Frequency of Common and Uncommon BRAF Alterations among Colorectal and Non-Colorectal Gastrointestinal Malignancies
Amit Mahipal, Michael H. Storandt, Emily A. Teslow, Ellen Jaeger, Melissa C. Stoppler, Zhaohui Jin, Sakti Chakrabarti

TL;DR
This study shows that BRAF gene changes are more common in certain non-colorectal GI cancers, like bile duct and small intestine cancers, and suggests they could be important for treatment.
Contribution
The study reveals a distinct BRAF alteration profile in non-colorectal GI cancers, highlighting the higher frequency of BRAF fusions and amplifications compared to colorectal cancer.
Findings
BRAF alterations are most common in bile duct and small intestinal cancers among non-CRC GI malignancies.
BRAF fusions and amplifications are more frequent in non-CRC GI cancers than in CRC.
Non-CRC GI cancers show a higher prevalence of class II and III BRAF alterations compared to CRC.
Abstract
The combination of dabrafenib plus trametinib received tumor-agnostic approval for patients with BRAF V600E mutations. BRAF alterations are well characterized in patients with colorectal cancer (CRC) but their role in other gastrointestinal (GI) cancers is not known. This study demonstrates that amongst non-CRC GI cancers, BRAF alterations are most commonly present in bile duct cancers and small intestinal cancers. BRAF amplifications and BRAF fusions are more commonly observed in non-CRC GI cancers than in CRC and can potentially be an attractive therapeutic target. The prognostic impact of BRAF alterations in non-CRC GI cancers needs to be further investigated. Background: The predictive and prognostic role of BRAF alterations has been evaluated in colorectal cancer (CRC); however, BRAF alterations have not been fully characterized in non-CRC gastrointestinal (GI) malignancies. In…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
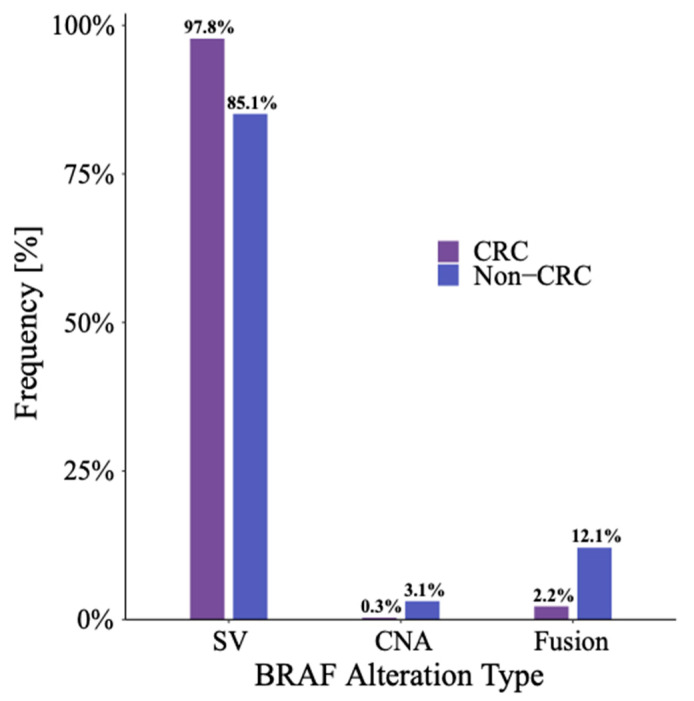 Figure 1
Figure 1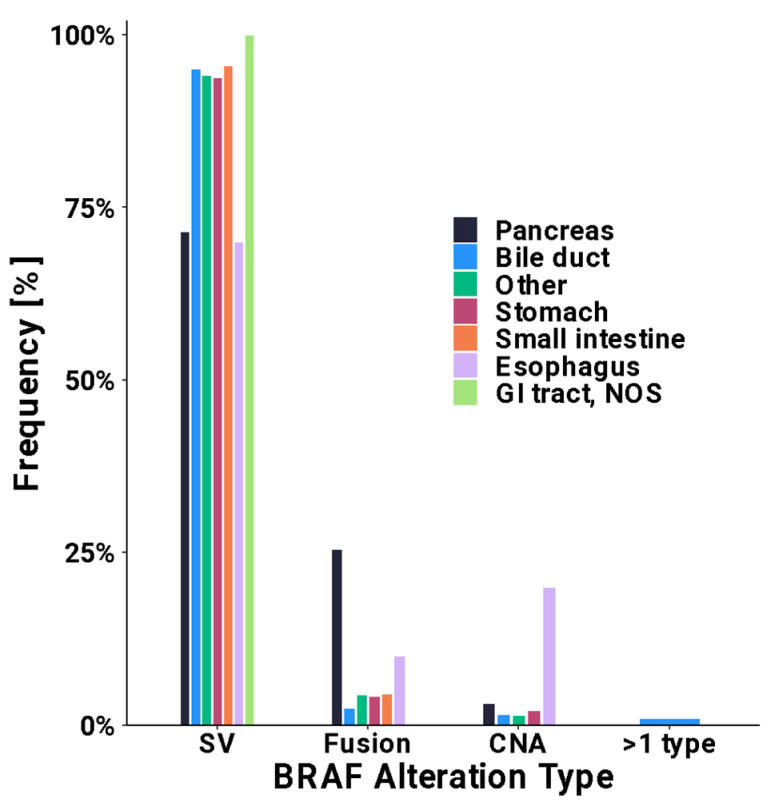 Figure 2
