An unusual cause of anterior wall ST-elevation myocardial infarction: a case report
Zouhir Dindane, Elena Golgor, Axel Linke, Norman Mangner

TL;DR
A case of heart attack caused by metastatic lung cancer highlights the need for accurate diagnosis and palliative care in rare, complex situations.
Contribution
Presents a rare case of tumour-induced myocardial infarction mimicking AMI, emphasizing diagnostic and therapeutic challenges.
Findings
Metastatic lung cancer can mimic acute myocardial infarction with ST-elevation and elevated cardiac enzymes.
Imaging confirmed tumour infiltration of the coronary artery, leading to unsuccessful intervention attempts.
The case highlights the importance of palliative care in managing such rare and complex conditions.
Abstract
Metastatic tumours, notably lung cancer, can cause conditions resembling acute myocardial infarctions (AMIs), contributing to the minor percentage of AMIs unrelated to coronary atherosclerosis. These instances necessitate specialized diagnostic and therapeutic approaches due to the distinct underlying pathology. We report a case of a 65-year-old male with metastatic lung cancer presenting with prolonged angina pectoris. Elevated troponin and creatine kinase levels led to emergency catheterization, revealing a total occlusion of the distal left coronary artery attributed to tumour infiltration. Intervention attempts were unsuccessful, and given the palliative context, other revascularization strategies were not pursued. Two-dimensional transthoracic echocardiogram depicted tumour invasion at the heart’s apex, confirming the diagnosis. The patient passed away shortly after receiving…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
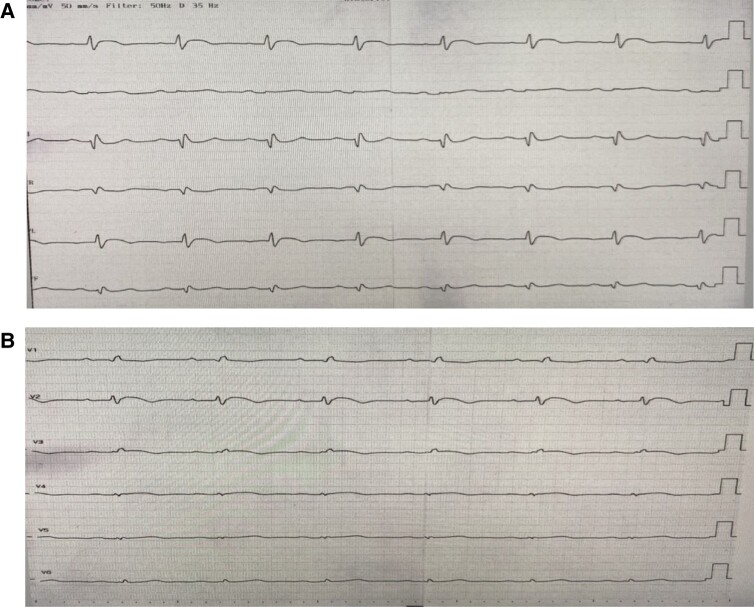 Figure 1
Figure 1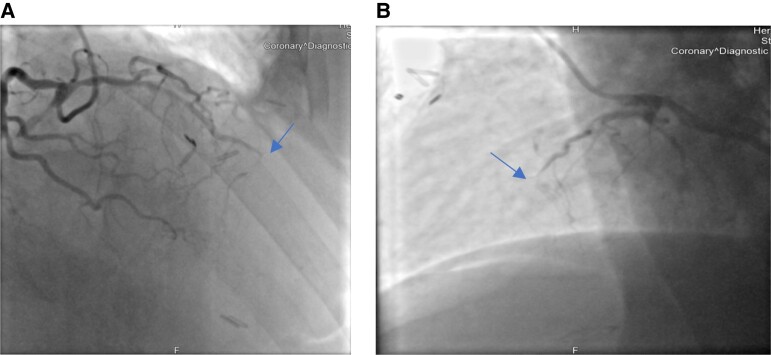 Figure 2
Figure 2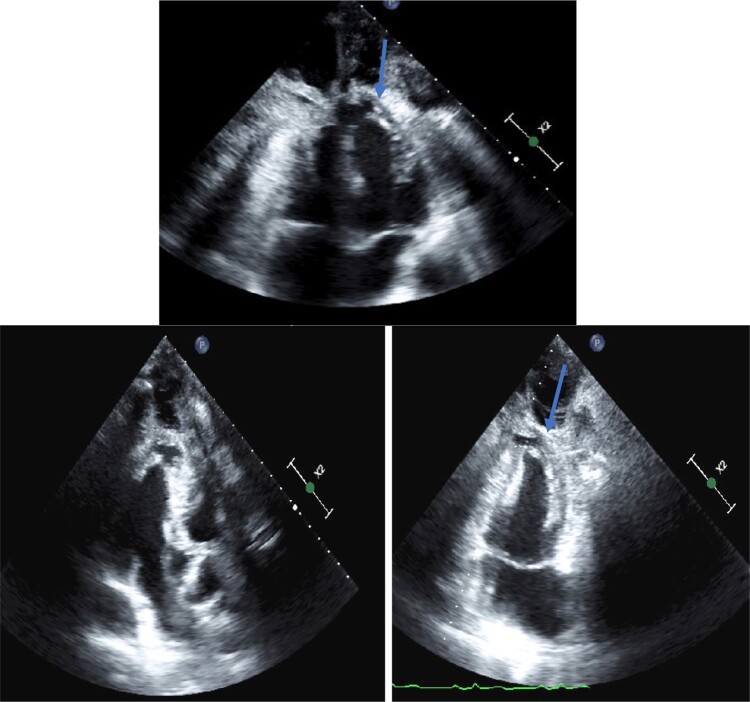 Figure 3
Figure 3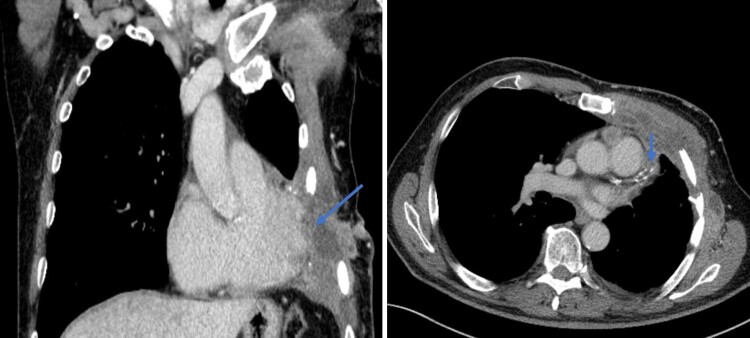 Figure 4
Figure 4| Time | Event |
|---|---|
| 2 years ago | Diagnosis of lung cancer (cT4cN1cM1) |
| Over the next 2 years | Treatment involving surgery, adjuvant chemotherapy, and three rounds of radiation therapy for the bone metastasis in the left scapula |
| Current presentation | Transferred to the emergency department with angina pectoris |
| On admission | Elevated high-sensitivity troponin and CK levels on blood test |
| On admission | Diagnosis of ST-elevation AMI, transfer for emergency catheterization |
| During catheterization | Coronary angiogram shows total occlusion of the distal LAD Unsuccessful wiring attempts of the occluded vessel |
