Yearlong Near-Syncope: Presentation of a Rare Right Atrial Myxoma
Vishal V Bandaru, Sophie L Talbot, Ricardo I Garcia, Luis J Carbajal, Pooja Sethi

TL;DR
A rare case of a right atrial myxoma causing long-term near-syncope symptoms is reported in a 67-year-old woman.
Contribution
This case highlights the importance of considering right atrial myxomas in the differential diagnosis of persistent syncope-like symptoms.
Findings
A 4.3 x 4.0 cm right atrial myxoma was diagnosed in a patient with yearlong near-syncope.
Surgical resection and immunohistochemistry confirmed the diagnosis of myxoma.
The case emphasizes the need to include right atrial myxomas in syncope differentials.
Abstract
Atrial myxomas are the most common form of primary benign cardiac tumors. The left atrium is typically the most common location while right atrial myxomas are much rarer and only occur in about 15%-25% of all myxoma patients. Typically, left atrial myxomas have the ability to cause symptoms such as syncope. We report a case of a 67-year-old female who presented with complaints of palpitations, dizziness, and near-syncope that had been ongoing for about a year. Other causes of syncope were investigated and ruled out. A transthoracic echocardiogram (TTE) found a large 4.3 x 4.0 cm spherical mass in the right atrium which was confirmed by surgical resection and immunohistochemistry to be a myxoma. The patient's condition of syncope-like symptoms warrants elevating atrial myxomas to a higher position in the diagnostic differential.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
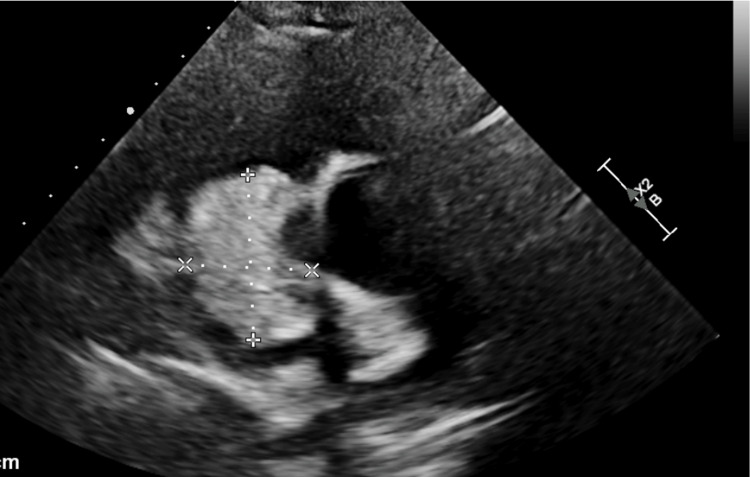 Figure 1
Figure 1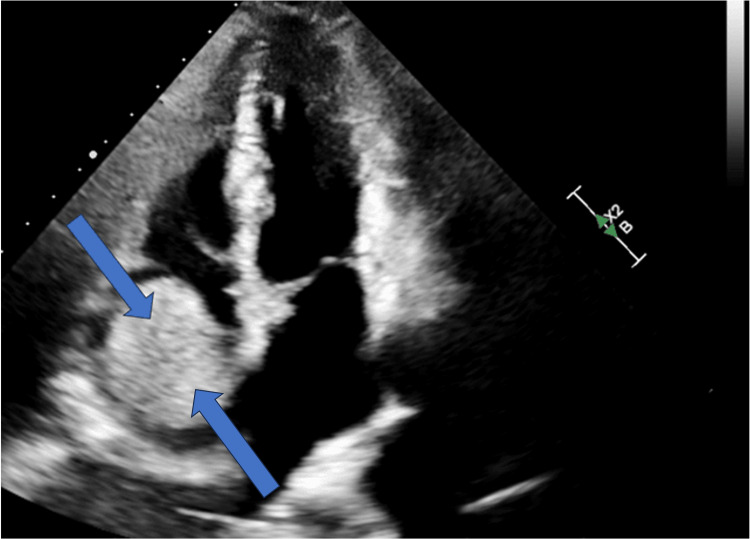 Figure 2
Figure 2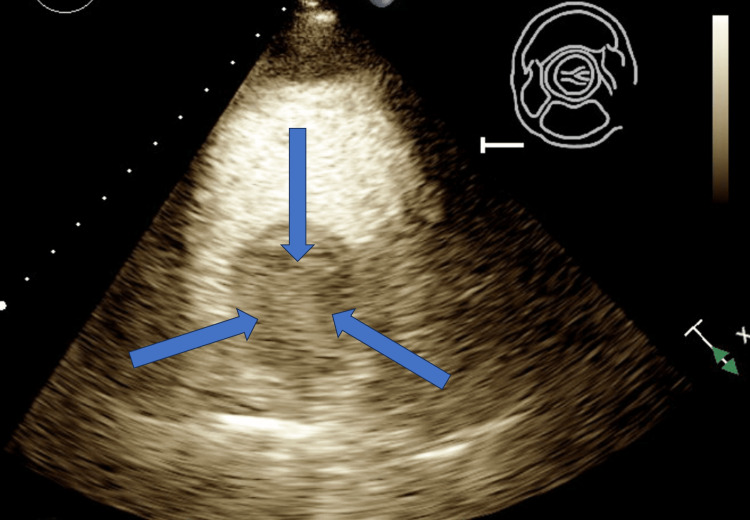 Figure 3
Figure 3 Figure 4
Figure 4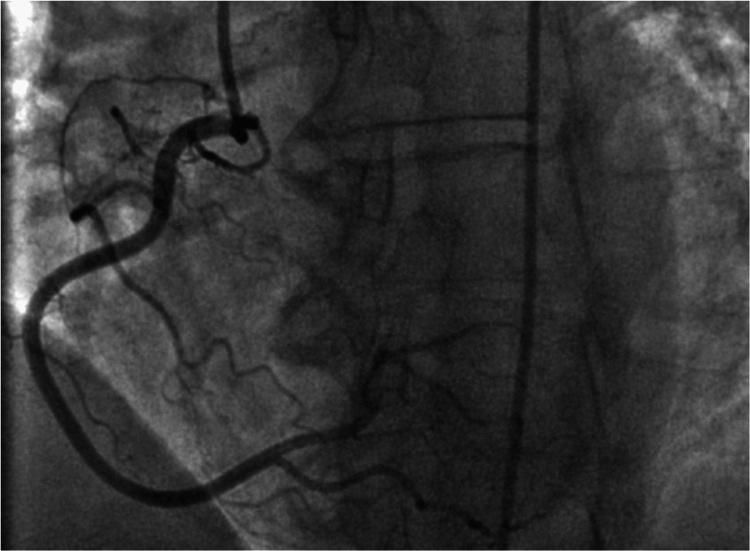 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Venous Thromboembolism Diagnosis and Management · Cardiac Arrhythmias and Treatments
Introduction
Cardiac tumors are rare; the incidence of tumors found on autopsies ranges from 0.001% to 0.3% and are reported to be 0.2% of all tumors found in humans. Roughly 75% of cardiac tumors are benign. Approximately 50% of these benign tumors are myxomas [1-5]. Characteristic findings of atrial myxomas include syncope, dizziness, orthopnea, pulmonary edema, cough, palpitations, fatigue, hemoptysis, and chest pain. Many of these findings are influenced by changing positions. Right atrial myxomas have been found to be associated with abdominal distension due to ascites [2,4]. Another study evaluating atrial myxomas found a neurological symptom rate