The Hepatic Imposter: Solitary Necrotic Nodules Masquerading as Hepatic Metastasis
Mohamed A Ebrahim, Eli A Zaher, Parth Patel, Omar Al Salman, Konrad Stelmark

TL;DR
A rare liver condition called solitary necrotic nodule was mistaken for cancer, highlighting the need for careful diagnosis to avoid unnecessary surgery.
Contribution
This case report highlights the diagnostic challenge of solitary necrotic nodules and emphasizes the role of biopsy in accurate diagnosis.
Findings
Solitary necrotic nodules can mimic metastatic tumors on imaging.
Needle biopsy confirmed the absence of malignancy in the reported case.
Abstract
Solitary necrotic nodules in the liver present a diagnostic challenge due to their rarity and resemblance to metastatic tumors. We report a case where imaging revealed multiple hepatic lesions suggestive of malignancy, prompting a needle biopsy. Histopathology confirmed necrosis without malignancy. Despite advancements in imaging modalities, distinguishing solitary necrotic nodules from metastases remains difficult. Recognition of characteristic imaging features and consideration of biopsy are crucial for accurate diagnosis and management. This case underscores the importance of thorough evaluation and differential diagnosis in liver lesions to prevent unnecessary surgical interventions and ensure appropriate clinical care.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1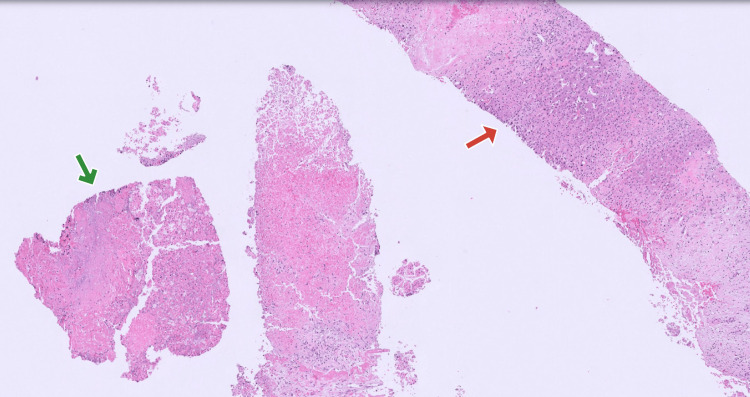 Figure 2
Figure 2| Component | Result | Reference range |
| Hemoglobin (g/dL) | 14.0 | 12.0-15.3 |
| White cell count (k/mm cu) | 9.0 | 4.0-11.0 |
| Mean corpuscular volume (f/L) | 90 | 80.0-100.0 |
| Platelets (k/mm cu) | 300 | 150-450 |
| Creatinine (mg/dL) | 3.5 | 0.6-1.2 |
| Sodium (mmol/L) | 135 | 133-144 |
| Albumin (g/dL) | 4.0 | 3.5-5.7 |
| Aspartate aminotransferase (IU/L) | 30 | 13-39 |
| Alanine aminotransferase (IU/L) | 42 | 7-52 |
| Total bilirubin (mg/dL) | 0.5 | 0.0-1.0 |
| Alkaline phosphatase (IU/L) | 100 | 35-104 |
| International normalized ratio | 1.0 | 0.9-1.1 |
| Lipase (IU/L) | 20 | 11-82 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Polyomavirus and related diseases · IgG4-Related and Inflammatory Diseases
Introduction
Necrotic hepatic nodules are rare benign lesions featuring a central necrotic core surrounded by a fibrotic capsule. Various theories about its origin have been proposed, including potential trauma, prior parasitic infection, or sclerosing hemangiomas. These nodules are often located beneath the liver capsule, slightly protruding from its surface, with distinct boundaries, occasionally leading to misinterpretation as metastatic growths [1]. Clinicians face challenges in accurate diagnosis due to the absence of distinctive clinical or radiological features [2,3]. Herein, we present a case of multiple necrotic hepatic nodules initially suspected to be of primary hepatic or metastatic origin in an elderly individual.
Case presentation
A 76-year-old obese male with a history of chronic kidney disease presented to the emergency department with complaints of intractable non-bloody vomiting and generalized abdominal pain for the preceding two weeks. He never had similar symptoms in the past and did not notice any relieving or exacerbating factors. No fevers or chills were reported. He denied using medications or illicit substances. He is a former 40-pack-year smoker and an occasional drinker.
Upon admission, vital signs were within normal limits. Physical examination was unremarkable. Blood work-up was consistent with an acute kidney injury, but was otherwise negative (Table 1).
CT of the abdomen without contrast showed multiple low-density hepatic lesions suspicious for a metastatic or primary tumor (Figure 1).
CT of the abdomen without contrast Multiple indeterminate low-density hepatic lesions, the largest measuring 7.5 cm. There is likewise moderate volume ascites seen
The patient was up to date on his colonoscopy screening, which is normal. He refused to have a repeat colonoscopy during the admission. Interventional radiology performed an ultrasound-guided needle biopsy of the liver, which showed necrosis without evidence of malignancy (Figure 2).
Liver histology Red arrow pointing towards an area of normal hepatic histology. Green arrow pointing towards an area of hepatic necrosis
Alpha-fetoprotein, carcinoembryonic antigen, and hepatitis panel were likewise negative. The patient recovered well with supportive management and was discharged home in good health.
