A Case of Tubercular Pericardial Tamponade With Anti-tuberculosis Treatment-Induced Hepatitis
Daniel Hijam, Supongbenla Supongbenla, Doyen Soram

TL;DR
This case study describes a patient with tuberculosis-related pericardial tamponade who also developed liver damage from anti-tuberculosis treatment.
Contribution
The paper presents a rare clinical case of TB-induced pericardial tamponade complicated by drug-induced hepatitis.
Findings
Pericardial fluid testing confirmed Mycobacterium TB using ADA and CBNAAT.
The patient developed ATT-induced hepatitis requiring modified treatment.
The patient showed clinical improvement after treatment adjustments.
Abstract
Pericarditis can be a common complication of tuberculosis (TB) in developing countries like India. It is associated with fever, fatigue, and weight loss and can often be accompanied by shortness of breath and chest pain. Other common causes of pericardial effusion include malignancy, renal failure, autoimmune disease, and viral and bacterial infections. When the pericardial fluid is bloody, TB is likely to be present in developing countries. It can often get complicated with cardiac tamponade, which has a high mortality rate. We present a case of a 55-year-old female with no co-morbidities who presented with shortness of breath, fatigue for two weeks, and chest pain for one week. She had no history of fever, chills, or rigour, and no history of TB contact. Clinical examination revealed low blood pressure with raised jugular venous pressure (JVP). Her electrocardiography (ECG) showed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
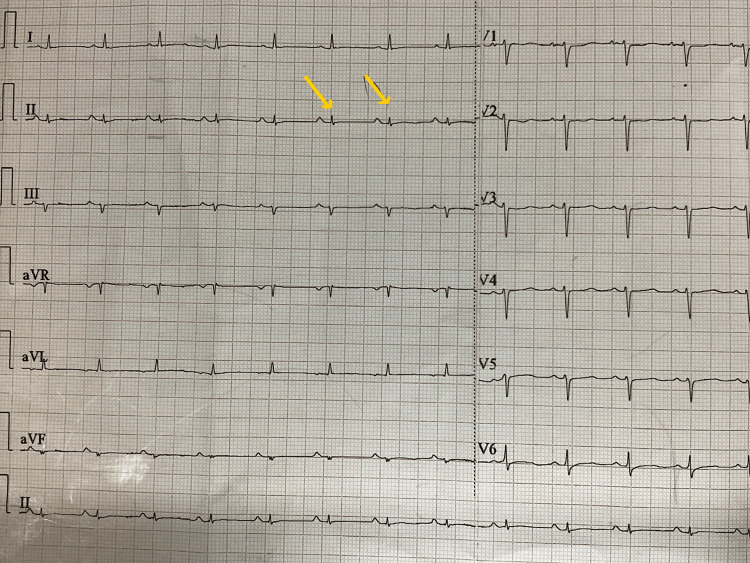 Figure 1
Figure 1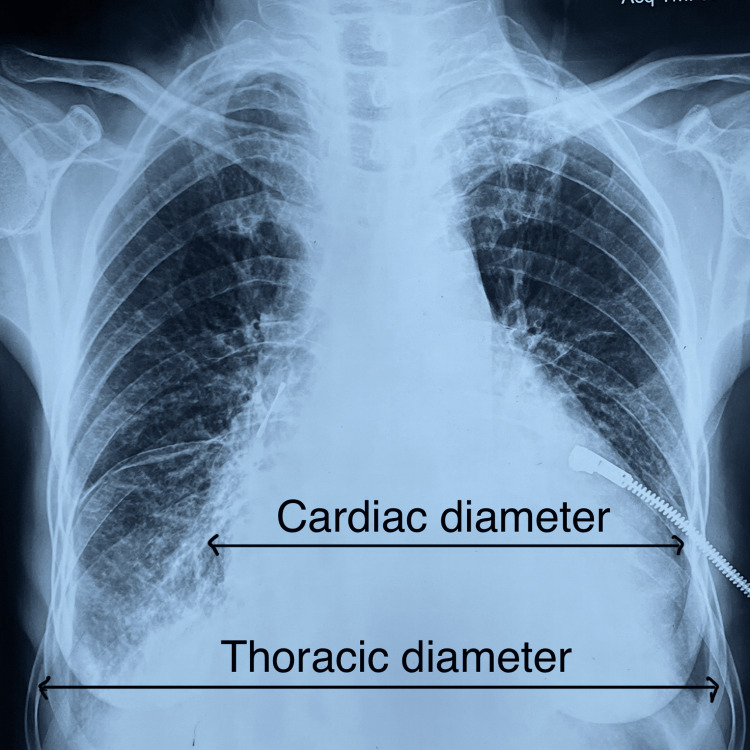 Figure 2
Figure 2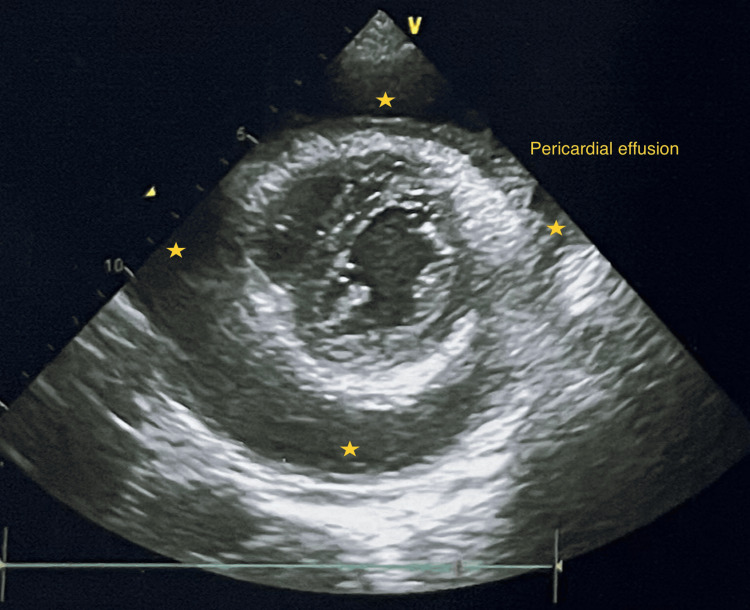 Figure 3
Figure 3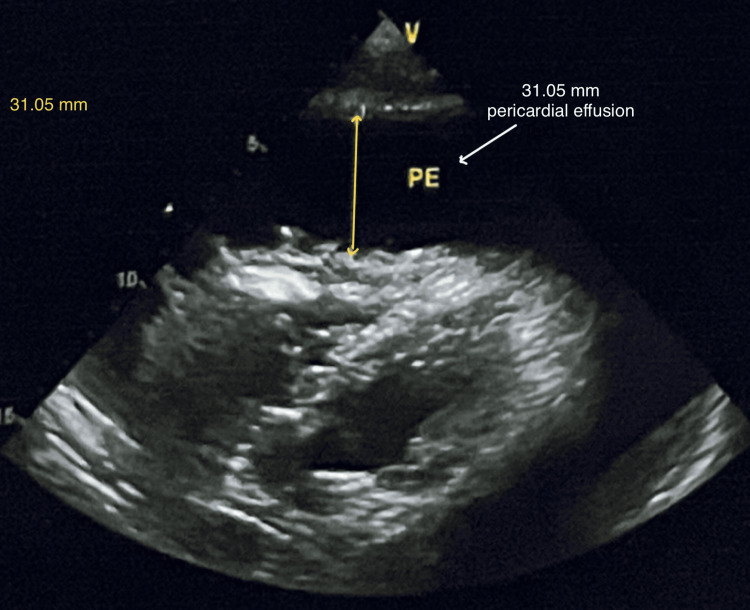 Figure 4
Figure 4 Figure 5
Figure 5| Pericardial fluid analysis | Value | Biological reference interval |
| Appearance | Haemorrhagic | Clear to pale yellow |
| Coagulum | Positive | Nil |
| Total protein (g/dL) | 3.7 | 1.7–4.6 |