of 16.9% with cerebral infarction being the most common complication among neurological conditions [6]. Auscultation can reveal a “tumor plop” heart murmur [4]. Diagnostically, atrial myxomas have generally been found via 2D-Echocardiograms such as a transthoracic echocardiogram (TTE), transesophageal echocardiogram (TEE), or via computerized tomography (CT) or magnetic resonance imaging (MRI) [7].
Case presentation
The patient is a 67-year-old female with a past medical history of hypertension (HTN), hyperlipidemia (HLD), type 2 diabetes (DM2), and Parkinson’s Disease who was admitted to the hospital in December 2022 for evaluation of palpitations associated with dizziness and near-syncope ongoing for one year. Episodes at onset lasted a few minutes before spontaneously resolving but worsened over the year in frequency and duration. She was referred to an outpatient cardiology clinic in December 2022 where a transthoracic echocardiogram (TTE) showed a right atrial mass concerning myxoma. The patient was sent to the emergency center for further evaluation and subsequently admitted for cardiovascular surgery evaluation. The physical examination was negative for murmurs, rubs, gallops, or clicks. An electrocardiogram (ECG) was unremarkable, and vitals were stable. Lab workup showed mildly elevated pro-brain natriuretic peptide (proBNP) of 259 pg/mL but otherwise was unremarkable.
A repeat TTE was done after admission which revealed a large 4.3 x 4.0 cm spherical mass arising in the right atrium and a small pericardial effusion without tamponade physiology. This mass appeared at least partially vascularized in echo contrast, raising suspicion of a myxoma (Figures 1-3).
TTE parasternal short axis view at the level of the aortic valve depicting a large 4.3 x 4.0 cm spherical mass arising in the right atriumTTE: transthoracic echocardiogram
Apical four-chamber view of TTE again depicting a large mass in the right atrium (blue arrows)TTE: transthoracic echocardiogram
TTE parasternal short axis view at the level of the aortic valve with IV contrast depicting partially vascularized right atrial mass concerning myxoma (blue arrows)TTE: transthoracic echocardiogram
Tissue Doppler imaging showed a mitral inflow pattern consistent with impaired relaxation of the left ventricle associated with grade I (mild) diastolic dysfunction. Left heart catheterization (LHC) was performed which showed no significant coronary artery disease (Figures 4, 5). There were normal cardiac filling pressures, normal ejection fraction (EF) without regional wall motion abnormalities, and normal coronary arteries.
