Assessing the Variation in COVID-19 Severity Among the Different Nationalities Living in Qatar
Wafa Ibrahim, Razi Mahmood, Elmobashar Farag, Devendra Bansal, Mohamed Alfaki, Hamad E Al-Romaihi, Mohammed Al-Thani, Rohayu Binti Hami

TL;DR
This study examines how the severity of COVID-19 varies among different nationalities in Qatar, finding significant differences linked to vaccination status.
Contribution
The study provides new insights into how nationality correlates with the severity of COVID-19 and highlights disparities in health outcomes.
Findings
Eastern Mediterranean nationalities had the highest disease severity at 40%.
Vaccination status was significantly correlated with disease severity.
Southeast Asian and Western Pacific groups showed lower severity rates compared to Eastern Mediterranean groups.
Abstract
Background Coronavirus disease (COVID-19) is a highly infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and it has resulted in a global pandemic. The COVID-19 pandemic has resulted in numerous reports on clinical outcomes and risk factors associated with morbidity and mortality. However, the extent to which nationality influences the severity of COVID-19 is not fully understood. Therefore, this study aimed to explore disparities in COVID-19 severity among individuals of different nationalities in Qatar. Methods This is a retrospective study. Secondary data were obtained from the Ministry of Public Health in Qatar. Patients of different nationalities were categorized into different groups based on the WHO regional classification, and the severity of COVID-19 across these groups was analyzed. Results Data were obtained for 96,728 patients.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
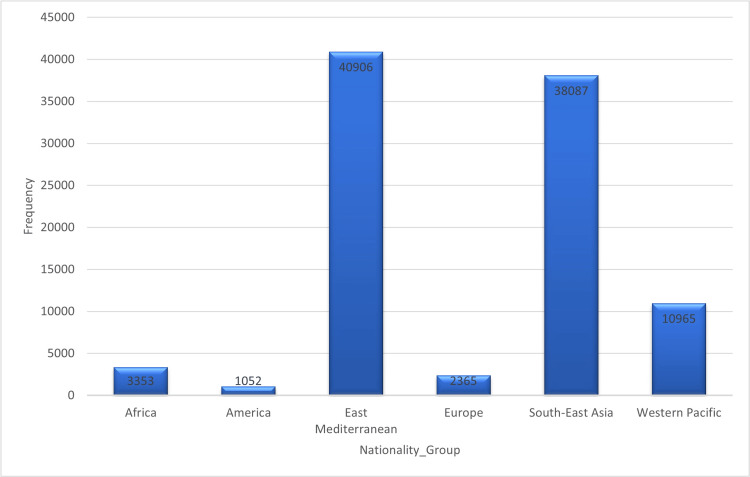 Figure 1
Figure 1| Severity | ||||||
| Asymptomatic | Symptomatic | Severe | Total | *P value | ||
| Nationality group | Africa | 2,429 | 823 | 9 | 3,261 | <0.001 |
| America | 741 | 292 | 1 | 1,034 | ||
| East Mediterranean | 26,631 | 13,112 | 68 | 39,811 | ||
| Europe | 1,708 | 604 | 5 | 2,317 | ||
| Southeast Asia | 24,413 | 13,038 | 65 | 37,516 | ||
| Western Pacific | 6,684 | 4,095 | 21 | 10,800 | ||
| Gender | Male | 40,887 | 20,736 | 115 | 61,738 | NS |
| Female | 21,719 | 11,228 | 54 | 33,001 | ||
| Age group | 0-19 | 12,399 | 4,943 | 30 | 17,372 | <0.001 |
| 20-39 | 25,142 | 12,321 | 63 | 37,526 | ||
| 40-59 | 22,369 | 13,091 | 69 | 35,529 | ||
| ≥ 60 | 2,696 | 1,609 | 7 | 4,312 | ||
| Vaccine status | Unvaccinated | 15,662 | 5,991 | 38 | 21,691 | <0.001 |
| First dose | 390 | 260 | 3 | 653 | ||
| Second dose | 27,660 | 14,705 | 79 | 42,444 | ||
| Booster | 18,894 | 11,008 | 49 | 29,951 | ||
| Vaccine type | Null | 15,662 | 5,991 | 38 | 21,691 | <0.001 |
| SARS-CoV-2(AstraZeneca) | 554 | 243 | 2 | 799 | ||
| SARS-CoV-2 (Moderna) | 14,647 | 8,524 | 45 | 23,216 | ||
| SARS-CoV-2 (Pfizer) | 31,621 | 17,164 | 83 | 48,868 | ||
| SARS-CoV-2 (Pfizer) Pediatrics | 122 | 42 | 1 | 165 | ||
| Comorbidities | Diabetes | 5,118 | 4,095 | 14 | 9,227 | <0.001 |
| HTN | 5,739 | 4,392 | 22 | 10,153 | <0.001 | |
| CVD | 1,109 | 808 | 4 | 1,921 | <0.001 | |
| Dyslipidemia | 4,202 | 3,196 | 12 | 7,410 | <0.001 | |
| Asthma | 2,329 | 1,751 | 8 | 4,088 | <0.001 | |
| Cancer | 504 | 256 | 3 | 763 | NS | |
| Kidney | 504 | 396 | 3 | 903 | <0.001 | |
| Obesity | 2,577 | 1,874 | 11 | 4,462 | <0.001 | |
| Death | Death | 21 | 10 | 42 | 75 | <0.001 |
| Nationality group | No. of cases | Asymptomatic | Symptomatic | Hospitalization | ICU/Tracheostomy | Death | ||||||
