Rituximab as a First-line Treatment for Autoimmune Hemolytic Anemia in Multicentric Castleman's Disease
Jose L Cáceres Medina, Luis A González Torres, Alan Gamboa-Meza, Olga G Cantu-Rodriguez

TL;DR
A 53-year-old woman with rare multicentric Castleman's disease and autoimmune hemolytic anemia was successfully treated with rituximab and steroids as first-line therapy.
Contribution
This is the first reported case of successful first-line rituximab treatment for concurrent multicentric Castleman's disease and autoimmune hemolytic anemia.
Findings
The patient showed clinical and laboratory improvement within seven days of rituximab and steroid treatment.
The case highlights the potential of rituximab as an effective first-line therapy for this rare comorbid condition.
The patient was discharged early following successful treatment outcomes.
Abstract
Castleman´s disease (CD) is a rare lymphoproliferative disorder. Concurrent autoimmune disease and CD are uncommon, but even more so, comorbid CD and autoimmune hemolytic anemia (AIHA). To the best of our knowledge, this case represents the first successful AIHA and multicentric CD (MCD) treatment using rituximab as first-line treatment. We present the case of a 53-year-old woman with a 10-year history of plasma cell variant CD who arrived at the emergency department with signs and symptoms of anemia. On admission, we made a preliminary diagnosis of hemolytic anemia and initiated immunosuppressive therapy with rituximab and steroids. After seven days, the patient recovered according to clinical and laboratory parameters, and we discharged her early. We portray a rare occurrence of CD and AIHA successfully treated with rituximab and steroid therapy, which makes our case unique.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
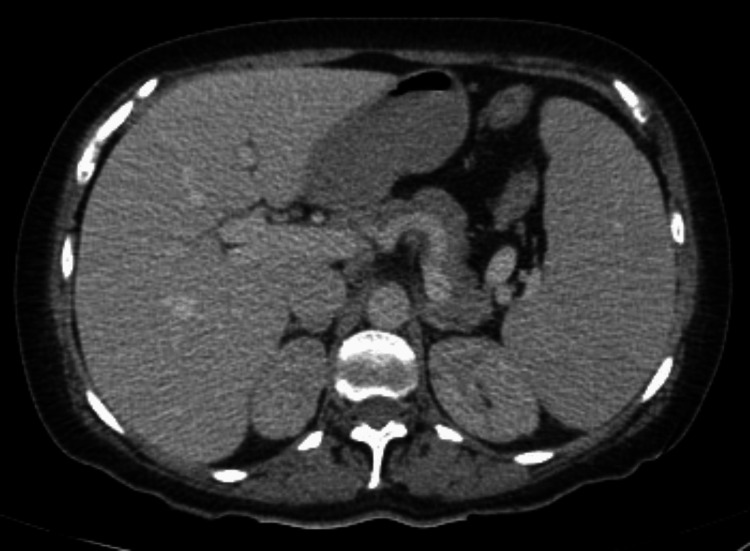 Figure 1
Figure 1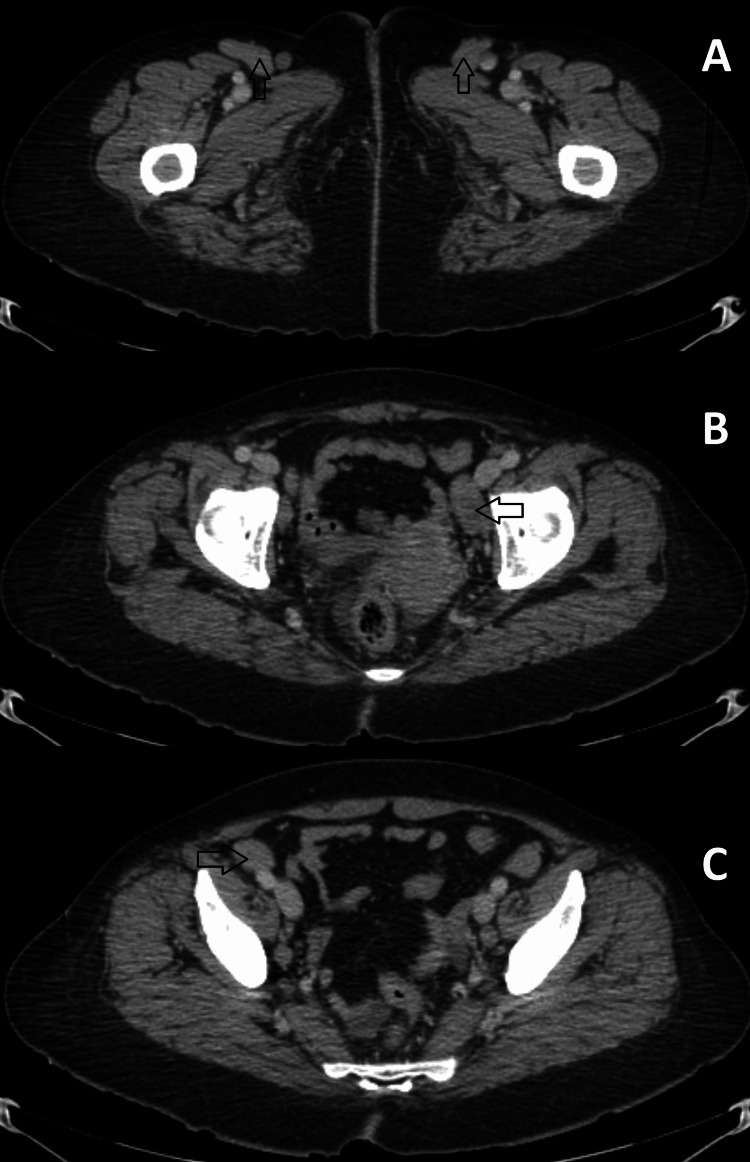 Figure 2
Figure 2| Case Report | Description |
| Tajima et al. [ | A 50-year-old male with MCD + AIHA; CHOP-R success, Rituximab may have contributed to AIHA remission. |
| Tabata et al. [ | A 43-year-old with MCD + AIHA; tocilizumab failure, success using rituximab. |
| Plano et al. [ | A 72-year-old male with MCD + AIHA; rituximab failure, success using siltuximab. |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood groups and transfusion · Viral-associated cancers and disorders · Parvovirus B19 Infection Studies
Introduction
Castleman disease (CD) is a rare lymphoproliferative disorder classified into two types: unicentric CD (UCD) and multicentric CD (MCD). There are three histologic subtypes: hyaline vascular (80%), plasma cell (10%), and mixed variants [1]. Autoinflammatory mechanisms may play an essential role in its development, as evidenced by a systematic review of 1923 cases reported in 38 patients with positive autoantibodies or autoimmune hemolytic anemia [2,3]. A few cases describe simultaneous autoimmune hemolytic anemia (AIHA) and CD occurrence.