Right anterior oblique (RAO) view of left heart catheterization (LHC) with no significant left coronary artery disease
Left anterior oblique (LAO) view of the left heart catheterization (LHC) with no significant right coronary artery disease
Our patient was placed on cardiopulmonary bypass and underwent sternotomy with successful resection of the right atrial singular circular mass. No other evidence of masses was found. No blood was given intra-operatively or post-operatively due to the patient’s status as a Jehovah’s Witness. Frozen sections of the excised mass were sent to pathology; three different specimens were selected and the sections showed polygonal/stellate myxoma (lepidic) cells around blood vessels within the myxoid stroma, positive for Calretinin stain, consistent with cardiac myxoma. In additional stains, S100 was negative and CD 68 highlighted scattered histiocytes. The immunohistochemistry (IHC) supported the diagnosis of an atrial myxoma. There were no post-operative complications and the patient was discharged home in stable condition after three days.
Discussion
Syncope is considered a rare manifestation of right atrial myxomas, seen in approximately 20% of cases [8-10]. Many case studies have found right atrial myxomas with a history of syncope and/or heart palpitations [8-13]. However, the absence of thromboembolic causes of syncope or common clinical findings suggestive of alternate etiologies of syncope should allow myxomas to be included higher in the differential, particularly in older patients [8]. Near-syncope symptomatology, over a long period of time, may need to garner further attention to right atrial myxomas as a possible cause. While syncope could be associated with reflex syncope, orthostatic hypotension, drug interactions, or dehydration, if the evaluation of the patient is still not explained or has additional cardiac symptomatology, a TTE may be a viable and easy mechanism for the diagnosis of myxomas [14].
Between 75-80% of myxomas are found in the left atrium and 15-20%, are located in the right atrium. Though myxomas may appear in other areas such as ventricular, biatrial, and multilocular locations, these myxomas represent an incredibly small proportion of cases [15]. Atrial myxomas have been found more often in women and over the atrial septum [4]. Generally, left atrial myxomas can cause syncope due to occlusion of the mitral valve. However, our case is most likely caused by a partial occlusion of the superior vena cava. Right atrial myxomas can cause symptoms resembling syncope if there is an obstruction to either the mitral valve or superior vena cava.
Our specific case had no irregularities in the myxoma in regards to the shape, size, and IHC. This myxoma was round, a shape that has been commonly reported in the literature: myxoma shapes have been recorded as round, multilobulated, or other irregular shapes. The size was within the reported literature value ranges (5.1 cm + 1.8 cm diameter) [16]. However, the presence of vascularization in the myxoma observed during contrast echo is an interesting finding. Due to the similarity in IHC between atrial myxomas and mural thrombi with myxoid stroma, the calretinin marker is specifically used for the differential, which was positive in our histochemistry. Other diagnostic considerations include intracardiac thrombi, rhabdomyomas, lipomas, sarcomas, or B-cell lymphomas [4,17]. Survival for patients with atrial myxomas is quite good at around 96% for a 10-year survival period and surgical interventions usually resolve symptoms [18].
Conclusions
The prevalence of right atrial myxomas is considerably less than that of left atrial myxomas. Older, female patients are more likely to have atrial myxomas. Surgical resection is often the choice of treatment for suspected myxomas which has historically resolved symptoms. Excisional biopsy and IHC are often necessary to confirm the diagnosis of a myxoma and exclude other possibilities. Our patient's yearlong palpitations and near-syncope symptoms were finally resolved post-surgery, but the duration of the symptomatology begs the overall question of differentials. This symptomatology warrants a deeper investigation into placing myxomas higher in the diagnostic differential for older patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Malignant cardiac tumors (Article in Portuguese)Rev Bras Cir Cardiovasc Lima PR Crotti PL 6473192004
- 2Atrial myxoma presenting with palpitations: a case report Cureus Prousi GS Moran JV Biggs RG 011201910.7759/cureus.4093 PMC 647271731032153 · doi ↗ · pubmed ↗
- 3Cardiac myxoma: a 13-year experience in echocardiographic diagnosis Rev Port Cardiol Oliveira R Branco L Galrinho A 10871100292010 https://www.ncbi.nlm.nih.gov/pubmed/2106696421066964 · pubmed ↗
- 4Atrial myxoma Stat Pearls Nguyen T Vaidya Y Treasure Island, FL Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 556040/
- 5Left atrial and right ventricular myxoma: an uncommon presentation of a rare tumour Interact Cardiovasc Thorac Surg Diaz A Di Salvo C Lawrence D Hayward M 6226231220112127325610.1510/icvts.2010.255661 · doi ↗ · pubmed ↗
- 6Neurological manifestations of atrial myxoma: a retrospective analysis Oncol Lett Wen XY Chen YM Yu LL 463546391620183021459810.3892/ol.2018.9218 PMC 6126161 · doi ↗ · pubmed ↗
- 7Giant left atrial myxoma - literature review and case presentation Rom J Morphol Embryol Raicea VC Suciu H Raicea AD Macarie GC Mezei T Maier MS 3613686220213502472410.47162/RJME.62.2.02PMC 8848268 · doi ↗ · pubmed ↗
- 8Right atrial myxoma and syncope Am J Case Rep Babs Animashaun I Akinseye OA Akinseye LI Akinboboye OO 6456471620152639007610.12659/AJCR.894513 PMC 4582919 · doi ↗ · pubmed ↗