| N | % | N | % | N | % | N | % | N | % | N | % | |
| Africa | 3,353 | 3.5% | 2,429 | 72.4% | 823 | 24.5% | 17 | 0.50% | 9 | 0.3% | 3 | 0.08% |
| America | 1,052 | 1.1% | 741 | 70.4% | 292 | 27.7% | 3 | 0.28% | 1 | 0.1% | 2 | 0.19% |
| East Mediterranean | 40,906 | 42.3% | 26,631 | 65.1% | 13,112 | 32.1% | 171 | 0.41% | 68 | 0.2% | 23 | 0.05% |
| Europe | 2,365 | 2.4% | 1,708 | 72.2% | 604 | 25.5% | 9 | 0.38% | 5 | 0.2% | 2 | 0.08% |
| Southeast Asia | 38,087 | 39.4% | 24,413 | 64% | 13,038 | 34.2% | 173 | 0.45% | 65 | 0.2% | 38 | 0.09% |
| Western Pacific | 10,965 | 11.3% | 6,684 | 61.9% | 4,095 | 37.9% | 53 | 0.48% | 21 | 0.2% | 7 | 0.06% |
| Total | 96,728 | 100% | 62,606 | 66.1% | 31,964 | 33.7% | 426 | 0.4% | 169 | 0.2% | 75 | 0.1% |
| Comorbidities | Nationality groups | ||||||||||||
| Africa | America | East Mediterranean | Europe | Southeast Asia | Western Pacific | P value | |||||||
| No. of cases | 3,353 | 3.5% | 1,052 | 1.1% | 40,906 | 42.3% | 2,365 | 2.4% | 38,087 | 39.4% | 10,965 | 11.3% | |
| HTN | 89 | 2.7% | 112 | 10.6% | 3,348 | 8.2% | 169 | 7.1% | 4,499 | 11.8% | 2,132 | 19.4% | <0.001 |
| Diabetes | 63 | 1.9% | 65 | 6.2% | 3,517 | 8.6% | 96 | 4.1% | 4,626 | 12% | 1,044 | 9.5% | <0.001 |
| CVD | 5 | 0.1% | 24 | 2.3% | 750 | 1.8% | 35 | 1.5% | 934 | 2.5% | 206 | 1.9% | <0.001 |
| Dyslipidemia | 31 | 0.9% | 96 | 9.1% | 3,383 | 8.3% | 140 | 5.9% | 2,977 | 7.8% | 928 | 8.5% | <0.001 |
| Asthma and COPD | 38 | 1.1% | 40 | 3.8% | 2,470 | 6% | 78 | 3.3% | 1,156 | 3% | 381 | 3.5% | <0.001 |
| Cancer | 11 | 0.3% | 14 | 1.3% | 379 | 0.9% | 36 | 1.5% | 190 | 0.5% | 151 | 1.4% | <0.001 |
| Kidney | 8 | 0.2% | 11 | 1% | 422 | 1% | 12 | 0.5% | 331 | 0.9% | 140 | 1.3% | <0.001 |
| Obesity | 27 | 0.8% | 59 | 5.6% | 3,483 | 8.5% | 68 | 2.9% | 701 | 1.8% | 224 | 2% | <0.001 |
| Severity | |||||
| Nationality groups | Asymptomatic | Symptomatic | Severe | Total | |
| Africa | Count | 2,429 | 823 | 9 | 3,261 |
| % within severity | 3.9% | 2.6% | 5.3% | 3.4% | |
| % of total | 2.6% | 0.9% | 0.0% | 3.4% | |
| Adjusted residual | 10.3 | -10.4 | 1.3 | ||
| America | Count | 741 | 292 | 1 | 1,034 |
| % within severity | 1.2% | 0.9% | 0.6% | 1.1% | |
| % of total | 0.8% | 0.3% | 0.0% | 1.1% | |
| Adjusted tesidual | 3.8 | -3.8 | -.6 | ||
| East Mediterranean | Count | 26,631 | 13,112 | 68 | 39,811 |
| % within severity | 42.5% | 41.0% | 40.2% | 42.0% | |
| % of total | 28.1% | 13.8% | 0.1% | 42.0% | |
| Adjusted residual | 4.5 | -4.5 | -.5 | ||
| Europe | Count | 1,708 | 604 | 5 | 2,317 |
| % within severity | 2.7% | 1.9% | 3.0% | 2.4% | |
| % of total | 1.8% | 0.6% | 0.0% | 2.4% | |
| Adjusted residual | 7.9 | -7.9 | .4 | ||
| South‒East Asia | Count | 24,413 | 13,038 | 65 | 37,516 |
| % within severity | 39.0% | 40.8% | 38.5% | 39.6% | |
| % of total | 25.8% | 13.8% | 0.1% | 39.6% | |
| Adjusted residual | -5.3 | 5.3 | -.3 | ||
| Western Pacific | Count | 6,684 | 4,095 | 21 | 10,800 |
| % within severity | 10.7% | 12.8% | 12.4% | 11.4% | |
| % of total | 7.1% | 4.3% | 0.0% | 11.4% | |
| Adjusted residual | -9.8 | 9.8 | 4 | ||
| Total | Count | 62,606 | 31,964 | 169 | 169 |
| % within severity | 100.0% | 100.0% | 100% | 100.0% | |
| % of total | 66.1% | 33.7% | 0.2% | 0.2% | |
| Severity | ||||||
| Vaccination status | Ethnic group | Asymptomatic | Symptomatic | Severe | Total | *P value |
| 0 (Not vaccinated) | Africa | 984 | 252 | 5 | 1,241 | < 0.001 |
| America | 217 | 71 | 1 | 289 | ||
| East Mediterranean | 9,912 | 3,873 | 24 | 13,809 | ||
| Europe | 393 | 131 | 1 | 525 | ||