Figure 2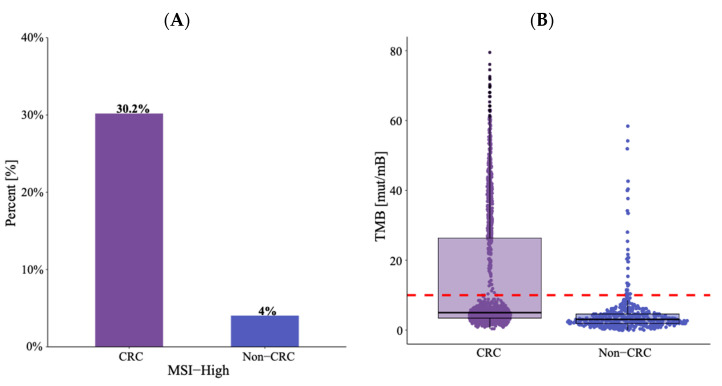 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsColorectal Cancer Treatments and Studies · Genetic factors in colorectal cancer · Cancer Genomics and Diagnostics
1. Introduction
The B-raf proto-oncogene (BRAF) encodes BRAF protein, which normally functions via the mitogen-activated protein kinase/extracellular signal-related kinase (MAPK/ERK) pathway downstream of growth-factor receptors to regulate cell growth and proliferation [1]. Activating BRAF alterations may result in constitutive activation of this pathway, and are implicated in oncogenesis, leading to an increase in tumor growth and metastasis [2]. Different classes of BRAF alterations have been identified, each with distinct clinical relevance. Class I mutations, the most common, include BRAF V600E alterations, which lead to the activation of BRAF monomers in a kinase-independent manner. Class II mutations result in the formation of activated BRAF dimers, also in an RAS-independent manner. Lastly, class III mutations result in kinase-inactivating heterodimers in an RAS-dependent manner [3,4,5,6].
Among gastrointestinal (GI) malignancies, BRAF mutations have been extensively studied in colorectal cancer (CRC), detected in about 8–12% of patients with metastatic disease [7]. BRAF mutations may be classified as class I (V600E), class II, and class III, with each class having a distinct mechanism and clinical phenotype. Class I mutations result in constitutive activation of BRAF monomers in an RAS-independent manner, class II mutations result in constitutively activate BRAF dimers in an RAS-independent manner, and class III mutations more avidly bind RAS and CRAF. The most common alteration, BRAF V600E, has been associated with right-sided primaries, and poorer survival [6]. Class II BRAF mutations have also been associated with a poorer prognosis, comparable to patients with class I mutations, while those with class III mutations have been found to have a higher frequency of left-sided disease, with a lower probability of nodal metastases [5].
