ± 10.8 | 0.163 |
| Female (%) | 99 (32.2) | 92 (32.2) | 7 (33.3) | 1.000 |
| BMI (kg/m2) | 24.9± 15.2 | 25.1 ± 15.7 | 22.4 ± 0.3.7 | 0.426 |
| Smoking history (%) | 132 (43.0) | 125 (43.7) | 7 (33.3) | 0.485 |
| Dyslipidemia (%) | 180 (58.6) | 169 (59.1) | 11 (52.4) | 0.709 |
| Diabetes mellitus (%) | 83 (27.0) | 76 (26.6) | 7 (33.3) | 0.675 |
| Hypertension (%) | 213 (69.4) | 201 (70.3) | 12 (57.1) | 0.310 |
| Hemodialysis (%) | 16 (5.2) | 15 (5.2) | 1 (4.8) | 1.000 |
| Previous MI | 5 (1.6) | 5 (1.9) | 0 (0) | 1.000 |
| TG (mg/dL) | 140.1 ± 121.8 | 143.1 ± 124.5 | 100.1 ± 65.7 | 0.119 |
| HDL-C (mg/dL) | 59.3 ± 24.1 | 59.5 ± 24.4 | 56.3 ± 20.1 | 0.648 |
| TC (mg/dL) | 175.1 ± 70.0 | 175.2 ± 70.5 | 173.6 ± 65.5 | 0.917 |
| eGFR (mL/min/1.73m2) | 61.2 ± 20.2 | 61.3 ± 20.4 | 60.3 ± 18.2 | 0.879 |
| HbA1c (%) | 6.2 ± 3.2 | 6.3 ± 3.2 | 5.6 ± 2.6 | 0.311 |
| NT-proBNP (pg/mL) | 102.0 (35.5, 238.5) | 97.0 (35.3, 241.0) | 124.0 (47.0, 209.0) | 0.836 |
| Heart rate at scan (bpm) | 61.6 ± 11.1 | 61.0 ± 11.1 | 69.6 ± 8.9 | 0.001 |
| Total calcium score | 356.5 (108.8, 899.8) | 322.9 (100.7, 850.0) | 931.2 (290.8, 1451.3) | 0.008 |
| Amount of contrast (mL) | 43.2 ± 13.6 | 43.1 ± 13.8 | 44.9 ± 11.0 | 0.556 |
| Ejection fraction (%) | 63.7 ± 11.4 | 64.1 ± 10.9 | 60.0 ± 16.3 | 0.047 |
| Use of β-blocker (%) | 138 (45.0) | 126 (44.1) | 12 (57.1) | 0.349 |
| Use of nitroglycerin (%) | 267 (87.0) | 247 (86.4) | 20 (95.2) | 0.406 |
| AF at scan (%) | 26 (8.5) | 24 (8.4) | 2 (9.5) | 1.000 |
| Age (y) | Sex | HR (bpm) | CCS | Non-measurable vessel | The reason for FFRCT non-measurability |
| 75 | M | 57 | 48.7 | ALL | Sub-optimal contrast |
| 88 | M | 65 | 2192.0 | RCA | Blooming artifact |
| 75 | F | 64 | 931.2 | RCA | Blooming artifact |
| 73 | F | 63 | 1299.5 | RCA | Blooming artifact |
| 79 | M | 56 | 789.2 | LMT | Blooming artifact |
| 78 | M | 68 | 260.7 | RCA | Motion artifact |
| 52 | M | 80 | 1657.3 | RCA | Motion artifact |
| 69 | F | 66 | 1212.7 | RCA | Motion artifact |
| 86 | M | 80 | 1383.5 | RCA | Motion artifact |
| 64 | F | 72 | 7.2 | RCA | Motion artifact |
| 81 | F | 95 | 606.3 | RCA | Motion artifact |
| 59 | M | 76 | 149.2 | RCA | Motion artifact |
| 90 | F | 66 | 290.8 | RCA | Motion artifact |
| 83 | M | 63 | 743.5 | RCA | Motion artifact |
| 78 | M | 61 | 1845.1 | RCA | Motion artifact |
| 73 | M | 74 | 731.6 | RCA | Motion artifact |
| 74 | M | 74 | 34.5 | ALL | Motion artifact |
| 53 | M | 75 | 3451.4 | ALL | Motion artifact |
| 73 | M | 69 | 1154.3 | LAD | Motion artifact |
| 90 | F | 65 | 1451.3 | LAD | Motion artifact |
| 69 | M | 71 | 2847.4 | LCX | Motion artifact |
| Univariable analysis | Multivariable analysis | |||
| Variable | Odds ratio | P value | Odds ratio | Odds ratio |
| Heart rate | 1.004 (1.001-1.007] | < 0.01 | 1.004 (1.001-1.006) | < 0.01 |
| Coronary calcium score | 1.0005 (1.0001-1.0009) | 0.03 | 1.0001 (0.9998-1.0004) | 0.051 |
| Amount of contrast | 1.00 (0.99-1.002) | 0.56 | ||
| Ejection fraction | 0.997 (0.995-0.99) | 0.046 | ||
| Use of β-blocker | 1.03 (0.97-1.09) | 0.25 | ||
| Use of nitroglycerin | 1.05 (0.97-1.14 | 0.24 | ||
| AF at scan | 0.93 (0.84-1.03) | 0.15 | ||
| Sensitivity (%) | Specificity (%) | PPV (%) | NPV (%) | Accuracy (%) | |
| HR >63 bpm | 76.2 | 67.1 | 14.5 | 97.5 | 67.8 |
| CCS >729.2 | 66.7 | 71.3 | 14.6 | 96.7 | 71.0 |
| HR >63 + CCS >729.2 | 47.6 | 92.0 | 30.3 | 96.0 | 88.9 |