| Glucose (mg/dL) | 72 | 80–134 |
| ADA | 96.1 U/L | <40 U/L |
| Total cell count (106 cells/L) | 90 | 35–2210 |
| Lymphocytes (106 cells/L) | 86 | 19–1634 |
| Neutrophils (106 cells/L) | 4 | 0–2 |
| Malignant cell | Not seen | Nil |
| CBNAAT for Mycobacterium TB | Positive | Nil |
| LFT | Before ATT | Day 11 of ATT | After 1 month of modified ATT | Reference intervals |
| S. T. bil | 0.3 | 0.8 | 0.6 | 0.2–1.2 mg% |
| S. D. bil | 0.1 | 0.2 | 0.2 | <0.2 mg% |
| S. T. prot | 5.9 | 6.3 | 6.6 | 6–8 g% |
| S. albumin | 3.4 | 2.4 | 3.5 | 3.5–5.5 g% |
| S. globulin | 2.5 | 3.9 | 3.1 | 1.8–3.6 g% |
| S. AST | 40 | 919 | 27 | <40 IU |
| S. ALT | 35 | 324 | 23 | <40 IU |
| S. ALP | 178 | 159 | 225 | 30–120 IU |
| S. GGT (female) | 61 | 83 | 211 | 7–32 IU |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Takotsubo Cardiomyopathy and Associated Phenomena · Pneumothorax, Barotrauma, Emphysema
Introduction
Tuberculosis (TB) is one of the most common causes of pericarditis in developing countries [1]. In developed countries, it is rare in immunocompetent and human immunodeficiency virus (HIV)-negative individuals [2]. Patients can present with non-specific signs and symptoms like fatigue, fever, weight loss, cough, shortness of breath, and chest pain [3]. It can often present with cardiac tamponade if early diagnosis and treatment are not initiated. Cardiac tamponade is an accumulation of fluid in the pericardial space, leading to compromised cardiac activity and shock, which is fatal [4]. The three principal features of tamponade are hypotension, soft or absent heart sound, and raised jugular venous pressure (JVP). The most common causes of tamponade are idiopathic pericarditis and pericarditis secondary to neoplastic diseases, TB, or bleeding into the pericardial space after leakage from an aortic dissection, cardiac operation, trauma, or treatment with anticoagulants [5]. In this case report, a patient presented with cardiac tamponade due to tubercular pericarditis, compounded by anti-tubercular treatment (ATT)-induced hepatitis.
