Wearing surgical face mask has no significant impact on auscultation assessment
Ivana Folnožić, Marija Gomerčić Palčić, Matilda Sabljak, Ena Vučak, Luka Vrbanić, Marija Mandić Perić, Fanika Mrsić, Aljoša Šikić, Ivan Ivanovski

TL;DR
Wearing surgical masks does not significantly affect pulmonologists' ability to assess lung sounds during auscultation.
Contribution
The study empirically shows that mask-wearing does not hinder lung sound assessment by pulmonologists.
Findings
No significant difference in agreement on lung sound assessment with or without masks.
Significant differences in agreement were observed among pulmonologists regardless of mask use.
Mask-wearing does not compromise clinical safety or diagnostic accuracy in auscultation.
Abstract
During the COVID-19 pandemic, universal mask-wearing became one of the main public health interventions. Because of this, most physical examinations, including lung auscultation, were done while patients were wearing surgical face masks. The aim of this study was to investigate whether mask wearing has an impact on pulmonologist assessment during auscultation of the lungs. This was a repeated measures crossover design study. Three pulmonologists were instructed to auscultate patients with previously verified prolonged expiration, wheezing, or crackles while patients were wearing or not wearing masks (physician and patients were separated by an opaque barrier). As a measure of pulmonologists’ agreement in the assessment of lung sounds, we used Fleiss kappa (K). There was no significant difference in agreement on physician assessment of lung sounds in all three categories (normal lung…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
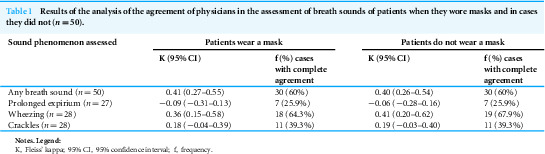 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPhonocardiography and Auscultation Techniques · Noise Effects and Management · Hearing Loss and Rehabilitation
Introduction
Since its outbreak in December 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that causes novel coronavirus disease 2019 (COVID-19) has caused 7,010,568 deaths worldwide (World Health Organization, 2024; https://data.who.int/dashboards/covid19/deaths?n=c, 14th January 2024). Since the beginning of the pandemic, many government health care agencies have recommended community-wide use of face masks as a low-cost and available epidemiologic tool for decreasing viral transmission, especially in patients with chronic diseases (European Centre for Disease Prevention and Control , 2021a; European Centre for Disease Prevention and Control , 2021b). Several studies have demonstrated that wearing face masks leads to a reduction in virus transmission (Seto et al., 2003; Jefferson et al., 2011; Smith et al., 2016; Chu et al., 2020) although more randomized control studies are needed to confirm these findings. Lung sound auscultation is still one of the key parts of a physical examination that is helpful in identifying respiratory pathology even when chest radiography findings appear normal (such as detecting crackles in patients with interstitial lung disease or detecting wheezes in bronchoobstruction). Other advantages of auscultation also lie in its widespread availability and affordability (Fajardo & Davis, 2022). According to the European Respiratory Society (ERS) Task Force on Respiratory Sounds, respiratory sounds should be divided into lung sounds and other (e.g., pleural rub, grunting, and snoring). Lung sounds should then be divided into normal (basic) sounds and adventitious sounds (Pasterkamp et al., 2016).
Since the beginning of the COVID-19 pandemic, most physical examinations have been done while patients were wearing surgical face masks, so the aim of our study was to investigate whether epidemiological recommendations of wearing surgical face masks have an impact on pulmonologist assessment during auscultation, as well as the reliability of performance under this condition.
Materials & Methods
This was a repeated measures crossover design study. We included 50 patients between November and December 2022 who were being treated at the Division of Pulmonology, Department of Internal Medicine, Sestre Milosrdnice University Hospital Center. All patients were older than 18 years and both genders were represented. Only patients with previously verified pathological lung auscultation finding (prolonged expiration, wheezing, or crackles) were included. All patients signed informed consent before being included in the study. The study was approved by the University Hospital Center Sestre Milosrdnice Ethical Committee (approval 251-29-11-21-03). Three pulmonologists were instructed to auscultate patients in the outpatient clinic (part of the forementioned division) and physicians did not sign informed consent. Inclusion criteria were stable chronic lung disease with lung sound phenomena present and the ability to sit upright. Exclusion criteria were acute infections, worsening acute heart disease, body mass indexes less than 18 kg/m2 and more than 40 kg/m2, and the presence of pleural effusion. During examination, physicians were unable to see if the patient was wearing a mask (patients’ heads were behind an opaque barrier). At the beginning of each examination, a fourth physician randomly instructed patients to put on or take off a three-layer surgical ear loop mask (ear loops were put behind both ears, the mask placed in front of nose and mouth, and aluminum strip nose wire pressed over the nose bridge), and the pulmonologist would auscultate the lungs once and then repeat auscultation after the patient changed their mask status. Subsequently, the fourth physician recorded the pulmonologists’ findings.