| HR >63 or CCS >729.2 | 95.2 | 46.5 | 11.6 | 99.3 | 49.8 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Imaging and Diagnostics · Coronary Interventions and Diagnostics · Advanced MRI Techniques and Applications
Introduction
Coronary artery disease remains a common problem in modern clinical practice [1] and is a leading cause of mortality [2,3]. Invasive fractional flow reserve (FFR), providing us with the physiological severity of coronary stenosis, has conventionally been recommended to assess the need for therapeutic intervention [2,4]. Recently, a non-invasive method to calculate FFR via coronary computed tomographic angiography (CCTA) image has been developed, called "FFRCT" [3]. It employs computational fluid dynamics and image-based modeling, permitting the determination of rest and hyperemic coronary flow and pressure from CCTA scans, without additional imaging, modification of acquisition protocols, or administration of medications. In clinical settings, this advanced technique enables us to gain FFR value non-invasively along with CCTA and to reduce unnecessary invasive coronary angiography, potentially decreasing the burden on patients and healthcare costs [5-8]. The previous multicentre studies have demonstrated its high diagnostic accuracy and discrimination with invasive FFR as the reference standard (area under the curve: 0.9) [6] and its high predictive value for fewer adverse cardiac events [7]. Although the utility of FFRCT has been established and is becoming indispensable in current clinical settings, the analysis can be rejected from the hub site of analysis at times, which is also called “non-measurability”, and its rate was previously reported as 8.4% in 2019 [9]. Although the analysis software has significantly advanced thereafter, the updated data on the non-measurability have not been reported. In this study, we aimed to determine the current rate of non-measurability and identify predictors thereof in routine clinical settings to explore potential approaches to reduce the non-measurability rate.
Materials and methods
Study design and population
The study retrospectively analyzed 334 consecutive cases using FFRCT analysis at a Japanese institution from January 2019 to October 2021 (Figure 1), detailing patient selection criteria, imaging protocols, and analytic techniques. The decision to refer patients for FFRCT analysis was made by the physician interpreting the CCTA based on the abnormalities in electrocardiogram, echocardiography, or chest symptoms suspected of coronary artery stenosis. Among those patients, those with a previous history of revascularization (percutaneous coronary intervention with a stent or a coronary artery bypass graft; n=26) and small vessels (≤1.8 mm; n=1) were excluded, as in previous studies [9]. This is because revascularization history and small vessels are actually not recommended for FFR-CT analysis at HeartFlow Inc. (Redwood City, CA), which is the site where our FFR-CT analysis was conducted. The present study was conducted in accordance with the Declaration of Helsinki and approved by the local institutional review committee on human research (Mitsui Memorial Hospital Ethics Committee No. C26). The study details were explained to all participants when obtaining consent for the CCTA scan and FFRCT analysis, and informed consent for this study was obtained in an opt-out manner.
