A Rare Case of Sphenoid Sinus Hemangioma With Intrasellar and Cavernous Sinus Extension
Mikiya Fujii, Kota Yokoyama, Yoji Tanaka, Daisuke Kobayashi, Ukihide Tateishi

TL;DR
This paper presents a rare case of a sphenoid sinus hemangioma that extended into critical brain areas, highlighting the challenges in diagnosing such tumors.
Contribution
The novelty lies in reporting a rare case with atypical features and emphasizing the importance of considering hemangiomas in differential diagnoses.
Findings
The patient's symptoms and imaging mimicked an aggressive tumor but were confirmed as a hemangioma via histopathology.
The case underscores the need for careful diagnosis to differentiate hemangiomas from more aggressive pathologies.
High vascularity and bone remodeling on imaging were key features in this case.
Abstract
Sphenoid sinus hemangiomas are uncommon and pose significant diagnostic challenges due to their rarity and the complex symptoms associated with their critical anatomical location. This report discusses a woman in her 40s who presented with worsening headaches, diplopia, and a sensation of pressure behind her eyes. Diagnostic imaging revealed a lobulated mass in the sphenoid sinus extending into the cavernous sinus and sella, initially mimicking an aggressive neoplastic pathology. However, histopathological examination following endovascular embolization and partial surgical resection confirmed the diagnosis of a cavernous hemangioma. This case highlights the importance of considering hemangiomas in the differential diagnosis of sphenoid sinus masses, especially when patients present with atypical symptoms and imaging shows features such as high vascularity and bone remodeling. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
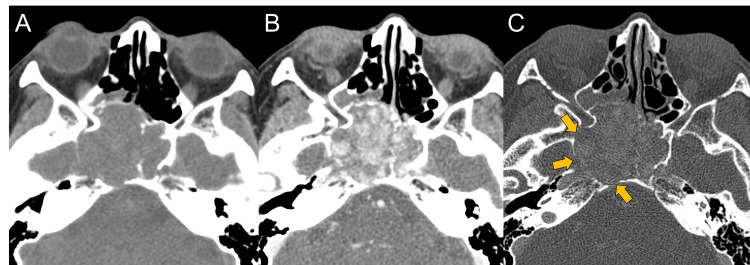 Figure 1
Figure 1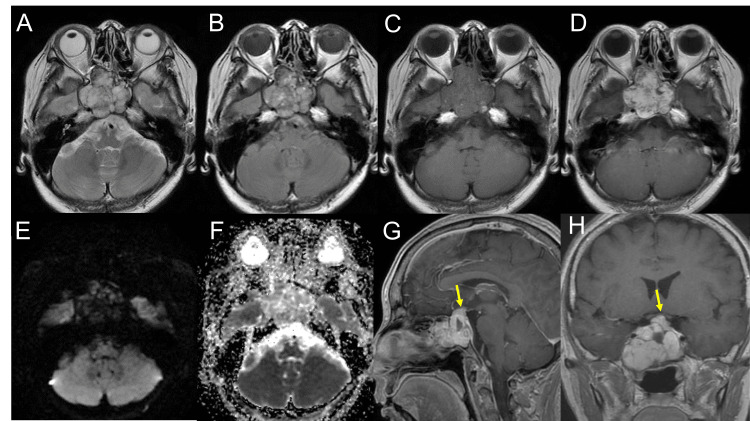 Figure 2
Figure 2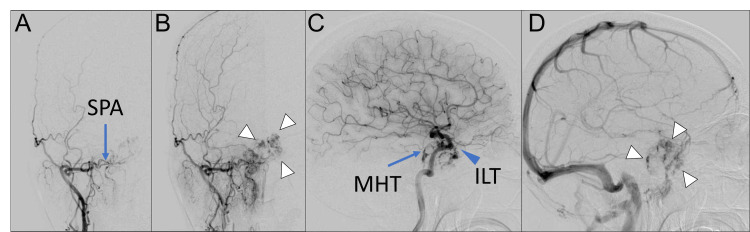 Figure 3
Figure 3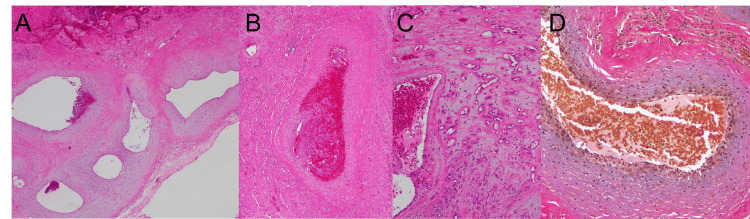 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Vascular Malformations and Hemangiomas · Head and Neck Surgical Oncology
Introduction
Hemangiomas of the head and neck, though benign, present unique diagnostic challenges due to their variable manifestations based on location [1-5]. As defined in the WHO's 5th Edition of Head and Neck Tumors, these vascular tumors show a preference for mucosal sites such as the oral cavity and the sinonasal tract [2]. The sphenoid sinus hemangioma, a particularly rare form, exemplifies these challenges due to its critical location and its potential to mimic more aggressive pathologies [6]. Key distinguishing features of hemangiomas include intense radiographic enhancement and the potential for bone remodeling, which are crucial for differentiating them from their malignant counterparts. Although the pathogenesis of hemangiomas is not fully understood, with recent genetic studies suggesting a potential origin from ectopic placental cells in congenital cases [7], this case report underscores the importance of understanding the morphological imaging characteristics of hemangiomas in rare locations. This is essential not only for accurate diagnosis but also for appropriate management to prevent overtreatment and ensure optimal patient outcomes. This report of a sphenoid sinus hemangioma extending into the intrasellar and cavernous sinuses emphasizes the need for meticulous evaluation in such complex cases.