Case presentation
A 55-year-old female presented to the emergency department with a two-week history of fatigue, shortness of breath, and chest pain for one week. It was not associated with nausea, vomiting, coughing, or palpitations. She had no history of fever, chills, or rigours, and no history of TB contact. There was no history of weight loss or night sweats. She did not have any co-morbidities and no history of drug use for any illness. On assessment, she had a temperature of 37 °C, a blood pressure of −80/60 mm Hg, a pulse rate of 130 bpm, a SpO_2_ of 96% in room air, and a respiratory rate of 18/min. Clinical examination revealed raised JVP and soft heart sounds. Electrocardiography (ECG) showed sinus tachycardia with a reduced QRS complex amplitude (Figure 1), cardiac enzyme hs Trop I was within the normal limit, and chest X-ray (CXR) showed an enlarged cardiac silhouette (Figure 2).
ECG showing sinus tachycardia with reduced QRS complex amplitude
CXR showing increased cardiothoracic ratio suggestive of cardiomegalyCXR: chest X-ray
Other routine investigations were within the normal limit. 2D echocardiography (2D Echo) showed a large pericardial effusion, compromising ventricular function, suggesting cardiac tamponade with no features of infective endocarditis (Figures 3-4).
2D Echo showing pericardial effusion distributed all around the heart
2D Echo showing massive pericardial effusion measured up to 31.05 mm
The patient was shifted to the intensive care unit (ICU), and emergency pericardiocentesis was done through a sub-xiphisternal approach under 2D Echo guidance. A 6F pigtail catheter was kept, bloody pericardial fluid of 1.4 L was drained, and a pericardial fluid analysis was sent (Figure 5).
Pericardiocentesis showing pericardial bloody fluid
Pericardial fluid analysis report showed adenosine deaminase (ADA) of 96.1 U/L (normal: <40 U/L), total cell count: 90 cells with 95% lymphocytes and 5% neutrophils, malignant cells: not seen, CBNAAT Mycobacterium TB positive with Rifampicin sensitivity indeterminate (Table 1).
The patient was started on ATT with broad-spectrum antibiotics and oral steroids, which included injection of piperacillin 4000 mg with tazobactam 500 mg intravenous thrice daily for seven days and oral prednisone 20 mg, one tablet once daily for seven days, respectively. We administered oral isoniazid (H) 300 mg, rifampicin (R) 450 mg, pyrazinamide (Z) 1500 mg, and ethambutol (E) 800 mg daily with pyridoxine supplementation. The patient developed severe nausea and vomiting by day 11 of treatment, and liver enzymes showed aspartate aminotransferase (AST) and alanine aminotransferase (ALT) more than three times the upper limit (AST>ALT). Jaundice was not visible clinically, and the prothrombin time-international normalized ratio (PT-INR) was high. In view of drug-induced hepatitis, ATT was therefore changed to modified ATT, i.e., injection streptomycin 750 mg, oral levofloxacin 750 mg, and ethambutol 800 mg per day. Hepatitis viral markers and HIV were negative. The patient was restarted with HRZE once the liver enzymes came down (Table 2 shows values of liver enzymes on different days of hospitalization). The pericardial drainage was carried out, yielding about 120-100 ml for the initial seven days and gradually decreasing to less than 10 ml per day, which was removed after three weeks. The blood, pleural fluid, and urine cultures were sterile. The USG abdomen showed normal findings; autoimmune, thyroid, and malignancy workups were negative. The patient improved clinically and symptomatically, got discharged, and was advised to follow up in the OPD.
