Progression-free survival estimation of docetaxel-based second-line treatment for advanced non-small cell lung cancer: a pooled analysis from 18 randomized control trials
Chaithra N, Anisha Jain, Sahana C, Bhargav Shreevatsa, Saravanan Rajendrasozhan, Chandan Dharmashekar, Kuralayanapalya Puttahonnappa Suresh, Sharanagouda S. Patil, Pranav Singh, Prashant Vishwanath, Chandrashekar Srinivasa, Shiva Prasad Kollur, Chandan Shivamallu

TL;DR
This study analyzed 18 clinical trials to compare how well docetaxel works compared to other treatments for advanced non-small cell lung cancer, focusing on how long patients stayed without disease progression.
Contribution
The study provides a pooled analysis of docetaxel's progression-free survival in second-line treatment for advanced NSCLC compared to other therapies.
Findings
Docetaxel-based therapy showed significantly longer progression-free survival (PFS) than antineoplastic agents, kinase inhibitors, and monoclonal antibodies.
Overall meta-analysis found slightly longer PFS in the standard treatment arm compared to the experimental therapy arm.
Docetaxel outperformed other therapies in second-line treatment of advanced NSCLC based on PFS.
Abstract
Lung cancer is the foremost cause of cancer-related death globally, with non-small cell lung cancer (NSCLC) accounting for 85–90% of cases. Targeted therapy is the most essential therapeutic option for NSCLC, other common treatments include radiation therapy, surgery, chemotherapy, and immunotherapy. Our study objective was to estimate whether progression-free survival (PFS) is an outcome of NSCLC extracted from 18 randomized control trials (RCTs) with docetaxel as experimental group and antineoplastic agent, kinase inhibitor, and monoclonal antibodies as a control group. We selected relevant studies published between 2011 and 2022 using Google Scholar, PubMed, Scopus, Science Direct, and Cochrane Library. Advanced NSCLC, chemotherapy, RCT, docetaxel, and second-line treatment were the terms included in the search. A total of 9738 patients were evaluated from the 18 identified…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
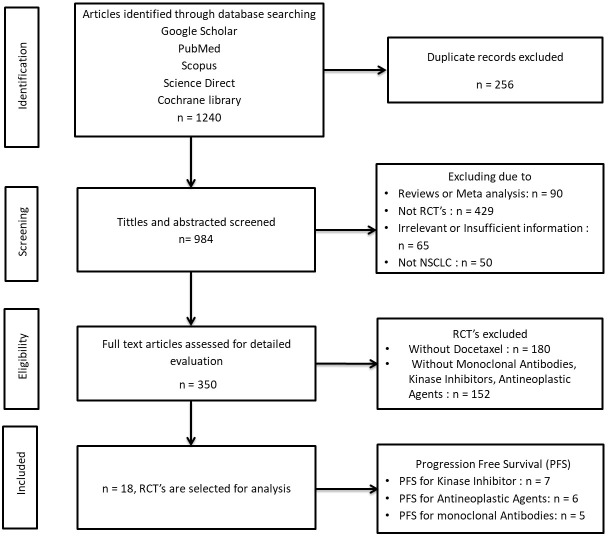 Figure 1
Figure 1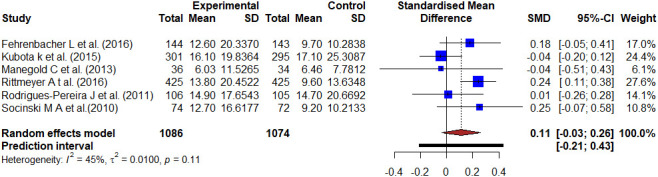 Figure 2
Figure 2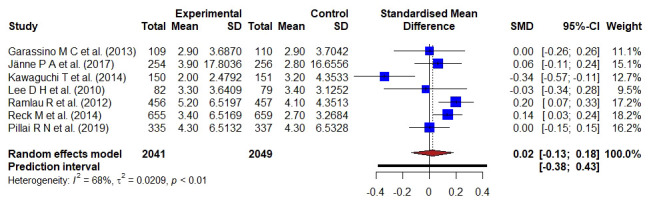 Figure 3
Figure 3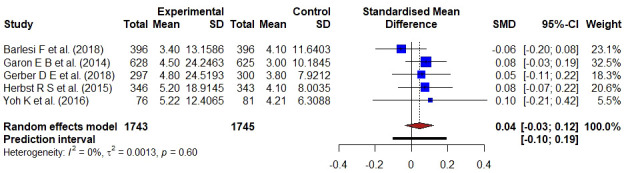 Figure 4
Figure 4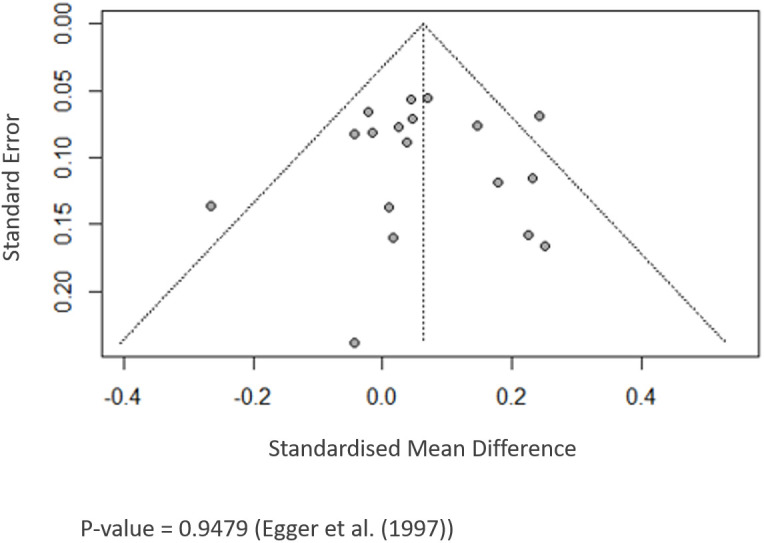 Figure 5