BRAF alterations have been less commonly reported in non-CRC GI malignancies, and little is known regarding the frequency and spectrum of these mutations. With the continued development of targeted therapies, it is essential to recognize the incidence of BRAF mutation types, as class I and II alterations may be a valid target in a subset of patients. Recently, dabrafenib, a BRAF inhibitor, in combination with trametinib, an MEK inhibitor, received tumor-agnostic approval for advanced solid malignancies harboring BRAF V600E [8]. This further highlights the importance of recognizing the frequency of BRAF alteration among non-CRC GI malignancies, as well as the class of BRAF alteration.
In the present study, we utilized data to determine the frequency of BRAF mutations among non-CRC GI malignancies and the spectrum of these mutations, and determined if there are differences in the prevalence of these alterations in certain patient populations.
2. Methods
2.1. Cohort Selection
Patients with a primary diagnosis of a GI malignancy were identified from the Tempus database and filtered to those who received Tempus xT or xF testing prior to September 2023. GI malignancies were defined as primary tumor sites outlined in Table 1. Patients were considered to have CRC if their primary cancer site was in the colon, rectum, or rectosigmoid junction. The concept of a primary cancer for this study is defined as the cancer diagnosis for which the patient underwent sequencing. Patients were further filtered into those who had a gain-of-function (GOF) BRAF alteration detected on either assay. For patients with multiple sequencing reports, the most recent report on which a BRAF alteration was detected was chosen for analysis. GOF BRAF alterations were defined as a pathogenic/likely pathogenic somatic short variant, copy number amplification ≥8, or fusion (RNA or DNA).
2.2. Sequencing Assays
Next-generation sequencing was conducted using the Tempus xT and xF assays (Tempus AI, Chicago, IL, USA), as previously described [9,10,11,12,13,14]. Briefly, Tempus xT is a targeted, tumor/normal-matched DNA panel that detects single-nucleotide variants (SNVs), insertions and/or deletions (indels), and copy number variants (CNVs) in 648 genes, as well as chromosomal rearrangements in 22 genes with high sensitivity and specificity. Tempus xF is a targeted liquid biopsy DNA panel that identifies SNVs and indels in 105 genes, CNVs in 6 genes, and chromosomal rearrangements in 7 genes.
2.3. Tumor Mutation Burden
Tumor mutation burden (TMB) was calculated as previously reported [12]. Briefly, TMB was calculated by dividing the number of nonsynonymous variations by the size of the panel. All nonsilent somatic coding variations such as missense, indel, and stop-loss variants with coverage greater than ×100 and an allelic fraction greater than 5% are included in the count of nonsynonymous variations. Tumors were considered to have high TMB (TMB-H) if they had an adjusted TMB score of 10 mutations per megabase (mut/Mb) or more in tissue testing, or 15 mut/Mb or more in liquid testing.
2.4. Microsatellite Instability
The Tempus xT panel included probes for 239 microsatellites that are frequently unstable in tumors with mismatch repair (MMR) deficiencies. The microsatellite instability (MSI) classification algorithm used reads mapping to these frequently unstable regions to classify tumors into three categories: microsatellite instability-high (MSI-H), microsatellite stable (MSS), or microsatellite equivocal (MSE). This assay can be performed with paired tumor–normal samples or tumor-only samples. Both algorithms return the probability of the patient being MSI-H, which is then translated into an MSI status of MSI-H, MSS, or MSE. All loci with sufficient coverage were tested for instability, as measured by changes in the distribution of the number of repeat units in the tumor reads as compared to the normal reads using the Kolmogorov–Smirnov test. If p ≤ 0.05, the locus was considered unstable. The proportion of unstable loci was fed into a logistic regression classifier trained on tumor samples with clinically determined MSI statuses. The Tempus xF panel included probes for 227 microsatellites that are frequently unstable in tumors with MMR deficiencies. To detect MSI, the relative frequency and distribution are determined for any read containing repetitive sequences. To predict the probability of an unstable locus, a k-nearest neighbors model (with k = 100) is used along with normalized percent lower, mean lower, and mean log-likelihood metrics. The percentage of unstable loci is calculated from the probabilities of each sample, with >50% unstable loci considered MSI-high [10,11,13].