Discussion
Mycobacterium TB presenting with pericardial disease complicated by cardiac tamponade is rare in developed countries, although it occurs more frequently in the context of immunosuppression [2]. In developing countries, it is still prevalent and can be life-threatening, even for immunocompetent patients [6]. Patients with tuberculous pericarditis are often associated with fever, fatigue, anorexia, weight loss, and night sweats, and on the extreme end of the spectrum, it can be associated with cardiac tamponade with a high mortality risk. It is most often caused by direct lymphatic spread or haematogenous seedlings. Risk factors include immunocompromised, elderly, and underlying co-morbid conditions. Our patient has no previous history of TB or TB contact, no underlying co-morbidities, and no history of trauma. In haemodynamically unstable patients, an emergency 2D-Echo should be done to rule out cardiac tamponade [7].
Diagnosis is made by pericardial fluid studies, including polymerase chain reaction (PCR), culture, and pericardial biopsy [8]. In our patient, pericardial fluid was bloody with high ADA activity (>40 U/L), and CBNAAT for Mycobacterium TB was positive. Management of tuberculous pericarditis consists of two months of Isoniazid, Rifampicin, Pyrazinamide, and Ethambutol, followed by four months of Isoniazid and Rifampicin (a total of six months of treatment) [9]. In our patient, oral Isoniazid 300 mg, Rifampicin 450 mg, Pyrazinamide 1500 mg, and Ethambutol 800 mg per day were given with pyridoxine supplementation and pericardial drainage.
Hepatotoxicity is one of the most common adverse drug reactions (ADR). Other ADRs include gastrointestinal and neurological disorders [10]. The incidence of drug-induced liver injury in India is said to be between 8% and 36% [11]. Our patient developed drug-induced hepatitis on day 11 of ATT and therefore changed to modified ATT: injection of streptomycin 750 mg, oral levofloxacin 750 mg, and ethambutol 800 mg. The patient was restarted with HRZE once liver enzymes were normalised. In this case, a patient with no co-morbidities came with tubercular pericardial effusion complicated by cardiac tamponade, requiring emergency pericardiocentesis and daily pericardial drainage. The patient was started on ATT, following which ATT-induced hepatitis developed, requiring supportive management, intensive care, and monitoring.
Conclusions
In patients presenting with pericardial effusion, tuberculosis has to be tested in developing countries like India, and if complicated with cardiac tamponade, emergency pericardiocentesis has to be done. Optimal management requires a combination of a drug-sensitive ATT regimen and pericardial drainage. Liver function tests along with other routine tests should be carried out before initiating ATT, and monitoring has to be done during the treatment as hepatotoxicity is one of the most common ADRs. Early diagnosis and treatment significantly improve the outcome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tuberculous pericarditis Circulation Mayosi BM Burgess LJ Doubell AF 3608361611220051633070310.1161/CIRCULATIONAHA.105.543066 · doi ↗ · pubmed ↗
- 2Incidence of specific etiology and role of methods for specific etiologic diagnosis of primary acute pericarditis Am J Cardiol Zayas R Anguita M Torres F 37838215199510.1016/s 0002-9149(99)80558-x 7856532 · doi ↗ · pubmed ↗
- 3Clinico-etiological profile of children with pericardial effusion in a tertiary care hospital in eastern India J Trop Pediatr Malgope R Basu S Sinha MK 11867202110.1093/tropej/fmaa 11833346812 · doi ↗ · pubmed ↗
- 4A case report of cardiac tamponade J Educ Teach Emerg Med Hunt DJ Mc Lendon K Wiggins M 06202110.21980/J 8J 644PMC 1033278437465716 · doi ↗ · pubmed ↗
- 5Harrisons Manual of Medicine, 19th Edition Kasper DL Fauci AS Hauser SL Longo DL Jameson JL Loscalzo J New York City Mc Graw Hill Professional 2016 https://archive.org/details/Dennis Kasper Anthony Fauci Stephen Hauser Dan Longo J.Jameson Joseph Loscalzo Harrisons Pri/page/n 2181/mode/2up
- 6A life-threatening pericardial tamponade revealing disseminated tuberculosis: a challenging medical care Heliyon Moussa C Rouis H Debbiche S Khattab A Khouaja I Zendah I Maȃlej S 09202310.1016/j.heliyon.2023.e 15174 PMC 1011420037089308 · doi ↗ · pubmed ↗
- 7Tuberculous pericarditis presenting as cardiac tamponade: role of Echocardiography J Med Cases Khatun N Akivis Y Ji B Chandrakumar HP Bukharovich I John S 2712761420233769236510.14740/jmc 4119 PMC 10482598 · doi ↗ · pubmed ↗
- 8Diagnostic test accuracy of Xpert MTB/RIF for tuberculous pericarditis: a systematic review and meta-analysis F 1000 Res Andrianto A Mertaniasih NM Gandi P Al-Farabi MJ Azmi Y Jonatan M Silahooij SI 761920203280232110.12688/f 1000 research.22770.1PMC 7417956 · doi ↗ · pubmed ↗