The flowchart of the patient selectionA flowchart demonstrates the selection process of the study population.FFRCT, fractional flow reserve derived from coronary computed tomography angiography
CCTA acquisition, reconstruction, and analysis
CCTA was conducted using single-source computed tomography (CT) scanners with 320 detector rows (Aqualion One, Canon Medical Systems, Tochigi, Japan) based on a previously described protocol [10]. Scanning parameters were as follows: collimation of 320 rows x 0.5 mm, rotation time of 350-400 ms, and tube voltage of 120 kV. The tube current (270-400 mA) was chosen based on the standard deviation of the noise level measured on the CT projection radiographs. Electrocardiogram-gated non-enhanced scans were obtained, followed by contrast-enhanced scans using Iopamiron 370 mg/mL injected at a rate of 4.0-5.0 mL/s. The scanner’s “arrhythmia rejection” software automatically removed irregular beats using the multi-segment acquisition technique. We semi-automatically determined the appropriate cardiac phase with minimal cardiac motion for the CT axial image reconstruction using the Phase-NAVI scanner software (Canon Medical Systems, Tochigi, Japan). All data acquired with 0.25-mm-thick slices were reconstructed using a standard kernel of FC04. Oral or intravenous beta-blockers, or both, were administered to achieve a heart rate (HR) of ≤60 beats/min [11], and sublingual nitroglycerin was administered to patients without any contraindications. The coronary artery calcium score (CCS) was calculated using a workstation (Ziostation2, Ziosoft, Tokyo, Japan) and expressed using the previously reported Agatston score [12].
FFRCT analysis
All FFRCT analyses were performed at HeartFlow Inc. (Redwood City, CA) as previously described [13]. Their software applies computational fluid dynamics and deep-learning image-based modeling to estimate rest and hyperaemic coronary flow and pressure from CCTA. Non-measurability in the FFRCT analysis was defined as an inability to perform quantitative analysis with FFRCT [14] and was determined by HeartFlow Inc.
Statistical analysis
Categorical variables were expressed as numbers and percentages (%), and continuous variables were expressed as mean±standard deviation (SD) or median and interquartile range (IQR) (25th to 75th percentile) according to their distribution. Assessment of normality for continuous data was performed using the Kolmogorov-Smirnov test. Categorical variables were analyzed using the chi-square or Fisher’s exact test, and differences in continuous variables were analyzed using a two-sided Student’s t-test or the Wilcoxon rank test. Binary logistic regression was used to assess the association between baseline covariates and non-measurability in FFRCT analysis (results were presented as odds ratio (OR) and 95% confidence interval (CI)). In order to predict the non-measurability, the optimal cut-off value with sensitivity and specificity was determined by the receiver operating characteristic (ROC) curve analysis. Variables with p<0.05 were considered to indicate a significant difference. All analyses were performed using the R software (version 4.1.2; R Foundation for Statistical Computing, Vienna, Austria). To control for type I error inflation due to multiple comparisons, we employed the Benjamini-Hochberg procedure. The false discovery rate was set at 5%.
Preprint disclosure
This article was previously posted to the Research Square preprint server (doi.org/10.21203/rs.3.rs-3211999/v1) on 2nd August 2023.
Results
Patient characteristics
We analyzed 307 cases in Japan, and their main clinical characteristics are summarized in Table 1. The mean age was 71.3 ± 10.6 years old. The rate of males (67.8%), smokers (43.0%), dyslipidemia (58.6%), and hypertension (69.4) were relatively high in the overall population. Non-measurability occurred in 21 (6.8%) patients and was associated with a higher HR at CT scanning (p < 0.01), higher CCS (p < 0.01), and lower ejection fraction (p = 0.047) than those with their FFRCT measurable. The rates of beta-blockers, nitroglycerin use, and atrial fibrillation were comparable between the two groups. A FFRCT of ≤0.8 was seen in 47.6% of patients with a measurable FFRCT, and a FFRCT of ≤0.8 was seen in 23.1% of all vessels with a measurable FFRCT.