Case presentation
A woman in her 40s presented to our hospital with a history of progressively worsening headaches, diplopia, and a sensation of pressure behind her eyes over the past five months. She also reported an increase in the frequency of epistaxis, which she had experienced occasionally since childhood. A physical examination showed restricted abduction in the right eye. Her medical history included only hyperlipidemia and allergic rhinitis, with no other significant past illnesses or conditions. Non-contrast computed tomography (CT) revealed a well-defined lobulated mass measuring 46×45×37 mm within the sphenoid sinus (Figure 1A), demonstrating expansile growth and bone remodeling (Figure 1C). Contrast-enhanced CT, although not a dynamic study, was taken in the arterial dominant phase and revealed enhancing vessel-like structures within the lesion (Figure 1B).
Non-contrast and contrast-enhanced computed tomography at the time of the visitOn a computed tomography (CT) scan, the mass shows expansive growth and iso-density on non-contrast CT (A). Contrast-enhanced CT in the arterial dominant phase revealed enhanced vessel-like structures within the lesion (B). There is remodeling rather than destruction of the surrounding bones (C, yellow arrows).
Magnetic resonance imaging displayed the mass as predominantly hyperintensity, with hypointense, thin internal septal structures on T2-weighted images (T2WI) (Figure 2A), heterogeneous signals on fluid-attenuated inversion recovery images (Figure 2B), and isointense structures on T1-weighted images (T1WI) (Figure 2C), with avid enhancement following contrast administration (Figure 2D). No diffusion restriction was noted (Figures 2E, 2F). The lesion primarily occupied the sphenoid sinus, extending into the cavernous sinus and the Sella, with noted compression of the optic chiasm (Figures 2G, 2H).
Preoperative magnetic resonance imaging On the magnetic resonance imaging (MRI) scan, the lesion shows predominantly hyperintensity with hypointense, thin internal septal structures on the T2-weighted image (A) and fluid-attenuated inversion recovery (B). The pre- (C) and post-contrast (D) T1-weighted image (T1WI) revealed the avid enhancement of the mass. The lesion did not show restrictions on the diffusion-weighted image (E) or apparent diffusion coefficient map (F). On sagittal (G) and coronal (H) post-contrast T1WI, the lesion was located mainly at the sphenoid sinus, involving the cavernous sinus and the sella. The optic chiasm was compressed by the lesion (G, H, yellow arrow).
Angiography revealed vascular pooling into the mass from branches of the external carotid artery, including the sphenopalatine artery, as well as branches of the internal carotid artery, such as the inferolateral trunk and meningohypophyseal trunk (Figure 3).
Preoperative angiography of the internal and external carotid arteriesAn anteroposterior view of the right external carotid angiography (A-B) revealed the vascular pooling of the mass (B, white arrowhead) supplied by the sphenopalatine artery (SPA) (A, blue arrow). On a lateral view of the internal carotid angiography (C-D), the vascular pooling of the mass (D, white arrowhead) supplied by the meningohypophyseal trunk (MHT) (C, blue arrow) and inferolateral trunk (ILT) (C, blue arrowhead) is revealed.
