Lung Diffusion Capacity in Patients With Bilateral COVID-19 Pneumonia: A Three-Month Follow-Up Study
Marina Vasilj, Kristina Galic, Tanja Zovko, Gordana Kraljevic, Nikolina Pravdic, Belma Saric-Zolj, Marija Goluza Sesar, Danijel Pravdic

TL;DR
This study tracks lung function recovery in patients with severe but non-critical COVID-19 pneumonia over three months.
Contribution
The study provides new insights into the timeline of lung function recovery in non-critical bilateral COVID-19 pneumonia patients.
Findings
Lung function parameters like FEV1 and DLCO improved significantly three months after infection.
DLCO/SB remained below normal even after three months.
Patients showed partial recovery one month post-infection but significant improvement by three months.
Abstract
Objectives: The aim of this study was to determine the short-term consequences of coronavirus disease 2019 (COVID-19) infection on pulmonary diffusion in patients with severe (but not critical) and moderately severe COVID-19 pneumonia during three months after COVID-19 infection. Methods: A prospective study included 81 patients with an RT-PCR-test confirmed diagnosis of COVID-19 infection treated in the COVID Department of Lung Diseases of University Clinical Hospital Mostar. Inclusion criteria were ≥18-year-old patients, COVID-19 infection confirmed using real-time RT-PCR, radiologically confirmed bilateral COVID-19 pneumonia, and diffusion capacity of the lungs for carbon monoxide (DLCO) one and three months after COVID-19 infection. The pulmonary function was tested using the MasterScreen Body Jaeger (Jaeger Corporation, Omaha, USA) and MasterScreen PFT Jaeger (Jaeger Corporation,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
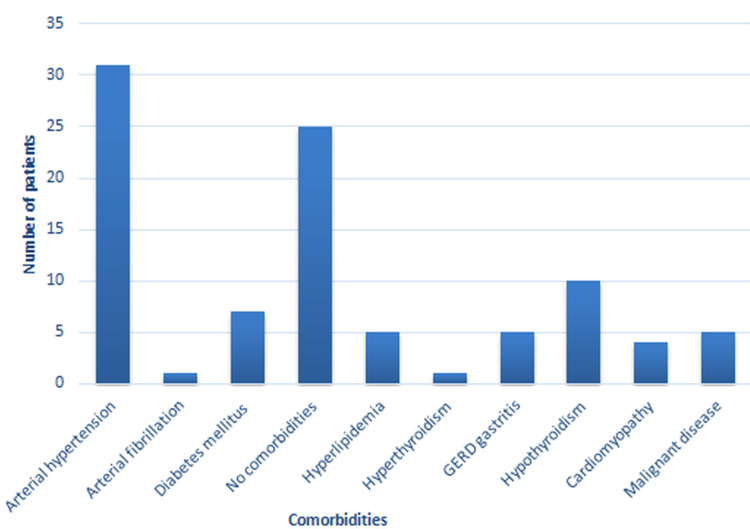 Figure 1
Figure 1| Place of treatment | Sex | N | % | Median age | Maximum age | Minimum age |
| Other hospitals | Male | 14 | 17 | 56 | 77 | 31 |
| Female | 8 | 10 | 60 | 83 | 26 | |
| University Clinical Hospital Mostar | Male | 31 | 38 | 64 | 84 | 33 |
| Female | 28 | 35 | 65 | 81 | 25 |
| Spirometry parameter | Point of measurement | N | M | SD | t | df | p |
| FVC | first-month | 81 | 89.4 | ± 17.0 | -6.44 | 80 | .000 |
| three-month control | 81 | 95.0 | ±17.1 | ||||
| FEV1 | first-month | 81 | 94.2 | ±19.2 | -4.25 | 80 | .000 |
| three-month control | 81 | 98.2 | ±19.8 | ||||
| FEV1/FVC | first-month | 81 | 85.3 | ±8.6 | 3.38 | 80 | .001 |
| three-month control | 81 | 83.4 | ±8.5 |
| Diffusion parameter | Point of measurement | N | M | SD | t | df | p |
| DLCO/SB | first-month | 81 | 63.2 | ±17.3 | -7.65 | 80 | .000 |
| three-month control | 81 | 73.0 | ±18.8 | ||||
| DLCO/VA | first-month | 81 | 78.1 | ±16.6 | -6.10 | 80 | .000 |
| three-month control | 81 | 85.6 | ±17.6 | ||||
| TLC | first-month | 81 | 84.5 | ±15.5 | -4.62 | 80 | .000 |
| three-month control | 81 | 88.5 | ±13.9 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Long-Term Effects of COVID-19 · COVID-19 Clinical Research Studies
Introduction
Emerging viral diseases have become a major public health problem [1]. Coronavirus disease 2019 (COVID-19) is disease caused by the SARS-CoV-2 [2,3]. During various stages, symptomatology of COVID-19 is different. The most frequent clinical symptoms are fatigue, shortness of breath, cough, fever, and sputum production [4,5].