| During hospital stay | TTE study shows invasion of the heart apex by the metastatic tumour, with localized thickening of the apical left ventricular wall and localized wall motion asynergy |
| During hospital stay | Review of previous CT images confirms tumour infiltration into the left ventricular apex |
| During hospital stay | Decision against further revascularization strategies due to the palliative situation |
| Few days after hospital stay | The patient underwent radiotherapy once more but unfortunately passed away |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · Cardiac tumors and thrombi · Pericarditis and Cardiac Tamponade
Introduction
Primary cardiac tumours are extremely rare. In contrast, metastatic heart involvement is nearly 20 times more frequent and has been observed in autopsy series in up to one in five cancer patients.^1^ The clinical presentation varies from asymptomatic to acute presentations with chest pain, arrhythmias, and acute myocardial infarction (AMI). We report here the case of a patient who developed AMI due to total occlusion of the left anterior descending (LAD) artery due to metastatic lung cancer.
Summary figure
**: **
Case report
A 65-year-old man with known metastatic lung cancer was transferred to our emergency department due to typical angina pectoris lasting ∼8 h.
The patient first received a diagnosis of lung cancer two years ago, which was classified based on the TNM system (tumour, nodes, metastases) as cT4cN1cM1. The palliative treatment involved a combination of surgery, adjuvant chemotherapy, and three rounds of radiation therapy to address the bone metastasis in the left scapula.
Until his current presentation, the patient had no history of chest pain, either at rest or during exertion, and no history of coronary artery disease. His coronary risk factors included hypertension and former smoking. On admission, the patient was haemodynamically stable without any signs of cardiac decompensation (Killip I). ECG showed ST-segment elevation in the anterolateral leads V2, V3, I, and aVL (Figure 1). A blood test conducted externally revealed elevated levels of high-sensitivity troponin and creatine kinase (CK), measured at 154 ng/L and 300 U/L, respectively. ST-elevation AMI was diagnosed, and the patient was transferred for emergency catheterization.
Illustrates ST-segment elevation detected in the anterolateral leads of the ECG as well as a QRS low voltage. (A) The limb leads; (B) the precordial Leads.