2.5. Statistical Analysis
Demographic and clinical characteristics are described as percentages or median with range and interquartile range and compared by chi-squared/Fisher’s exact tests or Wilcoxon rank sum tests, as applicable. The prevalence of MSI and TMB-H are described as percentages and compared using chi-squared tests. BRAF alteration types, class types, amino acid effects, and prevalence of co-mutations are described and compared similarly, with a false discovery rate correction for multiple testing. Analyses are two-sided with statistical significance evaluated at the 0.05 alpha level.
3. Results
3.1. Cohort Characteristics
Among 51,560 sequenced patients with a history of a GI malignancy, 40% were diagnosed with CRC (n = 20,656) and 60% were diagnosed with a non-CRC GI malignancy (n = 30,904). Among the BRAF-altered cohort, 73% underwent a tissue-based assay and 27% underwent a liquid-based (blood) assay. The most common non-CRC GI malignancies included cancers of the pancreas (14,300; 28%), bile duct (4923; 9.5%), esophagus (3.316; 6.4%), and stomach (3029; 5.9%). In our cohort, 17% of the patients had another prior malignancy (n = 432) with the most common being breast cancer (3.2%), prostate cancer (2.1%), hematologic malignancy (1.9%), and skin cancer (0.8%). The rates of multiple primary cancers were similar in the two groups.
BRAF GOF-altered patients diagnosed with CRC were compared to non-CRC GI malignancies. CRC patients were slightly older than those with non-CRC GI malignancies (median age of 67 vs. 66 years; p = 0.029). BRAF-altered CRC was more commonly found in females (57% vs. 45% female; p < 0.001) while BRAF-altered non-CRC GI malignancies were more often observed in males. Among BRAF-altered CRC patients, 85% were white, whereas only 77% of those with a BRAF-altered non-CRC GI malignancy were white. Notably, significant differences were observed across races between CRC and non-CRC GI malignancies (p < 0.001), with 11% of those with a non-CRC GI malignancy being black or African American, versus only 6.4% of those with BRAF-altered CRC. Sixty-nine percent with CRC had metastases prior to testing, while fifty-nine percent with a non-CRC GI malignancy had metastases prior to testing (p < 0.001). Characteristics of the BRAF-altered patients based on primary tumor location are described in Table 1.
3.2. Incidence of BRAF Gain-of-Function Alteration by Primary Tumor Location
BRAF GOF alterations were more frequently seen in patients with CRC, with higher prevalence compared to non-CRC GI malignancies overall (8.9% vs. 2.2%, p < 0.001). Non-CRC GI malignancies with the highest incidence of BRAF GOF alterations included bile duct cancers (4.1%) and small intestine cancers (4.0%). The frequency of BRAF GOF alteration by primary tumor location is described in Table 2 and Supplemental Table S1.
3.3. Characterization of BRAF Gain-of-Function Alterations
Among all patients with a BRAF GOF alteration, 94% were the result of a short variant (SV). SVs were more common among patients with CRC (98%) compared to patients with a non-CRC GI malignancy (85%) (p < 0.001). The most common SV mutations were in exon 15 and exon 11 with rates of 90% and 6.4%, respectively, in patients with CRC. The corresponding rates for patients with non-CRC GI cancers were 58% and 15%, respectively. Among patients with a BRAF-altered non-CRC GI malignancy, the prevalence of copy number amplification (3.1% vs. 0.3%, p < 0.001) and fusions (12% vs. 2.2%, p < 0.001) were higher when compared to those with CRC (Figure 1, Supplemental Table S2). Interestingly, there was also a small subset of patients with >1 BRAF alteration (SV, CNA, and/or fusion) detected, including four patients who harbored both a pathogenic BRAF fusion in addition to a V600E alteration. Figure 2 characterizes the type of BRAF alteration based on the primary location for non-CRC GI malignancies. Supplemental Table S3 provides a full list of fusions detected.