The health consequences of COVID-19 remain largely unclear [6]. The literature reports that patients may have persistent impairment in diffusion capacities after hospitalization [7]. Different pathophysiological events include diffuse alveolar epithelium destruction, hyaline membrane formation, capillary damage and bleeding, alveolar septal fibrous proliferation, and pulmonary consolidation [8].
Pulmonary function tests (PFTs), such as spirometry, diffusion capacity, and lung volumes, are mostly used for functional respiratory evaluations [9,10]. Chest computed tomography (CT) abnormalities may cause pulmonary fibrosis and should be analyzed together with lung function [11,12]. Patients who have severe COVID-19 pneumonia should be evaluated with full PFTs 12 weeks after hospitalization [13]. The first analysis of lung function showed that patients have a restrictive defect and a small airway dysfunction that can be persistent and not related to the disease severity [14]. The number of studies on the frequency and relevant predictors of COVID-19-related pulmonary sequelae is still limited with varying results [15].
Thus far, studies have not clearly determined the health consequences of COVID-19 patients. We designed our prospective study to investigate the prevalence of disturbances in the values of spirometric parameters and disturbances in diffusion parameters in post-COVID-19 patients and to investigate recovery of pulmonary function in these patients. This research might contribute to a better understanding of the impact of COVID-19 infection on respiratory function in the early recovery period to prevent long-term outcomes.
Materials and methods
Study design and study population
The prospective study was conducted in the period from 2021 to 2022 and included patients with COVID-19 infection treated at the COVID Department of Lung Diseases of the University Clinical Hospital Mostar (UCH Mostar), Cantonal Hospital Livno, and Cantonal Hospital, Dr. Safet Mujić“ Mostar. Subjects were ≥ 18-year-old patients diagnosed with COVID-19 infection. Criteria for inclusion of patients were aged over 18 with severe unstable, but not critical, COVID-19 disease (The Modified Early Warning Score, MEWS 3-4) and moderately severe stable disease (MEWS ≤ 3) with comorbidity, according to the guidelines issued by the World Health Organization (WHO) in 2020 [16]. Severe unstable, but not critical illness (MEWS 3-4) was defined as illness with clinical or laboratory signs of the impaired ratio of arterial partial pressure of oxygen to fraction of inspired oxygen, with breathing shortness, dyspnea, tachypnea, need for oxygen supplementation >4 liters per minute for regaining oxygen saturation measured by pulse oximetry above 92%, but without critical signs (impairment of consciousness, septic shock) [3]. Diffusion capacity of the lungs for carbon monoxide (DLCO) using a single-breath technique method adjusted for hemoglobin was performed one month and three months after COVID-19 infection. According to the Global Lung Function, we classified patients with normal DLCO (≥80% predicted) or altered DLCO (<80% predicted) [17]. Exclusion criteria were patients with a history of chronic lung disease or severe lung comorbidities (such as pulmonary resection, pulmonary embolism, pre-existing interstitial lung disease) and patients incapable of completing pulmonary functional tests due to any reason. This clinical study was approved by the Ethics Committee of the UCH Mostar where the study was conducted (no. 1494/23). Our study was performed following the ethical standards of the Helsinki Declaration of 1975, as revised in 2000.