Reason for non-measurability
According to the analysis by HeartFlow Inc., motion artifact (n=16; 76.2%) and blooming artifact (n=4; 19.0%) were major reasons for non-measurability (Figure 2A), followed by sub-optimal contrast (n=1; 4.8%). Data from all 21 cases with rejected FFRCT analysis are presented in Table 2. The right coronary artery (RCA) (n=16; 76.2%) was the most common non-measurable vessel.
The reasons for FFRCT non-measurability (A) and the ROC curve for FFRCT non-measurability (B,C)The pie chart (A) shows reasons for FFRCT non-measurability. The major reasons were motion and blooming artifacts. The ROC curve (B) shows the predictive value of HR for non-measurability (cut-off value, 63 bpm; AUC: 0.77; sensitivity: 67.1%; specificity: 76.2%). The other ROC curve (C) shows the predictive value of CCS for non-measurability (cut-off value, 729.2; AUC: 0.67; sensitivity: 71.3%; specificity: 66.7%)FFRCT, fractional flow reserve derived from coronary computed tomography angiography; ROC, receiver-operating characteristic; HR, heart rate; AUC, area under the curve; CCS, coronary artery calcium score
Factors associated with non-measurability
Univariate logistic regression analyses revealed that HR at CT examination (OR: 1.004; 95% CI: 1.001-1.007; p < 0.01) and CCS (OR: 1.00; 95% CI: 1.00-1.00; p = 0.03) were significant factors associated with non-measurability. Although we additionally analyzed other variables, including the amount of contrast, use of β-blocker or nitroglycerin, and AF, no significance was observed. Due to the small number of events, we conducted multivariate logistic regression analysis only including HR and CCS, and HR was the independent factor for FFRCT non-measurability (Table 3) (OR: 1.004; 95% CI: 1.001-1.006; p < 0.01). Based on the ROC curve analysis, the optimal cut-off for HR to predict non-measurability was 63 bpm, with a specificity and sensitivity of 67.1% and 76.2%, respectively (Figure 2B). The area under the ROC curve (AUC) was 0.77 (95% CI: 0.68-0.85). The CCS’s optimal cut-off to predict non-measurability was 729.2 with a specificity and sensitivity of 71.3% and 66.7%, respectively (Figure 2C), and the AUC was 0.67 (95% CI: 0.55-0.79).
Predictive features of HR and CCS
Based on HR and CCS, which were the factors associated with artifact and non-measurability, we classified all cases into four groups and investigated the occupation of non-measurability as follows: low HR (≤ 63) and low CCS (≤ 729.2) (n = 124); low HR (≤ 63) and high CCS (> 729.2) (n = 56); high HR (> 63) and low CCS (≤ 729.2) (n = 87); and high HR (> 63) and high CCS (> 729.2) (n = 40) (Figure 3). Of the four groups, the percentage of non-measurability was the highest in patients with a high HR and high CCS (30.3%), whereas the number of cases with a rejected FFRCT analysis was only one (0.7%) (p < 0.001) in patients with low HR and low CCS. The sensitivity, specificity, positive predictive value, and negative predictive value (NPV) of various characteristics in combination or independently are provided in Table 4. When either the HR was > 63 bpm or the CCS was > 729.2, sensitivity was 95.2% and NPV was 99.3%.
The bar graph of FFRCT non-measurability in each group divided by HR and CCSThe FFRCT analysis was most frequently rejected (30.3%) in the group with both a high HR (>63 bpm) and a high CCS (> 729.2), although that was only 0.7% in groups with a low HR (≤ 63 bpm) and a low CCS (≤ 729.2) (p < 0.01).HR, heart rate; CCS, coronary artery calcium score; FFRCT, fractional flow reserve derived from coronary computed tomography angiography
Discussion
The main findings of our study are that (1) the non-measurability rate due to inadequate image quality was 6.8%, (2) HR was an independent predictor of non-measurability, (3) the optimal HR to complete FFRCT analysis was < 63 bpm, and (4) cases with either an HR of > 63 bpm or a CCS of > 729.2 had extremely high NPV for non-measurability. The points to be emphasized are that HR and CCS are significant predictors associated with non-measurability and notably, considering that we can intervene on HR alone, in cases with severe calcification (CCS of > 729.2), adjustment of HR is particularly recommended because both HR of > 63 bpm and CCS of > 729.2 shows the specificity of 92.0% for non-measurability.
