Subvastus Arthrotomy and Multifaceted Fixation in Medial Femoral Comminuted Hoffa's Fracture: A Case Report
Siddharth K Patel, Sohael Khan, Ashutosh Lohiya, Ajay Koushik, Hardik Patel

TL;DR
A 45-year-old man with a rare knee fracture was successfully treated using a specific surgical approach and fixation techniques.
Contribution
This case report presents a successful surgical approach for a rare medial femoral comminuted Hoffa's fracture.
Findings
Subvastus arthrotomy and multifaceted fixation techniques were successfully used for the fracture.
The patient showed recovered knee function and radiographic signs of healing at one-year follow-up.
Abstract
In managing orthopedic trauma, Hoffa's fracture, a rare intra-articular fracture affecting the femoral condyle, presents a unique challenge. We report a case of a 45-year-old male patient who had a traumatic injury and complained of substantial knee discomfort and limited range of motion. The patient had a medial femoral comminuted Hoffa's fracture. Subvastus arthrotomy was employed to handle the fracture successfully, and then a locking reconstruction plate, Herbert screws, and 4 mm cannulated screws were used for precise reduction and fixation. At the one-year follow-up, the patient showed acceptable postoperative results, including recovered knee function and radiographic indications of fracture repair.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
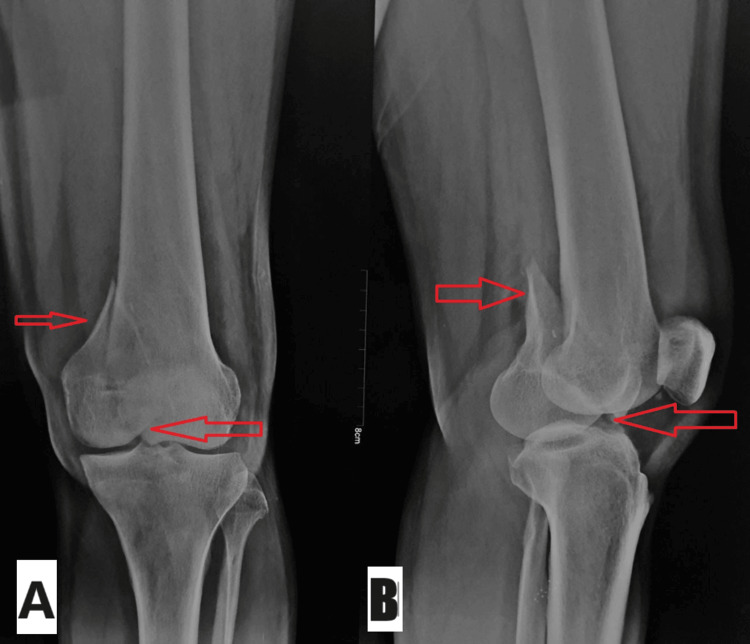 Figure 1
Figure 1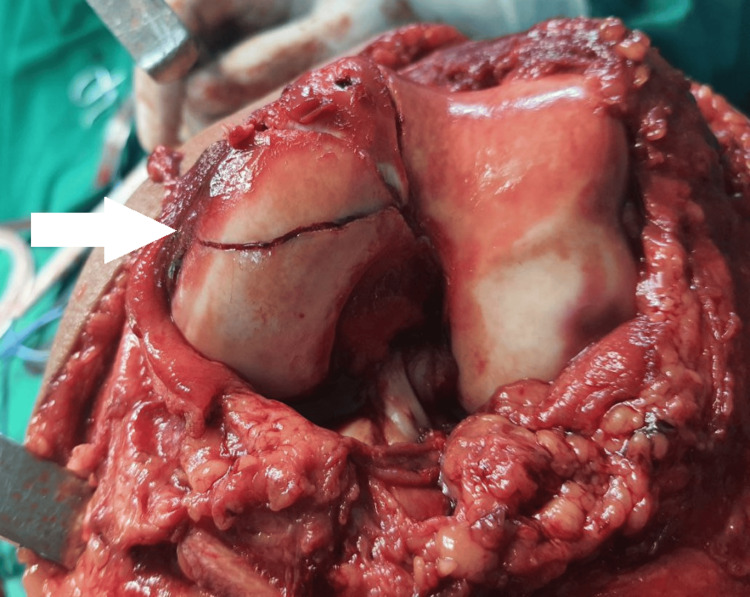 Figure 2
Figure 2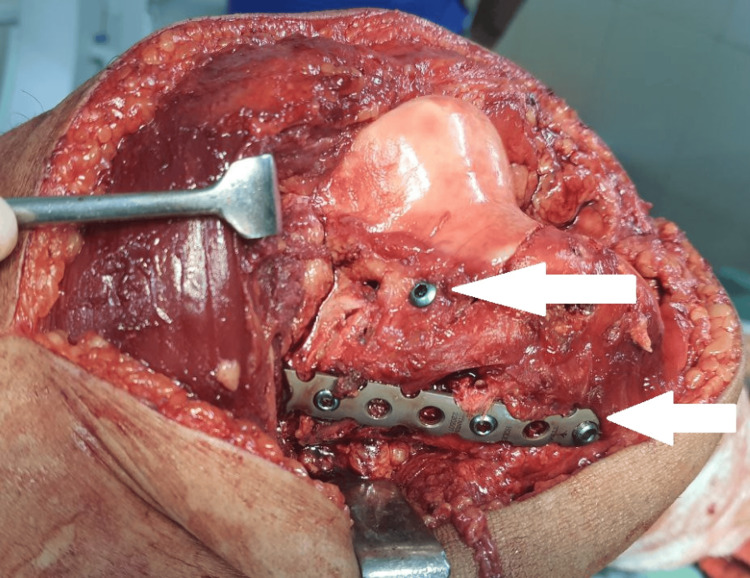 Figure 3
Figure 3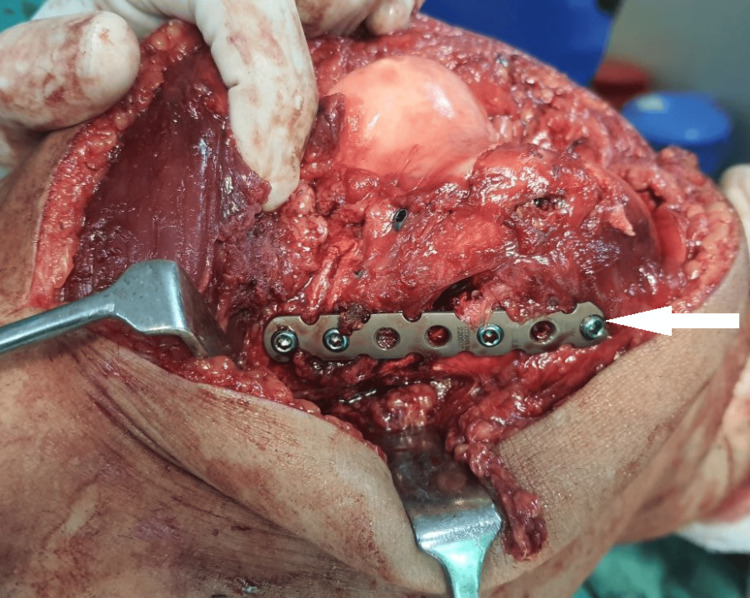 Figure 4
Figure 4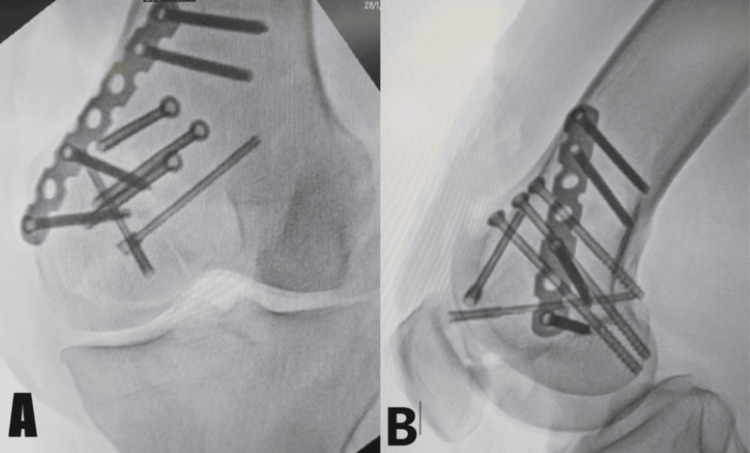 Figure 5
Figure 5 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHip and Femur Fractures · Bone fractures and treatments · Orthopaedic implants and arthroplasty
Introduction
The Hoffa fracture is named after Hoffa, who first reported it in 1904; it is defined as a femoral condyle fracture in the coronal plane affecting one or both condyles [1]. As the fracture is intra-articular and given the chance of potential articular cartilage damage, Hoffa's fractures affecting the medial femoral condyle present unique difficulties. These fractures are challenging to diagnose and sometimes go undetected on anteroposterior X-rays because the unfractured condylar section of the femur may obscure the broken condyle [2]. Such injuries are uncommon in adults and even rarer in teenagers; 8.7-13% of distal femur fractures are caused by them [3]. Owing to the knee joint's physiological genu valgus, injuries to the lateral condyle occur more frequently [4]. A Hoffa fracture is mostly caused by a high-energy trauma. It is advised to use surgical intervention, anatomical reduction, and solid fixation to lower the risk of issues such as osteonecrosis, nonunion, and arthritis [5].