Our case portrays this rare clinical scenario with the added value of treatment experience using rituximab and steroids. Two other case reports have reported the direct intention of using rituximab as a treatment, of which one was successful. This case describes the first successful treatment of AIHA and MCD using rituximab as first-line treatment.
Case presentation
A 53-year-old woman with a 10-year history of "plasma cell variant CD" presented to the Emergency Department (ED) with a three-month history of fatigue, moderate effort-dependent dyspnea, and new-onset jaundice the day before the presentation.
On admission, her vital signs showed tachycardia with no other abnormalities. The physical examination revealed generalized jaundice, hepatosplenomegaly, and bilateral superficial inguinal adenopathies. The laboratory results showed regenerative macrocytic anemia (hemoglobin: 3.4 g/dL, mean corpuscular volume: 110 fL, reticulocytes: 45%), elevated lactate dehydrogenase (LDH), indirect hyperbilirubinemia (total bilirubin: 5.0 mg/dL, direct bilirubin: 0.3 mg/dL, indirect bilirubin: 4.7 mg/dL, LDH: 376 U/L), and normal liver enzymes. We performed a Coombs test, which yielded a triple cross-positive result. Subsequently, we conducted a monospecific IgG test, which confirmed warm antibody AIHA. Hematology recommended administering dexamethasone at 40 mg every 24 hours for four days, followed by a daily dosage of 75 mg of prednisone. Rituximab was advised at a dose of 600 mg weekly for four weeks, along with a CD assessment. An abdominal computed tomography (CT) was performed, revealing hepatosplenomegaly and bilateral inguinal and external iliac lymph nodes (Figure 1 and Figure 2).
Contrast-enhanced abdominal CT scan in venous phase demonstrating hepatosplenomegaly, enlarged liver (21.4 x 17.5 cm) and spleen (17.1 x 15.2 cm)
Contrast-enhanced abdominal CT scan in venous phase showing multiple adenopathies(A) Right (3.8 x 1.3 cm) and left (2.9 x 1.4 cm) inguinal adenopathies (arrows); (B) Left external iliac adenopathy (2.9x 1.4 cm) (arrow); (C) Right external iliac adenopathy (2.6 x 1.8 cm) (arrow).
After seven days, the patient recovered substantially and exhibited no AIHA activity. By the third and 12th-month follow-up visits, we had detected no CD or AIHA activity.
Discussion
We presented a case of comorbid CD and AIHA treated with rituximab as a first-line therapy. To the best of our knowledge, this case represents the first successful AIHA-MCD treatment using rituximab and should serve as a guide when encountering patients with similar clinical characteristics. Our main challenge was the inability to attribute the complete response to rituximab therapy solely. Additionally, the lack of histopathological imaging for the excisional biopsy of adenopathies posed another limitation in our case.