Figure 5| Sl. | Study reference | Phase of trail | Patients, n | Median age | Drug class intervention | Intervention and dosage | Treatment and dosage | Primary endpoint |
|---|---|---|---|---|---|---|---|---|
| 1 | Barlesi F et al. (2018) ( | 3 | 792 | 63.5 | 3 | Avelumab 10mg/kg/2W | Docetaxel 75mg/m2/3W | PFS |
| 2 | Fehrenbacher L et al. (2016) ( | 2 | 287 | 62 | 1 | Atezolizumab 1200mg/3W | Docetaxel 75mg/m2/3W | PFS |
| 3 | Garassino M C et al. (2013) ( | 2 | 219 | 66.5 | 2 | Erlotinib 150mg/D | Docetaxel 75mg/m2/3W | PFS |
| 4 | Garon E B et al. (2014) ( | 3 | 1253 | 61.5 | 3 | Ramucirumab 10mg/kg/3W + Docetaxel 75mg/m2/3W | Placebo + Docetaxel 75mg/m2/3W | PFS |
| 5 | Gerber D E et al. (2018) ( | 3 | 597 | 62.5 | 3 | Bavituximab 3mg/kg/W + Docetaxel 75mg/m2/3W | Placebo + Docetaxel 75mg/m2/3W | PFS |
| 6 | Herbst R S et al. (2015) ( | 2&3 | 689 | 63 | 3 | Pembrolizumab 10mg/kg/3W | Docetaxel 75mg/m2/3W | PFS |
| 7 | Jänne P A et al. (2017) ( | 2&3 | 510 | 61.4 | 2 | Selumetinib 75mg/0.5D + Docetaxel 75mg/m2/3W | Placebo + Docetaxel 75mg/m2/3W | PFS |
| 8 | Kawaguchi T et al. (2014) ( | 3 | 301 | 68 | 2 | Erlotinib 150 mg/D | Docetaxel 75mg/m2/3W | PFS |
| 9 | Kubota k et al. (2015) ( | 3 | 596 | 62 | 1 | S-1 80mg/m2/D + cisplatin 60mg/m2/W | Docetaxel 60mg/m2/3W + Cisplatin 80mg/m2/3W | PFS |
| 10 | Lee D H et al. (2010) ( | 3 | 161 | 57.5 | 2 | Gefitinib 250mg/D | Docetaxel 75mg/m2/3W | PFS |
| 11 | Manegold C et al. (2013) ( | 2 | 70 | 60.2 | 1 | Cilengitide 600mg/m2/0.5D | Docetaxel 75mg/m2/3W | PFS |
| 12 | Ramlau R et al. (2012) ( | 3 | 913 | 59.6 | 2 | (Ziv-) aflibercept 6mg/kg/3W + Docetaxel 75mg/m2/3W | Placebo + Docetaxel 75mg/m2/3w | PFS |
| 13 | Reck M et al. (2014) ( | 3 | 1314 | 60 | 2 | Docetaxel 75mg/m2/3W + Nintedanib 200mg/0.5D | Docetaxel 75mg/m2/3W | PFS |
| 14 | Rittmeyer A t al. (2016) ( | 3 | 850 | 64 | 1 | Atezolizumab 1200mg/3W | Docetaxel 75mg/m2/3W | PFS |
| 15 | Rodrigues-Pereira J et al. (2011) ( | 3 | 211 | 59.5 | 1 | Pemetrexed 500mg/m2/3W + Carboplatin 5mg/ml/min | Docetaxel 75mg/m2/3W + Carboplatin 5mg/ml/min | PFS |
| 16 | Socinski M A et al. (2010) ( | 2 | 146 | 66 | 1 | Pemetrexed 500mg/m2/3W + Carboplatin 6mg/ml/min | Docetaxel 75mg/m2/3W + Carboplatin 6mg/ml/min | PFS |
| 17 | Yoh K et al. (2016) ( | 2 | 157 | 65 | 3 | Ramucirumab 10mg/kg/3W + Docetaxel 60mg/m2/3W | Placebo + Docetaxel 75mg/m2/3W | PFS |
| 18 | Pillai R N et al. (2019) ( | 3 | 672 | 68 | 2 | Ganetespib 150mg/m2/2W + Docetaxel 75mg/m2/3W | Docetaxel 75mg/m2/3W | PFS |
- —University of Hail 10.13039/501100008809