Preoperative multimodality imaging suggested a hypervascular mass in the sphenoid sinus. Despite the high signal intensity on T2WI, the presence of septal structures and low-signal components indicated a heterogeneous signal, suggesting the possibility of fibrous components. Although the patient’s age and gender were not typical for juvenile angiofibroma, they were considered in the differential diagnosis due to the imaging characteristics. A solitary fibrous tumor was also considered based on the T2WI heterogeneity, and paraganglioma was considered due to the hypervascular nature of the mass. Retrospectively, the imaging features were consistent with those reported for hemangiomas, but this was not included in the differential diagnosis preoperatively.
Perioperative endovascular coil embolization of the sphenopalatine artery and combined extended transbasal and endoscopic transnasal surgical approaches were performed, achieving a subtotal excision of the tumor.
Histopathological examination predominantly showed large vessels (Figure 4A) with partial luminal occlusion due to thrombosis (Figure 4B). Clusters of capillaries were also noted (Figure 4C). Internal elastic lamina in the vessel walls was absent (Figure 4D), and no tumor cells were observed, which led to a diagnosis of hemangioma.
Histopathology of the sphenoid sinus massHematoxylin and eosin staining (A-C) and Elastica van Gieson staining (D) of the sphenoid sinus hemangioma tissue specimen. Histopathological examination revealed that the lesion was predominantly composed of large vessels (A). Thrombosis (B) and several capillary vessels (C) are also depicted. No internal elastic lamina was observed on the vessel walls (D).
Postoperatively, the patient's symptoms improved, and she has been under follow-up with imaging. Nine years post-operation, there has been no recurrence of symptoms or lesions.
Discussion
This case presents a diagnostic challenge involving a sphenoid sinus mass that extended into the Sella and cavernous sinus, accompanied by significant bone remodeling. The imaging and clinical progression initially mimicked those of an aggressive neoplastic lesion. However, the final diagnosis was hemangioma, notable for the absence of tumor cells. Hemangiomas in the head and neck are defined as benign vascular neoplasms in the WHO classification [2], but they are categorized as a vascular malformation according to the latest International Society for the Study of Vascular Anomalies (ISSVA) classification published in 2018, due to the absence of atypical cells, and the term “-oma” is not preferred for non-neoplastic lesions [8,9]. Nevertheless, the mass lesions, so-called hemangioma, may be acceptable in imaging. The incidence rate of hemangiomas is approximately 1/2000-1/10000, with 40% occurring in the head and neck region [5,10]. Among hemangiomas in the head and neck region, 12.5% occur in the sinonasal area, with the most common sites being the nasal septum (40.5%) followed by the posterior nasal cavity (29.7%), while the involvement of the maxillary sinus is less frequent, reported at 8.1% [11]. Reports of sphenoid sinus hemangioma are extremely rare [6], as no sphenoid sinus involvement was documented in the largest study, which examined 37 sinonasal hemangiomas over 20 years at a single center [11]. The growth rate of hemangiomas is relatively slow, displaying an expansive growth pattern with well-circumscribed margins. Sphenoid sinus hemangiomas can present with central nervous system (CNS) symptoms such as headaches, visual impairment, diplopia, and olfactory disturbances, depending on the size and location of the lesion [1,6,12,13]. The present case showed similar CNS symptoms as well, consistent with the rare but documented progression of sphenoid sinus hemangiomas reported in the literature [6,11,12]. On imaging, hemangiomas typically demonstrate hypointense to isointense on T1WI, hyperintense on T2WI, and exhibit strong contrast enhancement, indicative of abundant vascular lumina. Although reports of imaging findings of sphenoid sinus hemangiomas are rare, they often appear slightly heterogeneous internally compared to the other locations, possibly due to bleeding effects [6,11]. Additionally, cases involving bone remodeling and progression into the cavernous sinus have been reported [6,14]. The differential diagnosis for sphenoid sinus hemangioma includes neoplasms such as chordoma, chondrosarcoma, and carcinoma, which commonly occur in this region, as well as juvenile angiofibroma, solitary fibrous tumor, paraganglioma, and metastases from hypervascular tumors such as clear cell renal cell carcinoma, hepatic cell carcinoma, and neuroendocrine tumors, which can also present as hypervascular masses in this location. Although there may be overlap in imaging and clinical findings, imaging features suggesting bone remodeling or high vascularity, as well as symptoms such as epistaxis, are considered helpful in the diagnosis of sphenoid sinus hemangioma. Pathologically, hemangiomas are primarily classified into capillary and cavernous types based on the dominant vessel size [1], and the present case showed the predominance of large artery-like vessels over capillary regions, which supports the diagnosis of a cavernous hemangioma rather than a capillary hemangioma. A broader categorization, such as "hemangioma," may be appropriate.