Anemic disorders are a frequent feature of the plasma cell variant of CD, but hemolytic anemia is not a common finding in CD [3]. Arthritis, proteinuria, Sicca syndrome, polyneuropathy (without diagnosing POEMS (Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal gammopathy, and Skin abnormalities) syndrome), interstitial lung disease, immune thrombocytopenic purpura, and AIHA are all autoimmune characteristics of MCD. Comorbid autoimmune diseases in CD include myasthenia gravis, psoriasis, amyloidosis, sarcoidosis, and others [4]. Liu et al. discovered that among 1923 CD cases, 38 exhibited autoantibodies indicative of AIHA [2]. Another large series of patients with UCD reported AIHA in only one out of 71 patients [5].
The literature shows more than 10 cases of AIHA with CD and four cases of Evans syndrome with CD. Treatment consistently involves steroids, with varying use of tocilizumab, rituximab, or chemotherapy. In a few reported persistent cases, splenectomy was the definitive treatment. Our patient presented with MCD and AIHA, and we decided to treat her with steroids and rituximab, to which she had a prolonged response. Monoclonal therapies appear to be therapeutical options when considering autoimmune coexistence with MCD. Table 1 summarizes monoclonal antibody use in CD presenting with AIHA [6-8].
Steroid therapy represents the initial treatment choice for AIHA. A comparative analysis from a small clinical trial examined the effectiveness of prednisolone alone versus a combination with rituximab therapy. The trial reported a success rate of 36% with prednisolone alone, contrasting significantly with a success rate of 75% when combined with rituximab therapy within 12 months [9].
A study by Barcellini et al., encompassing 308 cases of AIHA, pointed out that the emergence of severe anemia at disease onset is associated with elevated hazard ratios for relapse and an increased requirement for therapeutic interventions [10]. Additionally, their evaluation reported a 14% increase in relapse risk for every gram reduction of hemoglobin.
Given the rarity of similar cases, MCD activity proof, and the presentation of severe anemia, we opted to initiate second-line treatment as the primary approach. We observed a good response after 12 months.
Conclusions
We encountered a clinical scenario where a well-known disease met with a rarer one. Physicians should consider a diagnosis of AIHA in patients with a history of MCD, severe anemia, and constitutional signs. Rituximab is a viable first-line option for treating AIHA related to MCD. Little evidence supports monoclonal body use in AIHA and active MCD, and this case report presents the first successful experience of rituximab as a first-line treatment. Further knowledge, case reporting, and evidence review are needed when considering concomitant MCD with AIHA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Rituximab in the treatment of autoimmune haemolytic anaemia Br J Clin Pharmacol Rodrigo C Rajapakse S Gooneratne L 7097197920152513961010.1111/bcp.12498 PMC 4415708 · doi ↗ · pubmed ↗
- 2Idiopathic multicentric Castleman’s disease: a systematic literature review Lancet Haematol Liu AY Nabel CS Finkelman BS 0753201610.1016/S 2352-3026(16)00006-527063975 · doi ↗ · pubmed ↗
- 3Novel insights and therapeutic approaches in idiopathic multicentric Castleman disease Blood Fajgenbaum DC 2323233013220183048712910.1182/blood-2018-05-848671 PMC 6265649 · doi ↗ · pubmed ↗
- 4Idiopathic multicentric Castleman disease and associated autoimmune and autoinflammatory conditions: practical guidance for diagnosis Rheumatology (Oxford) González García A Fernández-Martín J Robles MarhuendaÁ 142614356220233599756710.1093/rheumatology/keac 481PMC 10070070 · doi ↗ · pubmed ↗
- 5Treatment and outcome of unicentric Castleman disease: a retrospective analysis of 71 cases Br J Haematol Boutboul D Fadlallah J Chawki S 26927318620193101673010.1111/bjh.15921 · doi ↗ · pubmed ↗
- 6Autoimmune hemolytic anemia with warm-reactive immunoglobulin M antibody in multicentric Castleman disease Ann Hematol Tajima K Yamamoto H Suzuki I 8498519220132318043510.1007/s 00277-012-1626-8 · doi ↗ · pubmed ↗
- 7Idiopathic multicentric Castleman disease with autoimmune hemolytic anemia and production of anti-drug antibody against tocilizumab Intern Med Tabata S Higuchi T Tatsukawa S Narimatsu K Takeo H Matsukuma S Ito T 331333185820193129238910.2169/internalmedicine.2989-19PMC 6911740 · doi ↗ · pubmed ↗
- 8A multicentric Castleman disease associated with mixed warm and cold antibody-mediated aha responsive to siltuximab Chemotherapy Plano F Mancuso S Camarda GM 35396920243763449210.1159/000533235 · doi ↗ · pubmed ↗