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Treatments and Mutations · Lung Cancer Diagnosis and Treatment · Lung Cancer Research Studies
Introduction
1
Cancer results from a complex multistep system including the accumulation of several gene mutations, which comprises encoding microRNA (1). Heredity ionizing radiation, chemical substances, alcohol, nitrates, estrogens, viruses, stress, and age are the main risk factors (2). Carcinoma, sarcoma, leukemia, lymphoma, and myeloma are types of cancer (3). According to the World Health Organization (WHO), it is the first or second largest cause of mortality before the age of 70 in 112 (of 183) nations, ranks third or fourth in another 23 countries, and was a major impediment to improving life expectancy in every country on the planet in 2019 (4).It has an impact on the high incidence of stroke and coronary heart disease mortality in many nations (5). HPV, HBV, HIV, and bacteria like Helicobacter pylori (stomach cancers) are infectious agents increasing the risk of cancer (6). The number of cancer cases is expected to increase from 979 786 in 2010 to 1 148 757 cases in 2020 (7). Lung cancer is the most recurrently diagnosed and the leading cause of cancer mortality. The two most common types of lung cancer are NSCLC and small cell lung cancer (SCLC). NSCLC makes for 80 to 85% of lung cancer cases, with SCLC accounting for the rest. Patients with lung cancer may be eligible for various therapies, including surgery, radiation, chemotherapy, and targeted therapy, depending on their stage. Targeted therapy is the most essential therapeutic option for NSCLC, other common treatments include radiation therapy, surgery, chemotherapy, and immunotherapy. Targeted therapies include monoclonal antibodies and small-molecule inhibitors. Specific mutations have been detected thanks to advances in genetics and biomarker testing, allowing doctors to better target treatment for individual patients (8, 9). Cigarette smoking is considered a significant hazard factor with an 82% mortality rate in males compared to females (10). It is asymptomatic in its early-stage, and patients diagnosed at an advanced stage experience a poor prognosis (11). The objective of our study was to estimate whether the PFS is an outcome of NSCLC, using data from 18 RCTs (12). PFS, the time from therapeutic initiation to disease progression, may be used as a measure of clinical benefit for drug approvals, depending on the condition and response observed (13).