Statistical analysis
We evaluated the data from both groups (mask and no-mask) and performed statistical analysis. As a measure of the pulmonologists’ agreement in the assessment of lung sounds, we used Fleiss kappa (K).
K assesses the agreement between raters in cases where categorical measures of ordinal or nominal measurement scales were used. Below, we present the results of the analysis of agreement between physicians in the assessment of various respiratory symptoms in two situations—when patients wore a mask and when patients did not wear a mask. Along with the value of K, we also show its 95% confidence interval. If the confidence intervals of the K values in the two situations did not overlap, this means that there was a statistically significant difference in agreement between the two situations. Otherwise, there was no difference.
In addition, for each symptom, the percentage of cases in which all three doctors completely agreed is shown. Software used for statistical analysis was IBM SPSS Statistics 29 (Chicago, IL, USA).
Results
Breath sounds
Three pulmonologists evaluated breath sounds in 50 patients in two situations: while the patients were wearing and not wearing masks. They evaluated breath sounds using the following measurement scale: 0 = normal breath sound, 1 = quieter breath sound, 2 = harsh breath sound. The results of the analysis of physician agreement are presented in Table 1.
Physician agreement in the assessment of breath sounds did not differ depending on whether patients wore a mask or not (Table 1). In both situations, physicians completely agreed in 60% of cases. None of the cases resulted in unanimous agreement among the three physicians on the presence of harsh breath sounds.
Expiration
All three physicians assessed the expiration of 27 patients in two situations (patients with and without a mask). Expiration was assessed using the following scale: 0 = regular, 1 = prolonged. The results of the analysis of physician agreement are shown in Table 1.
Physician agreement on the duration of expiration did not differ depending on whether patients wore mask or not. However, in both situations, the agreement was very low and physicians were in complete agreement only in 26% of cases.
Abnormal breath sounds
All three physicians assessed the presence of abnormal breath sounds in 28 patients in two situations (patients with and without a mask). They evaluated two sound phenomena: wheezing and crackles. Both phenomena were evaluated using a measuring scale: 0 = sound phenomenon is not present, 1 = sound phenomenon is present. The results of the analysis of physician agreement are shown in Table 1.
Table 1: Results of the analysis of the agreement of physicians in the assessment of breath sounds of patients when they wore masks and in cases they did not (n = 50).
Agreement of physicians in the assessment of abnormal breath sounds did not differ based on whether patients wore a mask or not. When assessing the presence of wheezing, agreement was mild to moderate, and physicians agreed in 64% of cases when patients wore a mask and 68% of cases when patients did not wear a mask. When assessing crackles, agreement was low, and physicians agreed in both situations in 39% of cases.
Discussion
To our knowledge, no similar study has been published so far. The results of our study showed that there was no significant difference in pulmonologists’ agreement in the assessment of breath sounds in all three categories (normal breath sound, duration of expiration, and abnormal breath sound) whether the patient was wearing a mask or not, but there were significant differences among pulmonologists when it came to overall agreement in assessed breath sounds. The difference in auscultation was determined by each pulmonologist because auscultation is a subjective method and interpretations vary widely between physicians (Xavier et al., 2014). Auscultation is an essential method in everyday practice that strongly influences future diagnostic and therapeutic workflows. It is performed by various specialists and characterized by its cost effectiveness, availability, simplicity, and transferability. The disadvantages of the mentioned methods are low sensitivity (37%) and acceptable specificity (89%), at least in acute respiratory pathology, all due to high subjectivity and difference in the experience of physicians (Arts et al., 2020). Indeed, physicians often differ in their assessments. In published studies, the pulmonary auscultatory skills of pulmonologists were found to be superior to those of medical students, and interns in internal medicine and general practice (Mangione & Nieman, 1997). Therefore, in this study only pulmonologists were included. Given the highly subjective nature of this interpretation, inter-listener variability restricts interoperability, with experience varying widely and differing across specialties (Sarkar et al., 2015; Hafke-Dys et al., 2019). Other sources of heterogeneity may originate from differences in the intrinsic properties of the stethoscope and extrinsic patient-related factors such as obesity, ambient noise, and patient compliance (e.g., crying child). Our study had some limitations. A higher number of patients would lead to more robust conclusions, and the inclusion of physicians from different specialties could confirm our results. It would also be interesting to see whether the type of the mask has an impact on the results. Further studies with more objective results could be obtained by using digital stethoscopes with recording capabilities to make comparison analysis of the breath sounds captured audio.