Data collection
We evaluated patients during hospitalization treatment for COVID-19 infection and three months after the infection in a nine-month period. The pulmonary function test was done in the Lung Function Laboratory of UCH Mostar. The MasterScreen Body Jaeger (Jaeger Corporation, Omaha, USA) was used for performing spirometry and MasterScreen PFT Jaeger (Jaeger Corporation, Omaha, USA) was for performing diffusion capacity of the lungs for carbon monoxide (DLCO) according to the American Thoracic Society guidelines one and three months after COVID-19. We analyzed the following parameters: FVC (forced vital capacity), FEV1 (forced expiratory volume in one second), FEV1/FVC (forced expiratory volume/forced vital capacity), DLCO/SB (single-breath diffusing capacity of the lung for CO), DLCO/VA (diffusing capacity for carbon monoxide divided by the alveolar volume), and TLC (total lung capacity) at first-month control. The patients came for follow-up after three months and the same parameters were analyzed again.
Statistical analysis
For this work, differences in the average values of individual parameters that describe the state of the disease at the time of admission and the state at the follow-up examination after three months were tested with the statistical T-test of dependent samples. For this test, data matching with a normal distribution was tested. The Shapiro-Wilk test was used to test normality. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 20 (Released 2011; IBM Corp., Armonk, New York, United States).
Results
We included 81 subjects, aged from 27 to 89 years. The average age was 60 years, 45 men (56%) and 36 (44%) women. Patients were treated at the COVID Department of Lung Diseases of the UCH Mostar and in other hospitals. The number of patients treated in other hospitals (Cantonal Hospital Livno and Cantonal Hospital, Dr. Safet Mujić“ Mostar) was 22 (27%), while 59 (73%) patients were admitted to our department for hospital treatment (Table 1).
The number of smoking patients in the sample was 31%. That is, 25 patients were active smokers or ex-smokers at the time of admission for examination. The frequency distribution of comorbidities in patients in the sample is given in Figure 1.
Prevalence of comorbidities in patientsGERD: Gastroesophageal reflux disease
The difference between the FVC level in the patients from the first-month control and the FVC level after the three-month control was tested using a t-test of dependent samples. According to the results of the t-test, a statistically significant increase in the value of FVC was determined from the admission of the patient (M=89.4; SD=17.0) to the control after three months (M=95.0; SD=17.1), t (80)=-6.44; p<0.0005 (Table 2).
According to the results of the t-test for the FEV1 parameter, it can be concluded that there was a statistically significant increase in the FEV1 value from the first-month control of the patient (M=94.2; SD=19.2) until control after three months (M=98, 2; SD=19.8), t(80)=-4.25; p<0.0005 (Table 2).
The patients' FEV1/FVC ratio was analyzed from the first-month control (M=85.3; SD=8.6) and at the control after three months (M=83.4; SD=8.5). The results of the t-test of dependent samples showed that the decrease in the value of the tested FEV1/FVC ratio was statistically significant t(80)=3.38; p<0.005 (Table 2).
The dependent samples t-test was used to test the difference between the DLCO/SB level from the first-month control and the DLCO/SB level after three months. According to the results of the t-test, a statistically significant increase in the value of DLCO/SB was determined from the first-month control (M=63.2; SD=17.3) to the control after three months (M=73.0; SD=18.8), t (80)=-7.65; p<0.0005 (Table 3).
The dependent samples t-test was used to test the difference between the DLCO/VA level during the first months of control and the DLCO/VA level after three months. According to the results of the t-test, a statistically significant increase in the DLCO/VA value was found from the first-month control (M=78.1; SD=16.6) to the control after three months (M=85.6; SD=17.6), t(80)=-6.10; p<0.0005. Our study showed that recovery of DLCO/VA was complete after three months, and DLCO/SB was below normal values even after three months (Table 3).
The TLC value of the patients was analyzed during the first-month control (M=84.5; SD=15.5) and at the control after three months (M=88.5; SD=13.9). The results of the t-test of dependent samples showed that the increase in the value of the tested TLC was statistically significant t(80)=-4.62; p<0.0005 (Table 3).
Discussion
In the prospective study of 81 subjects, we analyzed short-term consequences on pulmonary function in patients for three months after COVID-19 infection.
The patients surviving COVID-19 are frequently reported to have pulmonary sequelae [17,18]. The previous reports show that patients may have persistent impairment in respiratory function [19]. The first reports on lung function in these patients showed a restrictive defect and a small airway dysfunction that can be persistent and not related to the severity of the disease [14]. Authors reported diffusion capacity impairment followed by restrictive ventilatory defects, which are connected with disease severity [8]. In the international guidance on the management of COVID-19, 60% of experts were in favor of routine post-hospital PFT within 30-60 days regardless of the disease severity [18]. A few descriptive reports showed a substantial prevalence of altered DLCO percentage in survivors [19-21]. Pulmonary function, particularly DLCO, declined in COVID-19 survivors [22]. Patients with DLCO impairment have a higher percentage of interstitial pulmonary damage. Also, DLCO% performed four months after COVID-19 was the most important, independent correlate of more severe initial disease [11].