Methods
2
We selected relevant studies published between 2011 and 2022 using Google Scholar, PubMed, Scopus, Science Direct, and Cochrane Library. Advanced NSCLC, chemotherapy, RCT, docetaxel, and second-line treatment were the terms included in the search.
Randomized trials including patients diagnosed with NSCLC that evaluated docetaxel with a kinase inhibitor, antineoplastic agents, and monoclonal antibodies for NSCLC were included. Docetaxel compared with other therapeutic agents except for kinase inhibitors, monoclonal antibodies and antineoplastic agents was considered exclusion criterion. Similarly, studies that compared docetaxel to other drugs were excluded, as well as early studies published as a series of articles by the same author with overlapping data, editorials, case reports, conference articles, experimental studies, and related studies that failed to provide significant findings. Authorship, publication bias, clinical trials, demographic attributes, histology characteristics, smoking status, treatment for each group, and adverse events were all extracted using a fixed standardized procedure. The conventional treatment in this trial was docetaxel, while the experimental arm was a kinase inhibitor, antineoplastic drug, or monoclonal antibody.
A comprehensive search approach was devised to reduce the risk of publishing bias. Graphical funnel plots were used to visually evaluate publication bias and the quality of RCTs.
Pooled HR was calculated with 95% CI. We used forest plots and inconsistency statistic [I2] to determine heterogeneity. The OR was the summary measure used for pooling the studies. Hedge’s method evaluates the effect size calculated by standard mean difference (SMD) given as Hedge’s g-value. The meta-analysis was summarized graphically using a forest plot. Meta package of R Studio (v2021.09.0) was used to perform the meta-analysis.
Results
3
The details of study selection criteria followed for the meta-analysis of drug intervention prevalence are given in Figure 1. The number of published articles was 1240, of which 256 were rejected for duplication in one or the other form, 68 were excluded since reviews or meta-analysis and 429 were excluded as non-randomized control trials, 65 were excluded due to Irrelevant or Insufficient information and 50 excluded because of not NSCLC. Then after filtering 350 randomized control trials were selected for detailed evaluation, in which 180 were excluded which were treatment arms without docetaxel, and 152 were excluded which were without monoclonal antibodies, kinase inhibitors, and antineoplastic agents. Hence, finally 18 Randomized control trials were selected for the study.
Flowchart of the study selection steps.
The characteristics of selected RCTs of meta-analysis are given in Table 1. Six RCTs phase 3 data for the antineoplastic agent classes of intervention were analyzed, with 850 the maximum number of patients recorded with a median age of 64 and PFS as the primary endpoint. Data from seven phase 2 and 3 RCTs were analyzed for the kinase inhibitor class of intervention, with 1314 the highest number of patients having a primary endpoint of PFS with a median age of 60. The remaining five RCTs were phase 2 and 3 monoclonal antibody class intervention data analyzed with PFS as the main endpoint. The highest number of patients recorded was 1253 with a median age of 61.5 years.
Figures 2-4 show forest plots comparing the PFS of docetaxel to antineoplastic agents, kinase inhibitors, and monoclonal antibodies-based treatment. The six studies reported the PFS of antineoplastic agents compared with docetaxel with 2160 patients involved. The meta-analysis of all involved studies revealed significant statistical heterogeneity (I2 = 96%, τ2 = 0.2502, p < 0.01), and Hedge’s corrected SMD was -0.36 (95% CI: -1.01–0.29). There was a moderate effect because it was a negative value smaller than -0.20, which implies the result favored the antineoplastic agents-based treatment.
Forest plot representing the PFS of docetaxel versus antineoplastic agents treatment. Hedge’s corrected SMD is -0.36, and Higgin’s and Thompson’s I2 statistic is 96%.
Forest plot representing the PFS of docetaxel- versus kinase inhibitors- treatment; the Hedge’s corrected SMD is 0.02, and Higgin’s and Thompson’s I2 statistic is 68%.
Forest plot representing the PFS of docetaxel versus monoclonal antibodies treatment. Hedge’s corrected SMD is 0.04, and Higgin’s and Thompson’s I2 statistic is 0%.
