Early physical rehabilitation dosage in the IntensiveCare Unit predicts hospital outcomes after criticalCOVID-19
Kirby P. Mayer, Evan Haezebrouck, Lori M. Ginoza, Clarisa Martinez, Minnie Jan, Lori A. Michener, Lindsey Fresenko, Ashley A. Montgomery-Yates, Anna G. Kalema, Amy M. Pastva, Michelle Biehl, Matthew F. Mart, Joshua K. Johnson

TL;DR
Early physical rehabilitation in the ICU improves hospital outcomes for critical COVID-19 patients.
Contribution
A novel method to quantify rehabilitation dosage is introduced and linked to patient outcomes.
Findings
Rehabilitation dosage is moderately and positively associated with physical function at discharge.
Mechanical ventilation and early mobility scores predict physical function at discharge.
Higher rehabilitation exposure in the ICU correlates with better post-hospital physical outcomes.
Abstract
to examine the relationship between physical rehabilitation parameters including a novel approach to quantifying dosage with hospital outcomes for patients with critical COVID-19. Retrospective practice analysis from March 5, 2020, to April 15, 2021. Intensive care units (ICU) at four medical institutions n = 3,780 adults with ICU admission and diagnosis of COVID-19 We measured the physical rehabilitation treatment delivered in ICU and patient outcomes: 1) mortality; 2) discharge disposition; and 3) physical function at hospital discharge measured by the Activity Measure-Post Acute Care (AM-PAC) “6-Clicks” (6–24, 24=greater functional independence). Physical rehabilitation dosage was defined as the average mobility level scores in the first three sessions (a surrogate measure of intensity) multiplied by the rehabilitation frequency (PT + OT frequency in hospital). The cohort was a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
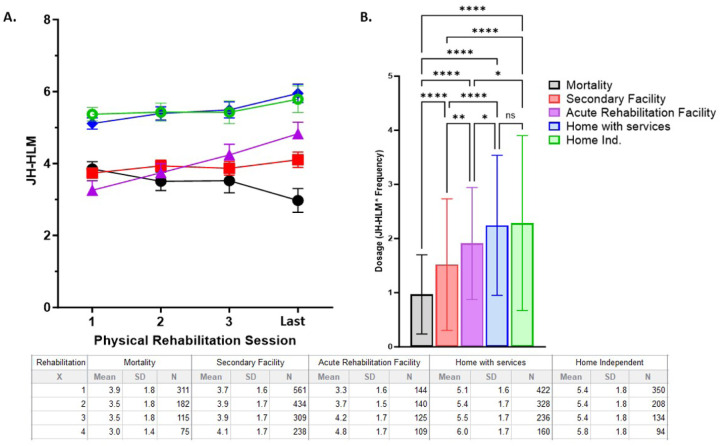 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Long-Term Effects of COVID-19 · Frailty in Older Adults
Objectives
Exercise and early mobility are key components of clinical practice guidelines for patients with critical illness, as defined in the Intensive Care Unit (ICU) Liberation bundle.^1^ However, findings from multiple randomized ICU rehabilitation trials have been equivocal, demonstrating minimal impact on mortality and physical function.^2–4^ A potential explanation for the lack of benefits is a non-specific exercise dose. Patients are routinely randomized to “one-size-fits-all” protocols leading to heterogeneity in the response to treatment. Dosage that accounts for the frequency and intensity of exercise is frequently overlooked or not addressed in critical care practice and research. The rehabilitation dosage delivered in large randomized controlled trials (RCTs) is rarely implemented in clinical practice^5,6^, and patients in the ICU seldomly receive a targeted or individualized dose of exercise. Patients with critical COVID-19 have not been studied to determine if dosage of exercise is related to outcomes. The COVID-19 pandemic may have unintentionally altered patterns in rehabilitation practice due to periods of isolation.^7^ Thus, the primary objective of this study was to examine the relationship between physical rehabilitation parameters including a novel approach to quantifying dosage with hospital outcomes for patients with critical COVID-19.
Design
Retrospective practice analysis for patients hospitalized from March 5, 2020, to April 15, 2021.