The rate of non-measurability in the current study was lower than that reported in previous studies (8.4-33%) [6,9,14-16]. We considered the major reason as the use of a wide-detector CT scanner. Previous studies have revealed that motion artifacts are closely associated with FFRCT non-measurability [6,9,14], and wide-coverage scanner technology can reduce the occurrence of motion artifacts as they allow whole-heart acquisition for a single beat and can provide relatively accurate images even in cases with a higher HR and arrhythmia [17-19]. In our institution, all CCTA examinations were performed with a 320-detector row CT scanner. In previous studies, the wide-coverage (≥ 16 cm) row scanner was only used in 17-46% of the study population [9,15]. This may be the main reason for the lower rate of non-measurability. Selecting a wide-detector scanner can be one of the methods to obtain optimal FFRCT values, especially in cases with tachycardia or arrhythmias.
Another conceivable reason for the lower non-measurability rate is the thinner CT section. The thickness of the CT section has also been reported as another common predictor for non-measurability in a large cohort study, with thinner sections decreasing the rates of non-measurability [9]. In our institution, all CT data were reconstructed with a 0.25 mm slice thickness, which was thinner than that reported in previous studies (0.63 ± 0.10 mm) [9]. Reconstructing CT images with thinner sections may also reduce image noise [20] and may also be beneficial to increase the rate of completion of FFRCT analysis.
The main reason for the rejection of FFRCT analysis in the present study was motion artifacts, which were the same as those in most previous studies [6,9,15]. Although CT hardware and FFRCT analysis software have improved gradually, HR remains the strongest predictor for non-measurability. To reduce motion artifacts, the Society of Cardiovascular Computed Tomography (SCCT) guidelines recommend HR control under 60 bpm on CT examination [11]. The optimal HR revealed in our analysis (≤ 63 bpm) was very close to the target HR to reduce motion artifacts in CCTA (60 bpm). This may indicate that the FFRCT analysis cannot be accomplished in place of motion artifacts. Therefore, we need to reduce the HR to below 60 bpm during CT scanning. To decrease HR, beta-blocker administration is also recommended [11]. However, in clinical practice, ideal HR control cannot always be accomplished as patients who require CCTA sometimes have aortic stenosis, a low left ventricular ejection fraction, and bronchial asthma, which all are factors that make it difficult for clinicians to use beta-blockers. In fact, the rate of beta-blocker use in this real-world clinical study (45.0%) was lower than in previous studies (72.0-78.0%) [6,21], which were dedicated FFRCT studies with institutions receiving specific FFRCT training and feedback. Thus, in clinical practice, using a wide-detector CT scanner and reconstructing images of better quality may be proper options for obtaining FFRCT values, especially in patients with a higher HR.
In addition, the present study showed that the RCA was the most common non-measurable vessel resulting from motion artifacts. We considered the reason was that the RCA moves in the perpendicular direction to the plane of the CT scan [22].
Apart from motion artifact, blooming artifact was the second cause of non-measurability in our study. However, the number of cases with non-measurability due to blooming artifacts was relatively small. In fact, FFRCT analysis was accomplished in 85.4% of patients with a high CCS (> 729.2), which indicated that FFRCT could be measured even in severely calcified coronary arteries. Basically, in the FFRCT computation processes, luminal dimensions are assessed along the entire length of each vessel using segmentation methods, which can correct calcium blooming [23]. Moreover, it has been demonstrated that FFRCT can provide superior diagnostic performance than CCTA alone in cases with a high CCS [24]. In clinical practice, poor CT images due to massive calcification could make physicians hesitant to undertake FFRCT analysis. However, research has shown that FFRCT can be analyzed completely and provide significant diagnostic performance even in patients with a high CCS.
Finally, we discuss the utility of CCS and HR in predicting the feasibility of FFRCT analysis based on Table 4. For CCS, even at values greater than 729.2, the positive predictive value is only 14.6%, indicating that FFRCT measurement is possible in many cases, as mentioned above. However, if CCS is below 729.2, FFRCT measurement is feasible with a very high likelihood considering a negative predictive value of 96.7%. Additionally, in cases with CCS greater than 729.2, and an HR at CT scan greater than 63, we can expect a very high probability of FFRCT non-measurement considering the specificity of 92.0%. Therefore, it is recommended to keep the HR below 63, particularly in cases of severe calcification. Conversely, as indicated by a sensitivity of 95.2% and a negative predictive value of 99.3%, if the calcification is relatively minor (CCS ≤ 729.2) and HR is controlled within the range of under 63, FFRCT analysis is likely feasible in almost all cases. The same can be applied to HR. FFRCT measurement is possible with an HR greater than 63 bpm, but a lower HR (≤ 63 bpm) increases the probability of successful FFRCT analysis. To note, considering that we can intervene on HR alone, in cases with severe calcification, adjustment of HR is particularly recommended.