When evaluating alteration class amongst BRAF GOF cancers, class I mutations were more common in BRAF-altered CRC compared to non-CRC GI malignancies (75% vs. 28%, p < 0.001). However, class II (28% vs. 6.8%, p < 0.001) and class III (23% vs. 14%, p < 0.001) were more commonly seen in BRAF-altered non-CRC GI malignancies compared to BRAF-altered CRC. Specific BRAF mutations with a prevalence of ≥1% are reported in Table 3.
3.4. MSI and TMB among BRAF-Altered Tumors
We then characterized TMB and MSI status in BRAF-altered malignancies. TMB-H was more frequently detected in those with BRAF-altered CRC compared to those with BRAF-altered non-CRC GI malignancies (31% vs. 6.8%, p < 0.001). Similarly, MSI-H was more frequently detected in BRAF-altered CRC versus non-CRC GI malignancies (30% vs. 4%, p < 0.001) (Figure 3, Supplemental Table S4). Mismatch repair protein (MMR) status by immunohistochemistry was available for a subset of patients (n = 730). MMR deficiency was also noted more commonly in patients with CRC compared to non-CRC GI cancers (36% vs. 6.3%, p < 0.001). In patients with MSI-stable tumors, rates of TMB-high were similar in CRC and non-CRC GI cancers (2.1% vs. 2.7%, p = 0.5).
3.5. Co-Mutations in BRAF-Altered Tumors
As part of an exploratory analysis, the co-mutational landscape of BRAF-altered cancers was evaluated (Supplemental Table S5). Commonly occurring co-mutations seen in BRAF-altered CRC were TP53 (70%), APC (42%), RNF43 (30%), SMAD4 (22%), PIK3CA (21%), KMT2D (detected in tissue only), and MSH3 (18%). The most common co-mutations observed in non-CRC GI malignancies were TP53 (52%), CDKN2A (32%), CDKN2B (20%, detected in tissue only), ARID1A, SMAD4, KRAS (17%), and MTAP (16%, detected in tissue only).
We specifically looked at the association of BRAF and RAS alteration. Of 2516 patients with a BRAF alteration, 379 (15%) patients had a co-alteration in an RAS gene. Interestingly, amongst 27 patients with BRAF amplification, 37% of the patients had an alteration in an RAS gene.
3.6. Characterization of Patients Treated with a BRAF Inhibitor
Last, we sought to characterize patients who had received a BRAF inhibitor. However, only 52 (2.8%) patients with BRAF-altered CRC and 11 (1.6%) patients with a BRAF-altered non-CRC GI malignancy had received a BRAF inhibitor, limiting further analysis. The most commonly used BRAF inhibitor among patients with BRAF-altered CRC was encorafenib in 85%, whereas the most common BRAF inhibitor in those with a BRAF-altered non-CRC GI malignancy was dabrafenib in 91%.
4. Discussion
In the present study, we described the frequency and spectrum of BRAF alterations in non-CRC GI malignancies by using a large database of patients who underwent tumor somatic profiling and compared it to the frequency of BRAF alteration in CRC. This has not been widely reported previously. BRAF alterations were present in 8.9% of CRC patients, yet less frequently detected in patients with a non-CRC GI malignancy (2.2%). In addition, non-CRC GI malignancies more frequently harbored uncommon class II and III BRAF alterations, including non-V600E SVs, fusions, and CNAs.