Discussion
A solitary necrotic nodule in the liver is a rare finding during ultrasound or CT scans and is often mistaken for necrotic metastasis [3]. Despite its singular name, this type of nodule can sometimes be multiple [4]. In many instances, it signifies the final stage of various benign conditions like larval infestation, sclerosed hemangioma, or trauma. Under the microscope, the nodule typically comprises a fibrotic outer layer with inflammatory cells surrounding a central core of necrotic material. These nodules can appear beneath the liver's outer covering or within its deeper tissues [5].
Solitary necrotic nodules, classified as benign lesions with no documented instances of severe complications like malignant transformation, pose a diagnostic challenge. Therefore, it's crucial for radiologists to recognize the imaging characteristics associated with solitary necrotic nodules of the liver to prevent unnecessary surgical interventions. Solitary necrotic nodules in the liver typically manifest as small, well-defined lesions measuring under 3.0 cm, displaying a round, oval, or lobulated morphology [2,6]. Predominantly situated in the right lobe and often found in the liver's subcapsular regions, these nodules are primarily solitary, although rare cases of multiple lesions within one patient have been documented, as observed in this particular case [6].
Recent advancements in liver surgery have resulted in an increased number of individuals eligible for partial hepatic resection due to metastatic diseases. Imaging plays a pivotal role in providing detailed maps of hepatic metastases and aiding in the careful selection of patients before surgery, thus reducing unnecessary surgical exploration. Non-invasive imaging methods such as ultrasound, CT, and MRI have recently shown improvements in detecting hepatic metastases. Among these, CT arterial portography (CTAP) is recognized as the most sensitive for detecting focal liver lesions, although its high false-positive rate is seen as a drawback [7]. Intraoperative ultrasound has also been utilized to uncover small metastases not detectable through direct palpation or other preoperative imaging methods. Nevertheless, all of these radiological features of these modalities lack the specificity required for accurately characterizing liver tumors [8]. In our case, the radiological observations of the multiple necrotic nodules in the liver resembled those of hepatic metastasis. Distinguishing between solitary necrotic nodules and hepatic metastasis using any imaging modality is highly challenging, if not impossible, due to their similar features, including central hypoattenuation caused by necrosis and peripheral hyperattenuation attributed to fibrosis. These similarities underscore the need for a more precise diagnostic approach. As such, a needle biopsy becomes indispensable for achieving an accurate diagnosis in such cases.
Conclusions
Solitary necrotic nodules in the liver can appear as either single or multiple lesions on radiologic imaging, potentially leading to misinterpretation as metastatic hepatic tumors. The diagnostic challenge posed by solitary necrotic nodules in the liver highlights the importance of thorough evaluation and differential diagnosis during radiologic imaging. Their resemblance to metastatic hepatic tumors highlights the need for careful consideration and, when necessary, further confirmatory testing to ensure accurate diagnosis and appropriate clinical management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Solitary necrotic nodules of the liver mimicking hepatic metastasis: report of two cases Korean J Radiol Yoon KH Yun KJ Lee JM Kim CG 165168120001175294910.3348/kjr.2000.1.3.165PMC 2718187 · doi ↗ · pubmed ↗
- 2A challenging case of solitary necrotic nodules of the liver mimicking hepatic metastases: CT, MRI, and PET-CT findings J Belg Soc Radiol Hwang JY Lee JE Jung MJ 1610420203229287510.5334/jbsr.2088 PMC 7147685 · doi ↗ · pubmed ↗
- 3Solitary necrotic nodules of the liver simulating hepatic metastases J Clin Pathol Shepherd NA Lee G 11811183361983661931410.1136/jcp.36.10.1181 PMC 498498 · doi ↗ · pubmed ↗
- 4'Solitary' necrotic nodules of the liver: an aetiology reaffirmed Gut Sundaresan M Lyons B Akosa AB 13781380321991175247210.1136/gut.32.11.1378 PMC 1379172 · doi ↗ · pubmed ↗
- 5Solitary "necrotic nodule" of the liver: a probable pathogenesis J Clin Pathol Berry CL 12781280381985406698810.1136/jcp.38.11.1278 PMC 499427 · doi ↗ · pubmed ↗
- 6Clinical features of solitary necrotic nodule of the liver Hepatobiliary Pancreat Dis Int Zhou YM Li B Xu F 48548972008 https://pubmed.ncbi.nlm.nih.gov/18842494/18842494 · pubmed ↗
- 7Preoperative assessment of resectability of hepatic metastases from colonic carcinoma: CT portography vs sonography and dynamic CTAJR Am J Roentgenol Soyer P Levesque M Elias D Zeitoun G Roche A 7417441591992152983510.2214/ajr.159.4.1529835 · doi ↗ · pubmed ↗
- 8Detection of liver metastases: comparison of superparamagnetic iron oxide-enhanced and unenhanced MR imaging at 1.5 T with dynamic CT, intraoperative US, and percutaneous US Radiology Hagspiel KD Neidl KF Eichenberger AC Weder W Marincek B 4714781961995761786310.1148/radiology.196.2.7617863 · doi ↗ · pubmed ↗