The critical period for diffusion capacity recovery is the first three months. This can be connected with capillary component damage recovery and accessible alveolar volume reduction [23]. Data from a study by Qin et al. pointed out that 44 (54%) of 81 patients had abnormal DLCO three months after COVID-19 (<80% predicted) [24]. Our study shows early recovery of pulmonary function in the first three months. The DLCO/SB was 63.2% at discharge and significantly improved to 73.0% at three months. The transfer coefficient of the lung for carbon monoxide (KCO)% pred significantly increased from 78.1% at discharge to 85.6% at three months. Our study showed that recovery of DLCO/VA was complete after three months, and DLCO/SB was below normal values even after three months. The change rates of DLCO% pred and KCO% were significantly higher in 0-3 months. It is important to address whether the DLCO assessment, in addition to spirometry, can be considered in routine clinical follow-ups of COVID-19 patients [24]. Early lung rehabilitation and individualized approach to recovery are worthy of additional investigation [25]. Lung function tests may be regarded as indispensable tools for monitoring functional impairment, planning rehabilitation, managing complications, and preventing long-term outcomes [26].
The limitation of our study it is a single-center study. Also, the initial values of the pulmonary functional tests were not available because the patients did not perform the tests upon discharge due to the severity of the disease, or due to epidemiological measures. Pulmonary function data before COVID-19 infection are lacking even though patients with chronic respiratory diseases were excluded from the study.
Conclusions
Patients with COVID-19 pneumonia significantly recover their lung function in the first month after COVID-19 infection. The parameter that did not recover even after three months was DLCO/SB, suggesting that disease effects on lung diffusion might be the limiting recovery factor in COVID-19 patients. Early monitoring is important in predicting the long-term consequences of COVID-19 pneumonia on lung function.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Severe acute respiratory syndrome coronavirus as an agent of emerging and reemerging infection Clin Microbiol Rev Cheng VC Lau SK Woo PC Yuen KY 6606942020071793407810.1128/CMR.00023-07PMC 2176051 · doi ↗ · pubmed ↗
- 2COVID-19: what is next for public health?Lancet Heymann DL Shindo N 54254539520203206131310.1016/S 0140-6736(20)30374-3PMC 7138015 · doi ↗ · pubmed ↗
- 3Q&A: the novel coronavirus outbreak causing COVID-19BMC Med Fisher D Heymann D 571820203210685210.1186/s 12916-020-01533-w PMC 7047369 · doi ↗ · pubmed ↗
- 4Clinical findings in a group of patients infected with the 2019 novel coronavirus (SARS-Cov-2) outside of Wuhan, China: retrospective case series BMJ 0368202010.1136/bmj.m 606PMC 722434032075786 · doi ↗ · pubmed ↗
- 5Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study Lancet Chen N Zhou M Dong X 50751339520203200714310.1016/S 0140-6736(20)30211-7PMC 7135076 · doi ↗ · pubmed ↗
- 6Origin, transmission, diagnosis and management of coronavirus disease 2019 (COVID-19)Postgrad Med J Umakanthan S Sahu P Ranade AV 753758962020 https://pubmed.ncbi.nlm.nih.gov/32563999/3256399910.1136/postgradmedj-2020-138234 PMC 10016932 · doi ↗ · pubmed ↗
- 76-month consequences of COVID-19 in patients discharged from hospital: a cohort study Lancet Huang C Huang L Wang Y 22023239720213342886710.1016/S 0140-6736(20)32656-8PMC 7833295 · doi ↗ · pubmed ↗
- 8Respiratory function in patients post-infection by COVID-19: a systematic review and meta-analysis Pulmonology Torres-Castro R Vasconcello-Castillo L Alsina-Restoy X Solis-Navarro L Burgos F Puppo H VilaróJ 3283372720213326207610.1016/j.pulmoe.2020.10.013PMC 7687368 · doi ↗ · pubmed ↗