Our data illustrates that there is a unique profile of BRAF alterations in the non-CRC GI malignancy population. Among patients with CRC, V600E accounted for 75% of BRAF alterations, which is consistent with prior reports [5,15]. Conversely, V600E only accounted for 27% of BRAF mutations among non-CRC GI malignancies, and class II and class III alterations accounted for 28% and 23%, respectively. Of note, a previous pan-cancer analysis of 115,000 patients found that non-V600E BRAF mutations accounted for 35% of BRAF mutations, which is lower than the rates of class II and III mutations reported in this study [16]. The difference in frequency of non-V600E BRAF mutation between CRC and non-CRC GI malignancies is important to consider, recognizing variation in tumor behavior by class of BRAF mutation. In the case of CRC, class II BRAF mutations have shown similar clinical outcomes when compared to V600E*,* while class III BRAF mutations have been associated with relatively better prognosis [5]. How these different classes of mutation may impact outcomes in non-CRC GI malignancies is not well established at this time and merits further evaluation. A previous study evaluating clinical outcomes in patients with BRAF-mutated intrahepatic cholangiocarcinoma reported that V600E was associated with larger, more invasive tumors and poorer overall survival when compared to non-V600E mutations. However, the breakdown of these mutations with regard to different classes was not reported [17]. Prognostic implications of non-V600E mutation also merit further evaluation across non-CRC GI malignancies.
When looking at non-CRC GI malignancies, biliary tract cancers were found to have the highest frequency of BRAF alteration in 4.1% of patients, which is comparable to prior studies reporting a frequency of 5–7% [18]. BRAF V600E is a targetable mutation in biliary tract cancers, based on the results of the phase 2 basket trial, ROAR [19]. However, it is again important to note the high frequency of non-V600E mutations among non-CRC GI malignancies. In the case of small bowel cancer, which was the second most common non-CRC GI malignancy to have a BRAF mutation in this study, an incidence of 4.0% was detected, which is lower than a prior report suggesting a frequency of approximately 9% [20]. Studies have also shown that the majority of BRAF mutations in small bowel adenocarcinoma are non-V600E, which is consistent with our current report [21,22]. Overall, these two examples demonstrate an unmet need for targeting non-V600E BRAF alteration in non-CRC GI malignancies. There is some evidence that MEK inhibition may have activity in targeting non-V600E BRAF mutations [23,24,25]. However, an additional basket study including patients with solid tumors and lymphoma harboring a non-V600E BRAF mutation or BRAF fusion did not show promising activity [26]. Additionally, there is some thought that class III BRAF-mutated CRC may have elevated sensitivity to EGFR inhibition, which may be applicable to non-CRC GI malignancies as well [27,28].
Another finding of interest in this study was higher rates of BRAF fusions in patients with BRAF-altered non-CRC GI malignancies compared to CRC (12% vs. 2.2%, p < 0.001). BRAF fusions result in the substitution of the N-terminus region of BRAF, which is its inhibitor domain, with another binding partner, which may result in constitutive activation of the BRAF gene [29,30]. A prior study, including 2154 patients with CRC who completed comprehensive genomic profiling found BRAF fusion in 4 patients with CRC (0.3%) [31]. Concerning non-CRC GI malignancies, fusions were most frequently detected in pancreatic cancer, with an incidence of 0.3% in the aforementioned study [31]. In the current study, with regards to non-CRC GI tumors, we also found that fusions were more frequent in pancreatic as well as esophageal tumors, accounting for 25% and 10% of BRAF alterations occurring in those tumor types, respectively. While rare, solid malignancies with BRAF fusion may be targeted by MEK inhibitors, based on a study evaluating trametinib in melanoma with non-V600E BRAF mutation or BRAF fusion, although additional study in other solid malignancies is needed [23].
In addition, we found that BRAF-altered CRC had a significantly higher frequency of MSI-H and TMB-H when compared to BRAF-altered non-CRC GI malignancies. The association between BRAF mutation and MSI-H in CRC is well established. The reason for the decreased frequency of MSI-H among patients with BRAF-mutated non-CRC GI malignancies is not certain, but prior work has demonstrated that non-V600E BRAF-mutated CRC exhibits lower rates of MSI-H [32]. Recognizing that non-CRC GI malignancies have higher rates of non-V600E BRAF mutation, this is a very plausible explanation for this difference in frequency.