Limitations
This study had several limitations. First, the present study was a retrospective analysis of data collected from a single center, representing a small cohort of FFRCT cases in Japan. Thus, selection biases are inevitable, and our study was underpowered to make strong statements. Validation in large multicenter prospective studies is required. The second limitation was referral bias. The decision to proceed to FFRCT analysis was made by each physician interpreting the CCTA, and referral bias was likely present. Third, we did not investigate all factors that had a significant association with non-measurability in previous studies, including temporal resolution, aorta contrast opacification, reconstructed field of view, and atheroma volume. Since these can be factors associated with CCTA image quality and confounders for non-measurability, future studies will be required to collect these variables.
Conclusions
The rate of non-measurability of FFRCT was 6.8% in our hospital. HR and CCS were important factors in acquiring FFRCT values and in cases with both HR and CCS below a specified threshold, the likelihood of ruling out non-measurability could be significantly high. Particularly in cases with severe calcification (CCS > 729.2), adjustment of HR to under 63 bpm is highly recommended considering that the specificity of both HR > 63 bpm and CCS > 729.2 for non-measurablity was 92%. Furthermore, using a wide-detector CT scanner and reconstructing images of better quality may be proper options for obtaining FFRCT values, especially in patients with a higher HR. While technological advancements in CCTA machines and FFRCT analysis software are expected, further investigation in a larger-scale cohort will help reduce the non-measurability rate more by elucidating the valuable predictive factors that we can adjust.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prognosis of patients with stable coronary artery disease (from the CORONOR study)Am J Cardiol Bauters C Deneve M Tricot O Meurice T Lamblin N 114211451132014
- 22021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR guideline for the evaluation and diagnosis of chest pain: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines Circulation Gulati M Levy PD Mukherjee D 0454144202110.1161/CIR.000000000000102934709879 · doi ↗ · pubmed ↗
- 3JCS 2022 guideline focused update on diagnosis and treatment in patients with stable coronary artery disease Circ J Nakano S Kohsaka S Chikamori T 8829158620223528340110.1253/circj.CJ-21-1041 · doi ↗ · pubmed ↗
- 4Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses N Engl J Med Pijls NH De Bruyne B Peels K Van Der Voort PH Bonnier HJ Bartunek J Koolen JJ Koolen JJ 170317083341996863751510.1056/NEJM 199606273342604 · doi ↗ · pubmed ↗
- 5Cost analysis of non-invasive fractional flow reserve derived from coronary computed tomographic angiography in Japan Cardiovasc Interv Ther Kimura T Shiomi H Kuribayashi S 38443020152503018010.1007/s 12928-014-0285-1PMC 4573651 · doi ↗ · pubmed ↗
- 6Diagnostic performance of noninvasive fractional flow reserve derived from coronary computed tomography angiography in suspected coronary artery disease: the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps)J Am Coll Cardiol Nørgaard BL Leipsic J Gaur S 114511556320142448626610.1016/j.jacc.2013.11.043 · doi ↗ · pubmed ↗
- 7Rationale, design and goals of the Heart Flow assessing diagnostic value of non-invasive FFR(CT) in Coronary Care (ADVANCE) registry J Cardiovasc Comput Tomogr Chinnaiyan KM Akasaka T Amano T 6267112017 https://doi.org/10.1016/j.jcct.2016.12.002.2801729110.1016/j.jcct.2016.12.002 · doi ↗ · pubmed ↗
- 8Caution is needed when evaluating coronary slit-like lesions with FFR-CT Cardiovasc Interv Ther Kosaki T Okayama H Okabe H Shigematsu T Higaki A Yamada T 7477483720223536620210.1007/s 12928-022-00855-1 · doi ↗ · pubmed ↗