A total of 4090 patient data from seven studies reported the PFS of kinase inhibitor compared with docetaxel-based treatment. A bias-corrected SMD; Hedge’s g-value was 0.02 (95% CI: -0.13–0.18), implying the result favored the docetaxel-based standard treatment. A significant statistical heterogeneity (I2 = 68%, τ2 = 0.0209, p < 0.01) was found in the pooled analysis of all included studies.
The PFS of monoclonal antibodies was compared to docetaxel in five studies involving 3488 individuals. There was no substantial statistical heterogeneity in a pooled analysis of all included trials (I2 = 0, τ2 = 0.0013, p = 0.60), and Hedge’s g-value was 0.04 (95% CI: -0.03–0.12), indicating that the result favored docetaxel-based treatment. The SMD value was less than 0.20, indicating that docetaxel had a minor effect.
The p-values for the meta-analyses of PFS of 18 RCTs are > 0.05, indicating that formal statistical testing revealed no indication of significant publication bias (PFS: Egger’s test, p = 0.947) (Figure 5).
Funnel plot showing publication bias.
Discussion
4
A meta-analysis was conducted for 18 RCTs (14–31) with docetaxel as the experimental group and antineoplastic agent, and kinase inhibitor and monoclonal antibodies as a control group including 9738 patients with stage III–IV NSCLC. The objective of this study was to see if the PFS of patients improved. Platinum-based two-drug combinatorial chemotherapy has been the standard of care for advanced NSCLC patients (22–24). Our study’s main aim was to compare the two treatment regimens in terms of PFS in patients with advanced NSCLC (24). A total of 2160 cases with six RCTs were used to compare the docetaxel with antineoplastic agents. Six studies compared the improvement of PFS between docetaxel and atezolizumab, S-1 plus cisplatin, cilengitide, pemetrexed/carboplatin (15, 22, 24, 27–29). The period from randomization to either progressing illness or death was referred to as PFS. The different randomization methods are used to receive either 60 mg/m2 docetaxel plus cisplatin, 75 mg/m2 docetaxel, docetaxel 75 mg/m2/3W + carboplatin 5 mg/ml/min or oral S-1 80 mg/m2/day plus cisplatin 60 mg/m2, cilengitide 600 mg/m2, pemetrexed 500mg/m2/3W + carboplatin 5mg/ml/min, atezolizumab 1200 mg to see the improvement of PFS between these groups (15, 22, 24, 27–29). The PFS was similar between each control and treatment group. The median PFS was 2.7 months with atezolizumab and 3.0 months with docetaxel with a HR of 0.94 (95% CI 0.72–1.23) (15). The median PFS was 2.8 months with atezolizumab and 4.0 months with docetaxel. The HR was 0.63 [95% CI 0.43–0.91] (27). The median PFS was 4.9 months in the SP group and 5.2 months in the DP group with a HR of 1.113; 95% CI, 0.945 to 1.311 (22). There were no statistically significant differences in PFS between the treatment groups with a HR of 0.91 (0.67–1.23) (24). Therefore, there was no improvement in PFS between the groups.