Setting
ICUs at four academic medical institutions (University of Kentucky, Cleveland Clinic, University of Michigan, and University of Southern California)
Patients
3,780 adults (≥ 18 years of age) admitted to ICU with primary diagnosis of COVID-19
Interventions
We examined the relationship between ICU-based physical rehabilitation interventions and hospital-based outcomes. Outcomes included: 1) mortality; 2) discharge disposition; and 3) physical function at or near hospital discharge measured by the Activity Measure-Post Acute Care (AM-PAC) “6-Clicks” Inpatient Mobility Short Form (6–24, 24=greater functional independence).^8^ Physical rehabilitation parameters included time to first rehabilitation (physical [PT] or occupational [OT]) session in days, number of PT and OT sessions completed during hospital length of stay (LOS), frequency of PT and OT (# of session / hospital LOS), mobility status during first three and the last recorded (if more than 3 sessions) rehabilitation sessions. Mobility levels were quantified by the John Hopkins-Highest Level of Mobility (JH-HLM, 1–8, 1=lying in bed; 8=ambulating >250 feet). The physical rehabilitation dose was quantified in a novel method: the average JH-HLM score over the first three sessions (a surrogate measure of early intensity) was multiplied by rehabilitation frequency (PT + OT frequency). The novel dose provides information on delivery of ICU rehabilitation such that patients who achieve high mobility with daily frequency of rehabilitation receive the highest dosage, whereas patients with lower mobility levels and infrequent rehabilitation receive the lowest dose. Our method is based on our previous published studies demonstrating that the mobility levels obtained in the first 3 rehabilitation sessions predict, or at minimum, associate with patient-centered outcomes.^9,10^
Measurements and Main Results
Descriptive statistics were reported as mean ± SD, median [IQR], or n (%) as appropriate. A total of 3780 patients with COVID critical illness were included. Patients were stratified into groups according to discharge disposition (in-hospital death, subacute or long-term care facility, acute rehabilitation facility, home with services, or home independent). The change in mobility level during rehabilitation as measured by JH-HLM among discharge groups was compared using a two-way ANOVA. Dose of rehabilitation between discharge disposition groups was compared using Tukey’s multiple comparison test. Univariate analyses (Spearman’s correlation) were performed to assess associations between rehabilitation parameters and functional outcomes. Multivariate linear regression was performed to analyze the association between rehabilitation dose and discharge AM-PAC scores, which defined physical function among survivors, adjusting for pre-specified covariates including age, sex, body mass index (BMI), ICU length of stay, and receipt of mechanical ventilation.
Patients demographics are described in Table 1. The cohort was a mean 64 ± 16 years old, 41% female and mean BMI of 32 ± 9 kg/m^2^. Mechanical ventilation was required in 46% (n=1739), and the median hospital LOS was 12 days (IQR 7–21). A total of 2200 (58%) and 1698 (45%) patients received at least one PT and OT session, respectively. The first rehabilitation session occurred 7.5 ± 8.0 days after ICU admission. Patients received PT at a frequency of 0.22 ± 0.14 days a week and OT at a frequency of 0.18 ± 0.11 days a week, equivalent to 2.8 rehabilitation sessions per week. Mobility levels on the JH-HLM scale generally increased from the first to last session (+0.93 ± 2.1). The mean JH-HLM score for all sessions was 4.6 ± 1.7; this suggests a likely ability to transfer from a bed to a chair but not stand for up to one minute. The mean dose of physical rehabilitation was 1.8 ± 1.3 units.
Patients who died in the hospital (n = 994, 26%) were older, more likely to require mechanical ventilation, had longer durations of mechanical ventilation, and longer ICU LOS (Table 1) compared to patients who survived to hospital discharge. Compared to survivors, those who died in the hospital had an earlier start of rehabilitation, but had lower frequencies of rehabilitation, achieved lower levels of mobility, and received a lower dose of physical rehabilitation (Table 1). Stratified by discharge disposition, patients discharged to home had the highest dose of rehabilitation (F = 69, p <0.0001; Figure 1).
For 2191 patients with complete data, mean AM-PAC scores at discharge were 15.6 ± 5.9; similar to the JH-HLM mean score, this suggests requiring a lot of help for bed-to-chair transfers.^11^ Rehabilitation dose and AM-PAC at discharge were moderately, positively associated (Spearman’s rho [r] = 0.484, p < 0.001). Physical function at discharge as measured by AM-PAC was significantly associated with average mobility achieved in first 3 sessions (r = 0.799, p < 0.001), change in mobility from first to last session (r = 0.445, p < 0.001), and PT and OT frequency with physical function (r = 0.130, p < 0.001). Multivariate linear regression (model adjusted R^2^= 0.68, p <0.001) demonstrates mechanical ventilation (β = −0.86, p =0.001), average mobility score in first three sessions (β = 2.6, p <0.001) and physical rehabilitation dosage (β = 0.22, p = 0.001) were predictive of AM-PAC scores at discharge when controlling for age, sex, BMI, and ICU LOS.