Studies have documented the use of a range of surgical techniques, including open reduction and internal fixation (ORIF) with different implant configurations, to treat Hoffa cracks. Patients with comminuted Hoffa fractures, metaphyseal fracture extension, or low bone quality might be managed with hybrid fixation methods, which incorporate the use of a plate and screws [6,7]. For Hoffa fractures, ORIF is recommended regardless of the degree of fracture displacement, to anatomically restore the articular surface [8]. We report a case of comminuted Hoffa's fracture in the medial femur, which was fixed with 4 mm cannulated screws, a locking reconstruction plate, and Herbert screws by using a subvastus arthrotomy approach.
Case presentation
The patient was a 45-year-old male who presented at our institution's emergency room with acute left knee pain and edema following a fall from a height. The initial examination revealed a limited range of motion, edema over the knee, discomfort over the medial femoral condyle, and evidence of an intra-articular fracture. The patient had no prior history of hospitalization and no known comorbidities. An X-ray of the left knee taken from the lateral and anteroposterior views validated the radiographic assessment of diagnosing a medial femoral comminuted Hoffa's fracture with significant displacement and joint involvement, as shown in Figure 1.
Preoperative X-ray of the left kneeThe anteroposterior (A) and lateral (B) views. The red arrows show medial femoral comminuted Hoffa's fracture with substantial displacement and joint involvement
To stabilize the fracture, the patient was first treated with an above-knee slab, following which he was admitted. The patient was managed with a subvastus arthrotomy approach combined with fixation using 4 mm cannulated screws, Herbert screws, and a locking reconstruction plate. He was put under spinal anesthesia, put in a supine position on an operative theatre (OT) table, and had a tourniquet applied to the left thigh. The knee joint was accessed via a subvastus arthrotomy technique, which preserved the extensor mechanism and reduced soft tissue damage and fracture, as shown in Figure 2.
Intraoperative image - 1The white arrow shows the fracture in the intra-articular surface of the medial femoral condyle
The extent of the fracture was established by intraoperative fluoroscopy, and then anatomical reduction forceps and manual manipulation were used to reduce the fracture carefully. The fracture was then stabilized by applying a locking reconstruction plate in a buttress shape, 4 mm cannulated screws, and Herbert screws to support the comminuted pieces and restore joint congruity, as shown in Figure 3 and Figure 4.
Intraoperative image - 2The white arrow shows the fracture stabilized by a reconstruction plate and Herbert screws
Intraoperative image - 3The white arrow shows the fracture stabilized by a locking reconstruction plate and Herbert screws
Following surgery, the patient followed a planned rehabilitation program that included crutch-assisted partial weight-bearing, range-of-motion exercises, and early mobilization. Regular radiographic evaluation showed increasing fracture healing and joint alignment restoration. At the one-year follow-up, the patient reported a significant improvement in knee function, minimal pain persistence, and a manageable range of motion. Signs of remodeling and fracture union were seen on radiographs, indicating a successful surgical intervention, as shown in Figure 5 and Figure 6.