Conclusion
The results suggest that wearing surgical face masks during lung auscultation had no impact on agreement in pulmonologist assessment and is therefore an appropriate epidemiological measure in healthcare systems during the pandemic or in any environment with high risk of airborne infection. Wearing masks can enhance the safety of clinicians and health professionals from respiratory infections. Patients should be encouraged to wear masks because our study proved no significant differences in the physician assessment of auscultated breath sounds whether the patients wore a mask or not. Additionally, patients (particularly those who are susceptible) can lower their risk of infection by wearing masks while being certain that surgical mask will not “mask” their breath sounds. This was the first study where the influence of a surgical face mask on lung sound examination was assessed, and the results will reassure medical professionals in encouraging patients to wear a surgical face mask knowing it will not change auscultation findings.
Supplemental Information
10.7717/peerj.17368/supp-1Supplemental Information 1Raw data: auscultation summaryFindings from three pulmonologists coded 0,00; 1,00; 2,00; 0,10; 0,20. The complete physical finding, expiration length, and different sound phenomena, and whether the patient wore a mask or not.
10.7717/peerj.17368/supp-2Supplemental Information 2Raw data: auscultation expirationFindings from three pulmonologists. 1 is prolonged expirium and whether patient wore a mask or not.
10.7717/peerj.17368/supp-3Supplemental Information 3Raw data: auscultation sound phenomenaFindings from three pulmonologists regarding lung sound phenomena: wheezing, crackles and rales and whether patient wore a mask or not.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Arts L Lim EHT van de Ven PM Heunks L Tuinman PR 2020 The diagnostic accuracy of lung auscultation in adult patients with acute pulmonary pathologies: a meta-analysis Scientific Reports 101734710.1038/s 41598-020-64405-632355210 PMC 7192898 · doi ↗ · pubmed ↗
- 2Chu DK Akl EA Duda S Solo K Yaacoub S Schünemann HJ 2020 Physical distancing, and masks, face, and eye protection to prevent person-to-person transmission of SARS-Co V-2 and COVID-19: a systematic review and meta-analysis Lancet 395102421973198710.1016/S 0140-6736(20)31142-932497510 PMC 7263814 · doi ↗ · pubmed ↗
- 3European Centre for Disease Prevention and Control 2021 a Using face masks in the community: first update. 15 2021 ECDC Stockholm
- 4European Centre for Disease Prevention and Control 2021 b Infection prevention and control and preparedness for COVID-19 in healthcare settings –Sixth update. 9 2021 ECDC Stockholm
- 5Fajardo E Davis JL 2022 History and physical examination Murray & Nadel’s textbook of respiratory medicine Elsevier Inc Philadelphia Broaddus VC Ernst JD Jr TE King Lazarus SC Sarmiento KF Schnapp LM Stapleton RD Gotway MB 2412547 th edn
- 6Hafke-Dys H Breborowicz A Kleka P Kocinski J Biniakowski A 2019 The accuracy of lung auscultation in the practice of physicians and medical students PLOS ONE 148e 022060610.1371/journal.pone.022060631404066 PMC 6690530 · doi ↗ · pubmed ↗
- 7Jefferson T Del Mar CB Dooley L Ferroni E Al-Ansary LA Bawazeer GA van Driel ML Nair S Jones MA Thorning S Conly JM 2011 Physical interventions to interrupt or reduce the spread of respiratory viruses Cochrane Database of Systematic Reviews 11CD 00620710.1002/14651858.CD 006207.pub 6PMC 699392121735402 · doi ↗ · pubmed ↗
- 8Mangione S Nieman LZ 1997 Cardiac auscultatory skills of internal medicine and family practice trainees. A comparison of diagnostic proficiency JAMA 278971772210.1001/jama.1997.035500900410309286830 · doi ↗ · pubmed ↗