In patients with metastatic NSCLC, antibodies targeting the immune checkpoint molecules PD-L1 or PD-1 enhance PFS compared to standard of care chemotherapy treatment (14). A total of 3488 patients in five trials have been used to compare docetaxel-based treatment with monoclonal antibody-based therapy (14, 17–19, 30). The meta-analysis of avelumab versus docetaxel in advanced NSCLC patients and progression of disease following platinum-based treatment was described by Barlesi et al. (14). A block randomized method was used to acquire either docetaxel 75 mg/m2 or avelumab 10 mg/kg and PFS was a secondary endpoint. The median PFS in the avelumab group was 2.8 months (95% CI 2.7–3.5) and 4.2 months (3.3–5.2) in the docetaxel group with HR 1.16 [95% CI 0.97–1.40]. As a result, with avelumab, PFS was substantially longer, and objective responses were more likely than with docetaxel. Garon et al., compared the effectiveness and safety of docetaxel with ramucirumab versus placebo as second-line therapy for stage IV NSCLC patients (17). A randomized method was used to assign the patients either ramucirumab 10 mg/kg or docetaxel 75 mg/m2. The median PFS for the ramucirumab group was 45 months, compared to 30 months for the control group with a HR of 0.76 (0.68–0.86). The PFS is improved in ramucirumab compared to docetaxel in patients with stage IV NSCLC. The efficacy of bavituximab in combination with docetaxel in patients with advanced NSCLC who have already been treated was investigated by Gerber et al. (18). The authors used a stratified randomized technique to provide docetaxel plus placebo or docetaxel plus bavituximab 3 mg/kg to the patients. With HR 1.00; 95% CI, 0.82–1.22, there was no alteration in PFS. The addition of bavituximab to docetaxel did not improve PFS. Herbst et al. compare pembrolizumab’s effectiveness and safety to those of docetaxel (19). A randomized method was used to acquire either pembrolizumab 10 mg/kg or docetaxel 60 mg/m to the selected participants. The median PFS was 3.9 months with pembrolizumab, 4.0 months with docetaxel (HR 0.88, 95% CI 0.74–1.05). Therefore, PFS was significantly longer with pembrolizumab than docetaxel. Yoh et al., explain how a phase II, double-blind, randomized, placebo-controlled trial in Japanese patients with NSCLC examined the safety and effectiveness of second-line ramucirumab-docetaxel (30). The median PFS was 5.22 months for ramucirumab-docetaxel and 4.21 months for placebo-docetaxel with HR of 0.83 (95% CI 0.59–1.16). Hence, PFS was longer with ramucirumab-docetaxel than with placebo-docetaxel. Seven clinical studies, including 4090 participants, were conducted to compare the docetaxel-based therapy with kinase inhibitor for patients with advanced NSCLC. The authors of seven studies compared the efficacy and safety of Gefitinib, erlotinib, aflibercept (Ziv-aflibercept), docetaxel plus nintedanib, mitogen-activated protein kinase (MEK) inhibitor, selumetinib + docetaxel and combination of ganetespib-docetaxel with the treatment group of docetaxel in patients with advance NSCLC to check the improvement of PFS between the groups. A randomized clinical method was used and patients received either docetaxel (75 mg/m2), IV placebo plus docetaxel (75 mg/m2), placebo + docetaxel (75 mg/m2/3W) or gefitinib (250 mg/d), erlotinib orally 150mg/day, (Ziv-) aflibercept 6 mg/kg intravenous plus docetaxel 75 mg/m2 erlotinib 150 mg/D, nintedanib 200 mg orally, selumetinib 75mg/0.5D plus docetaxel 75mg/m2/3W, ganetespib 150 mg/m until unacceptable side effects or disease progression based on previous bevacizumab treatment, histology, ECOG performance status, and presence of brain metastases (15, 19, 20, 22, 24, 25, 30). PFS was estimated as a primary and secondary endpoint in these studies. The median PFS was 3.9 months with selumetinib + docetaxel and 2.8 months with placebo + docetaxel with HR, 0.93 [95% CI, 0.77–1.12] (19). The median PFS in the ganetespib and docetaxel arm was 4.2 months, and 4.3 months in the docetaxel arm, with an HR of 1.16 (95% CI, 0.96–1.403) (31). Gefitinib had a better PFS than docetaxel, with a HR of 0.729; 90% CI, 0.533–0.998. The PFS was longer with gefitinib than docetaxel. As a result, gefitinib was a crucial and effective second-line treatment option for Korean NSCLC patients (23). Gefitinib had a longer PFS than docetaxel. The median PFS was 2.9 months with docetaxel versus 2.4 months with erlotinib with HR 0.71, 95% CI 0.53–0.95 (16). Median PFS was significantly longer in the (Ziv-)aflibercept arm of 5.2 months than in the placebo arm of 4.1 months with HR was 0.82 (95% CI 0.72–0.94). Erlotinib had a median PFS of 2.0 months against 3.2 months when compared to docetaxel with an HR of 1.22; 95% CI, 0.97 to 1.55. In an EGFR-unselected patient sample, erlotinib failed to improve PFS compared to docetaxel (21). The median PFS in the docetaxel plus nintedanib group was 3·4 months compared to 2.7 months in the docetaxel plus placebo group (HR 0.79, 95% CI 0.68–0.92) (26).