Conclusions
Our expansive study, involving over 3700 critically ill patients with COVID-19 at four medical insitutions, underscores the pivotal role of physical rehabilitation exposure in the ICU, demonstrating a significant correlation with favorable hospital outcomes. This findings aligns with previous research highlighting the positive association between rehabilitation frequency and outcomes in COVID-19 patients, albeit not specifically focusing on those with critical illness.^12^ Introducing a novel methodology, we measure rehabilitation dose by assessing both session frequency and a surrogate marker of intensity derived from achieved mobility levels during sessions. Although our approach lacks physiologic dosage markers such as vital signs, and duration of intensity, it introduces a groundbreaking method for quantifying ICU rehabilitation dose with a single unit. Adopting this approach may enable ICU rehabilitation programs to specifically delineate the intervention provided and anticipate patient benefit. In future, stratification and phenotypic analysis accounting for dose hold promise to guide interventions in clinical research settings. this approach may be useful for prescribing interventions in clinical research.
Precision exercise, dose-reponse, and individual response heterogeneity are concepts in exercise dosing that are known to impact outcomes in older adults and diverse patient populations.^13–15^ The intra-individual variations have also been recognized in critical care with ventilatory and pharmaceutical interventions.^16,17^ To improve the ICU rehabilitation field, it is imperative that clinicians and researchers examine the dose-response. As clinicians, we must modify and adjust treatments based on patient- and clinical-related factors to enhance outcomes. Our work as well as other research demonstrates that older individuals and patients with chronic disease respond differently to exercise.^10,18^ Thus, we strongly suggest that researchers and clinicians must begin to examine the response to targeted or individualized rehabilitation dose.
Our study has several strengths including a large sample size from multiple academic medical centers with high functioning ICU rehabilitation programs. We also used real world data directly from each rehabilitation session provided to create our method. The study also has limitations. The retrospective study design limits our ability to draw definitive conclusions with regard to causation and is at risk of residual confounding, so our findings should be considered hypothesis-generating. Additionally, while we adjusted for receipt of MV and ICU length of stay, patients who survived may have had lower severity of illness and thus participated at higher levels of mobility with rehabilitation, regardless of the dose. Lastly, we could not account for duration of exercise intensity in our models; longer physiologic demands may produce additional benefits. In conclusion, we found that greater dose of rehabilitation during critical illness due to COVID-19 was associated with improved outcomes. Future studies should utilize personalized rehabilitation doses and identify the most optimal personalized dosage of rehabilitation in critically ill patients, including those with COVID-19.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Devlin JW, Skrobik Y, Gélinas C, Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit Care Med 2018;46(9):e 825–e 873. (In eng). DOI: 10.1097/ccm.0000000000003299.30113379 · doi ↗ · pubmed ↗
- 2Morris PE, Berry MJ, Files DC, Standardized Rehabilitation and Hospital Length of Stay Among Patients With Acute Respiratory Failure: A Randomized Clinical Trial. JAMA 2016;315(24):2694–702. DOI: 10.1001/jama.2016.7201.27367766 PMC 6657499 · doi ↗ · pubmed ↗
- 3Moss M, Nordon-Craft A, Malone D, A Randomized Trial of an Intensive Physical Therapy Program for Patients with Acute Respiratory Failure. American journal of respiratory and critical care medicine 2016;193(10):1101–10. (In eng). DOI: 10.1164/rccm.201505-1039 OC.26651376 PMC 4872662 · doi ↗ · pubmed ↗
- 4Tipping CJ, Harrold M, Holland A, Romero L, Nisbet T, Hodgson CL. The effects of active mobilisation and rehabilitation in ICU on mortality and function: a systematic review. Intensive Care Med 2017;43(2):171–183. (In eng). DOI: 10.1007/s 00134-016-4612-0.27864615 · doi ↗ · pubmed ↗
- 5Jolley SE, Moss M, Needham DM, Point Prevalence Study of Mobilization Practices for Acute Respiratory Failure Patients in the United States. Crit Care Med 2017;45(2):205–215. (In eng). DOI: 10.1097/ccm.0000000000002058.27661864 PMC 5520580 · doi ↗ · pubmed ↗
- 6Nydahl P, Ruhl AP, Bartoszek G, Early mobilization of mechanically ventilated patients: a 1-day point-prevalence study in Germany. Crit Care Med 2014;42(5):1178–86. (In eng). DOI: 10.1097/ccm.0000000000000149.24351373 · doi ↗ · pubmed ↗
- 7Myszenski A, Bello R, Melican C, Pfitzenmaier N. Patient Characteristics and Acute PT and OT Utilization During the Initial Surge of COVID-19: A Retrospective Observational Study. J Acute Care Phys Ther 2022;13(1):2–7. (In eng). DOI: 10.1097/jat.0000000000000163.34925956 PMC 8670083 · doi ↗ · pubmed ↗
- 8Jette DU, Stilphen M, Ranganathan VK, Passek SD, Frost FS, Jette AM. Validity of the AM-PAC “6-Clicks” inpatient daily activity and basic mobility short forms. Physical therapy 2014;94(3):379–91. (In eng). DOI: 10.2522/ptj.20130199.24231229 · doi ↗ · pubmed ↗