The coronary angiogram revealed a total occlusion of the distal LCA (Figure 2). It was conspicuous that no cardiac motion was detectable at the left ventricular apex and the mid-LCA (see Supplementary material online, Video S1). Several wiring attempts of the occluded vessel were unsuccessful and were not forced due the risk of perforation and bleeding under the suspicion of tumour invasion into the myocardium. Due to the palliative situation, other revascularization strategies weren’t considered.
(A) Shows a RAO cranial view of the LCA; (B) shows a LAO cranial view of LCA, both views showing a distal total occlusion of the left coronary artery.
The performed transthoracic echocardiography (TTE) study showed an invasion of the apex of the heart by the metastatic tumour, which was manifested by localized thickening of the apical left ventricular wall along the site of tumour attachment, a localized wall motion asynergy was also observed (Figure 3, Supplementary material online, Video S2). A review of previous CT images showed evidence of tumour infiltration and contrast enhancement into the left ventricular apex (Figure 4). The localized thickening and wall motion asynergy observed on TTE corresponded well with the identified area of tumour involvement.
Displays a set of three views of the transthoracic echocardiogram, including a four-chamber view, a two-chamber view, and a three-chamber view. The images reveal a localized thickening of the apical left ventricular wall (arrow), which corresponds to the site of tumour attachment. The thickening is visualized as a focal area of hyperechogenity, with a blurred margin and a heterogenous texture.
Displays a soft tissue window of a CT scan of the thorax, showing both a coronal and axial section. The images reveal a large malignant tumour infiltrating the myocardium of the left ventricle with contrast enhancement.
In the synopsis of the collected findings, our diagnosis hypothesis of occlusion due to tumour metastasis in the left ribs could be confirmed. The patient underwent radiotherapy once more, but unfortunately passed away a few days later.
Discussion
About 5% of AMIs are not caused by coronary atherosclerosis and plaque rupture,^2^ and many factors are implicated, including cocaine misuse, radiation-associated fibrosis, amyloidosis, infectious illness, embolism, and neoplasia. Metastatic tumours are frequently asymptomatic, although heart failure, pericardial effusion, arrhythmia, myocardial infarction, and sudden cardiac death can happen and this relies on the location and size of the tumour.
We herein describe a case of metastatic lung cancer infiltrating the left ventricle and leading to the occlusion of the LAD artery. Given the patient’s overall condition and a life expectancy exceeding 6 months, an emergency angiogram was performed,^3^ revealing a complete occlusion of the distal LAD. Multiple attempts to wire the occluded vessel were unsuccessful. Due to the palliative situation, other revascularization strategies weren’t considered. The performed TTE study was able to delineate the location of the tumoural invasion at the apex of the heart. We decided against further imaging studies regarding the patient’s situation and the diagnosis associated with a dismal prognosis.
Myocardial involvement due to metastasis may provoke ST-elevation myocardial infarction.^4^ Such metastases might obstruct coronary arteries, either by direct invasion or compression, which could make percutaneous coronary intervention (PCI) a consideration. The appropriateness of PCI must be carefully weighed against potential bleeding risks, cancer prognosis, and the patient’s overall clinical condition^5^—including pain intensity, response to analgesia, haemodynamic stability, as well as patient and family preferences.
In assessing the tumour’s extent, imaging modalities such as two-dimensional TTE are instrumental in delineating the size and proximity of the metastasis to the coronary vessels, thus guiding the treatment strategy.
Conclusion
We report a rare clinical scenario of a patient who had a myocardial infarction caused by the occlusion of the coronary artery by a myocardial infiltration through metastatic lung cancer. Two-dimensional echocardiography was useful for obtaining good spatial information and diagnosing the cause of AMI in this patient. A percutaneous intervention may not succeed in such cases, and palliative strategies have to be considered.
Supplementary Material
ytae243_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lam KY , Dickens P, Chan AC. Tumors of the heart. A 20-year experience with a review of 12,485 consecutive autopsies. Arch Pathol Lab Med 1993;117:1027–31.8215825 · pubmed ↗
- 2Niccoli G , Scalone G, Crea F. Acute myocardial infarction with no obstructive coronary atherosclerosis: mechanisms and management. Eur Heart J 2015;36:475–81.25526726 10.1093/eurheartj/ehu 469 · doi ↗ · pubmed ↗
- 3ESC Guidelines on cardio-oncology.
- 4Chen J , Craft C, Panakos AW, Marhefka GD. Squamous cell carcinoma metastatic to the heart mimicking ST-elevation myocardial infarction. Med Forum 2016;17, Article 3.
- 5Kwok CS , Wong CW, Kontopantelis E, Barac A, Brown SA, Velagapudi P, et al Percutaneous coronary intervention in patients with cancer and readmissions within 90 days for acute myocardial infarction and bleeding in the USA. Eur Heart J 2021;42:1019–1034.33681960 10.1093/eurheartj/ehaa 1032 · doi ↗ · pubmed ↗