Postoperative X-raysAnteroposterior (A) and lateral (B) views show fracture reduction done by the locking reconstruction plate in a buttress shape, 4 mm cannulated screws, and Herbert screws
Follow-up postoperative X-ray at one yearAnteroposterior (A) and lateral (B) views show the united fracture with a locking reconstruction plate in a buttress shape, 4 mm cannulated screws, and Herbert screws in situ
Discussion
A Hoffa's fracture is a complex intra-articular fracture involving the weight-bearing surface of the femoral condyle, also known as a coronal fracture of the femoral condyle. These fractures usually result from high-energy trauma from car crashes or falls from considerable heights. These fractures are complicated due to their locations and how the injury was sustained, potentially making treatment difficult and raising the possibility of adverse effects. A major problem with Hoffa's fractures is the increased risk of complications like nonunion, malunion, and avascular necrosis. It is rare to have a medial femoral condyle coronal fracture in isolation, leaving the lateral condyle intact [9]. Given the possibility of articular incongruity, posttraumatic arthritis, and functional impairment, Hoffa's fractures remain a challenge to treat.
No surgical approach or fixing technique has been generally acknowledged to provide the best results in these patients [10]. Nonetheless, several strategies have been used to treat these intricate fractures. Although there is a chance of neurovascular damage, direct lateral/medial and posterolateral methods have the benefit of improved visualization and access to smaller Hoffa fragments. To offer even more stability, a plate may occasionally be utilized in conjunction with posterior-anterior direction screws [11].
The subvastus arthrotomy approach was used in our case to minimize soft tissue disturbance and provide sufficient exposure to the fracture site. This method, along with the use of Herbert screws, 4 mm cannulated screws, and a locking reconstruction plate, allowed for early mobilization and stable fixation, leading to favorable clinical outcomes. The subvastus arthrotomy and combination of screws and locking reconstruction plate utilized in this case's surgical technique allowed for sufficient exposure and solid fixation, eventually resulting in positive results.
Conclusions
Medial femoral comminuted Hoffa's fractures are uncommon but challenging orthopedic injuries that need to be recognized promptly and treated surgically if required. Subvastus arthrotomy offers a viable therapeutic option with the potential for good clinical results and fracture union when paired with fixation utilizing 4 mm cannulated screws, Herbert screws, and a locking reconstruction plate. More research is necessary to assess this method's long-term effects in treating Hoffa's fractures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hoffa fracture in skeletally immature patients: a case report and review of literature J Orthop Case Rep Ranjan R Kumar R Jeyaraman M Jain R Chaudhary D Kumar S 1121181120213414168410.13107/jocr.2021.v 11.i 02.2050 PMC 8180317 · doi ↗ · pubmed ↗
- 2Hoffa fracture of the femoral condyle: injury mechanism, classification, diagnosis, and treatment Medicine (Baltimore) Zhou Y Pan Y Wang Q Hou Z Chen W 098201910.1097/MD.0000000000014633 PMC 640808830813201 · doi ↗ · pubmed ↗
- 3Operative management of Hoffa fractures--a prospective review of 18 patients Injury Gavaskar AS Tummala NC Krishnamurthy M 149514984220112199336810.1016/j.injury.2011.09.005 · doi ↗ · pubmed ↗
- 4Hoffa fractures are associated with concomitant soft tissue injures and a high postoperative complication rate Arch Orthop Trauma Surg Neumann-Langen MV Eggeling L Glaab R von Rehlingen-Prinz F Kösters C Herbst E 74775414420243809308910.1007/s 00402-023-05133-0PMC 10822794 · doi ↗ · pubmed ↗
- 5Hoffa nonunion, two cases treated with headless compression screws J Knee Surg Somford MP van Ooij B Schafroth MU Kloen P 09326201310.1055/s-0032-131978123288759 · doi ↗ · pubmed ↗
- 6Repair of displaced partial articular fracture of the distal femur: the Hoffa fracture J Orthop Trauma Egol KA Broder K Fisher N Konda SR 0131201710.1097/BOT.000000000000089628697072 · doi ↗ · pubmed ↗
- 7Analysis of functional outcome of Hoffa fractures: a retrospective review of 32 patients J Orthop Surg (Hong Kong) Trikha V Das S Gaba S Agrawal P 4625201710.1177/230949901771892828673200 · doi ↗ · pubmed ↗
- 8A rare case of open bicondylar Hoffa fracture with extensor mechanism disruption BMJ Case Rep Kini SG Sharma M Raman R 24262013201310.1136/bcr-2013-009541 PMC 366988623645653 · doi ↗ · pubmed ↗