Limitations of this study include a lack of diversity among the sample population ordered at a large diagnostic testing laboratory, which was predominantly white, limiting generalizability to other racial groups to some extent. Additionally, data regarding BRAF inhibitor treatment and clinical outcomes has yet to be evaluated. In this study, only a small population of patients had a history of receiving BRAF inhibitors prior to sample collection (n = 63); thus, this remains an important area for future research in exploring outcomes of patients with various BRAF alterations across tumor subtypes to determine if BRAF inhibitors can alter the natural history of the disease. Importantly, it will be important to assess the impact of BRAF inhibitors in BRAF non-V600E mutated non-CRC GI cancers, especially those with BRAF fusions.
5. Conclusions
In this study, we report a higher frequency of non-V600E (class II and III) BRAF alterations in non-CRC GI malignancies compared to CRC. Prior work has shown that these mutations result in distinct phenotypes and may have prognostic implications for the patient. Future work should aim to better define the prognostic implications of these mutations, as well as the efficacy of targeted therapies to treat this subpopulation of cancer patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Śmiech M. Leszczyński P. Kono H. Wardell C. Taniguchi H. Emerging BRAF Mutations in Cancer Progression and Their Possible Effects on Transcriptional Networks Genes 202011134210.3390/GENES 1111134233198372 PMC 7697059 · doi ↗ · pubmed ↗
- 2Dibb N.J. Dilworth S.M. Mol C.D. Switching on kinases: Oncogenic activation of BRAF and the PDGFR family Nat. Rev. Cancer 2004471872710.1038/NRC 143415343278 · doi ↗ · pubmed ↗
- 3Lin Q. Zhang H. Ding H. Qian J. Lizaso A. Lin J. Han-Zhang H. Xiang J. Li Y. Zhu H. The association between BRAF mutation class and clinical features in BRAF-mutant Chinese non-small cell lung cancer patients J. Transl. Med.20191729810.1186/S 12967-019-2036-731470866 PMC 6716889 · doi ↗ · pubmed ↗
- 4Wan P.T.C. Garnett M.J. Roe S.M. Lee S. Niculescu-Duvaz D. Good V.M. Project C.G. Jones C.M. Marshall C.J. Springer C.J. Mechanism of activation of the RAF-ERK signaling pathway by oncogenic mutations of B-RAF Cell 200411685586710.1016/S 0092-8674(04)00215-615035987 · doi ↗ · pubmed ↗
- 5Schirripa M. Biason P. Lonardi S. Pella N. Simona Pino M. Urbano F. Antoniotti C. Cremolini C. Corallo S. Pietrantonio F. Class 1, 2, and 3 BRAF-Mutated Metastatic Colorectal Cancer: A Detailed Clinical, Pathologic, and Molecular Characterization Clin. Cancer Res.2019253954396110.1158/1078-0432.CCR-19-031130967421 · doi ↗ · pubmed ↗
- 6Ciombor K.K. Strickler J.H. Bekaii-Saab T.S. Yaeger R. BRAF-Mutated Advanced Colorectal Cancer: A Rapidly Changing Therapeutic Landscape J. Clin. Oncol.2022402706271510.1200/JCO.21.0254135649231 PMC 9390817 · doi ↗ · pubmed ↗
- 7Sanz-Garcia E. Argiles G. Elez E. Tabernero J. BRAF mutant colorectal cancer: Prognosis, treatment, and new perspectives Ann. Oncol. Off. J. Eur. Soc. Med. Oncol.2017282648265710.1093/ANNONC/MDX 40129045527 · doi ↗ · pubmed ↗
- 8Subbiah V. Kreitman R.J. Wainberg Z.A. Gazzah A. Lassen U. Stein A. Wen P.Y. Dietrich S. de Jonge M.J.A. Blay J.Y. Dabrafenib plus trametinib in BRAFV 600E-mutated rare cancers: The phase 2 ROAR trial Nat. Med.2023291103111210.1038/S 41591-023-02321-837059834 PMC 10202803 · doi ↗ · pubmed ↗