There are limits to our analysis that should be considered while evaluating the results. First, the different treatment regimens add to the meta-analysis’ clinical heterogeneity, which makes meta-analysis interpretation more difficult. In three studies, docetaxel was used in conjunction with other medicines, either cisplatin or carboplatin, in the control arm. The quality of the results was influenced by the quality of each study’s results. Finally, because the research included in this study was all conducted in the West, the findings must be confirmed in Asia. Docetaxel was revealed to be more effective in the second-line therapy of advanced NSCLC than antineoplastic drugs, kinase inhibitors, and monoclonal antibodies, according to the findings.
Conclusion
5
The phase 2 and 3 study of antineoplastic agents demonstrate a clinically significant survival benefit over docetaxel in patients with NSCLC. Compared to docetaxel, monoclonal antibodies and kinase inhibitors did not affect PFS in NSCLC patients. From the results of 18 trials involving 9738 patients, those who received docetaxel-based therapy had a significantly longer PFS than those who received kinase inhibitors or monoclonal antibodies. In the overall meta-analysis, patients in the standard treatment arm had a slightly longer PFS than those in the experimental therapy arm. Biological behavior subgroups such as those entirely refractory, those with partial and incomplete responses, and those with short and extended disease-free intervals will be examined in future meta-analysis investigations.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Author contributions
CN: Methodology, Software, Writing – original draft, Writing – review & editing. AJ: Validation, Writing – original draft, Writing – review & editing. SC: Methodology, Validation, Writing – original draft. BS: Resources, Writing – review & editing. SR: Funding acquisition, Writing – review & editing. CD: Data curation, Writing – review & editing. KS: Validation, Writing – review & editing. SP: Resources, Supervision, Writing – review & editing. PS: Supervision, Writing – review & editing. PV: Supervision, Validation, Writing – review & editing. CSr: Data curation, Writing – review & editing. SK: Supervision, Validation, Writing – original draft. CSh: Conceptualization, Investigation, Supervision, Validation, Writing – review & editing.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ali Syeda Z Langden SS Munkhzul C Lee M Song SJ . Regulatory mechanism of micro RNA expression in cancer. Int J Mol Sci. (2020) 21:1723. doi: 10.3390/ijms 21051723 32138313 PMC 7084905 · doi ↗ · pubmed ↗
- 2Cicero G De Luca R Dieli F . Progression-free survival as a surrogate endpoint of overall survival in patients with metastatic colorectal cancer. Onco Targets Ther. (2018) 11:3059–63. doi: 10.2147/OTT.S 151276 PMC 597560529872317 · doi ↗ · pubmed ↗
- 3Glinsky GV Berezovska O Glinskii AB . Microarray analysis identifies a death-from-cancer signature predicting therapy failure in patients with multiple types of cancer. J Clin Invest. (2005) 115:1503–21. doi: 10.1172/JCI 23412 PMC 113698915931389 · doi ↗ · pubmed ↗
- 4Sundar S Wu J Hillaby K Yap J Lilford R . A systematic review evaluating the relationship between progression free survival and post progression survival in advanced ovarian cancer. Gynecol Oncol. (2012) 125:493–9. doi: 10.1016/j.ygyno.2011.12.420 22155676 · doi ↗ · pubmed ↗
- 5Sung H Ferlay J Siegel RL Laversanne M Soerjomataram I Jemal A . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71:209–49. doi: 10.3322/caac.21660 33538338 · doi ↗ · pubmed ↗
- 6Masrour-Roudsari J Ebrahimpour S . Causal role of infectious agents in cancer: An overview. Caspian J Intern Med. (2017) 8:153–8. doi: 10.22088/cjim.8.3.153 PMC 559618428932365 · doi ↗ · pubmed ↗
- 7Takiar R Nadayil D Nandakumar A . Projections of number of cancer cases in India (2010-2020) by cancer groups. Asian Pac J Cancer Prev. (2010) 11:1045–9.21133622 · pubmed ↗
- 8Jain AS Prasad A Pradeep S Dharmashekar C Achar RR Silina E . Everything old is new again: drug repurposing approach for non-small cell lung cancer targeting MAPK signaling pathway. Front Oncol. (2021) 11:741326. doi: 10.3389/fonc.2021.822865 34692523 PMC 8526962 · doi ↗ · pubmed ↗