Treatment for sphenoid sinus hemangioma often requires surgical intervention, particularly when symptomatic. Previous reports have predominantly reported undergoing endoscopic endonasal surgery [1,6,12,13,15]. Recurrence after excision is uncommon, and the prognosis is generally favorable. However, vascular malformations involving the cavernous sinus carry a risk of bleeding, and biopsy or surgery can lead to massive hemorrhage, potentially resulting in fatal outcomes [16]. When hypervascularity is identified on imaging, it is necessary to exercise caution during invasive procedures. Preoperative embolization should be considered to minimize intraoperative bleeding and facilitate a safer surgical intervention [15].
Conclusions
This case underscores the diagnostic complexities associated with sphenoid sinus hemangiomas, particularly when they mimic more aggressive neoplastic processes. The diagnosis was challenging due to the hemangioma's rare location and its similar presentation to malignant tumors on imaging. However, careful evaluation, including clinical, radiological, and histopathological examination, was crucial in differentiating it from other serious conditions. This case highlights the need for clinicians to consider hemangiomas in the differential diagnosis when encountering expansile lesions of the sphenoid sinus with significant bone remodeling and high vascularity, even when initial symptoms and imaging may suggest malignancy.
The management of sphenoid sinus hemangiomas involves tailored therapeutic strategies to prevent significant morbidity. This case not only adds to the existing literature by documenting a rare occurrence of sphenoid sinus hemangioma but also emphasizes the importance of a thorough diagnostic approach that integrates clinical, radiological, and pathological data to ensure accurate diagnosis and appropriate management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intracranial capillary hemangioma: extra-axial tumorous lesions closely mimicking meningioma J Neurooncol Phi JH Kim SK Cho A Kim DG Paek SH Park SH Wang KC 17718510920122254465210.1007/s 11060-012-0884-6 · doi ↗ · pubmed ↗
- 2WHO Classification of Tumours Haemangioma. Head and Neck Tumours Thompson LDR Bullerdiek J Flucke U Lyon (France)International Agency for Research on Cancer 202320241159 https://tumourclassification.iarc.who.int/chapters/52.2.
- 3Role of imaging in the diagnosis of parotid infantile hemangiomas Int J Pediatr Otorhinolaryngol Weber FC Greene AK Adams DM Liang MG Alomari MH Voss SD Chaudry G 616610220172910687710.1016/j.ijporl.2017.08.035 · doi ↗ · pubmed ↗
- 4Non-epithelial tumors of the nasal cavity, paranasal sinuses, and nasopharynx: A clinicopathologic study. I. General features and vascular tumors Cancer Fu YS Perzin KH 5127533197410.1002/1097-0142(197405)33:5<1275::aid-cncr 2820330513>3.0.co;2-44362952 · doi ↗ · pubmed ↗
- 5Understanding venous malformations of the head and neck: a comprehensive insight Med Oncol Colletti G Ierardi AM 423420172818120710.1007/s 12032-017-0896-3 · doi ↗ · pubmed ↗
- 6Capillary hemangioma of the sphenoid sinus with intrasellar and parasellar extensions Radiol Case Rep Pas M Shimono T Morisako H 1561601720223482004110.1016/j.radcr.2021.10.011PMC 8599932 · doi ↗ · pubmed ↗
- 7Endothelial and circulating C 19MC micro RN As are biomarkers of infantile hemangioma JCI Insight Strub GM Kirsh AL Whipple ME 01201610.1172/jci.insight.88856 PMC 502941927660822 · doi ↗ · pubmed ↗
- 8ISSVA: Classification for vascular anomalies 5 2024 2018 https://www.issva.org/classification