| Southeast Asia | 3,635 | 1,360 | 6 | 5,001 | ||
| Western Pacific | 521 | 304 | 1 | 826 | ||
| Total | 15,662 | 5,991 | 38 | 21,691 | ||
| First dose | Africa | 27 | 10 | 0 | 37 | < 0.001 |
| America | 2 | 1 | 0 | 3 | ||
| East Mediterranean | 145 | 111 | 1 | 257 | ||
| Europe | 12 | 7 | 0 | 19 | ||
| Southeast Asia | 184 | 115 | 2 | 301 | ||
| Western Pacific | 20 | 16 | 0 | 36 | ||
| Total | 390 | 260 | 3 | 653 | ||
| Second dose | Africa | 1,160 | 437 | 4 | 1,601 | < 0.001 |
| America | 271 | 103 | 0 | 374 | ||
| East Mediterranean | 12,677 | 6,754 | 34 | 19,465 | ||
| Europe | 666 | 231 | 3 | 900 | ||
| Southeast Asia | 10,718 | 5,957 | 31 | 16,706 | ||
| Western Pacific | 2,168 | 1,223 | 7 | 3,398 | ||
| Total | 27,660 | 14,705 | 79 | 42,444 | ||
| Third dose | Africa | 258 | 124 | 0 | 382 | < 0.001 |
| America | 251 | 117 | 0 | 368 | ||
| East Mediterranean | 3,897 | 2,374 | 9 | 6,280 | ||
| Europe | 637 | 235 | 1 | 873 | ||
| Southeast Asia | 9,876 | 5,606 | 26 | 15,508 | ||
| Western Pacific | 3,975 | 2,552 | 13 | 6,540 | ||
| Total | 18,894 | 11,008 | 49 | 29,951 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · SARS-CoV-2 and COVID-19 Research · COVID-19 and Mental Health
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), which was first given the name “2019 novel coronavirus." The disease was initially misdiagnosed as severe pneumonia and quickly became a global pandemic [1]. The first outbreak was reported in Wuhan, China, in December 2019, and it was linked to the Huanan seafood market [2]. The World Health Organization (WHO) was alerted to the new disease by Chinese health authorities on December 31, 2019, owing to its high transmission rate and potential to pose a global health threat [2,3]. As the pandemic progressed, reports on clinical outcomes and risk factors for ICU admission and mortality have emerged. The highly transmissible nature of COVID-19 has resulted in numerous studies examining the risk factors for severe outcomes, such as ICU admission and mortality. Although the role of nationality in COVID-19 severity is not yet fully understood, various studies have suggested that both genetic and socioeconomic factors may play a role. Additionally, age and comorbidities such as lung, heart, and metabolic diseases as well as obesity have been strongly associated with severe COVID-19 outcomes. Epigenetic alterations may also contribute to the onset of disease-related complications.
A study revealed that a high level of cytokines indicates a poor prognosis in COVID-19 patients. Additionally, postmortem examination of lung tissues from COVID-19 patients has revealed excessive infiltration of pro-inflammatory cells, involving macrophages and T-helper cells, which may contribute to the poor prognosis. Other studies suggest that a "cytokine storm" may increase the risk of mortality from COVID-19 [4]. The WHO reports that more than 700 million cases and six million deaths have been reported in 220 countries [5]. Qatar is one of the many countries affected by the COVID-19 pandemic. The population of Qatar is approximately 2.6 million, with foreigners comprising the majority. Qatari citizens account for only 12% (313,000) of the population, whereas the remaining 88% (2.3 million) have approximately 94 different nationalities. COVID-19 infections began in Qatar in February 2020, with the first cases identified among travelers returning to the country [6].
Qatar has granted emergency authorization for four vaccines: Pfizer-BioNTech, Moderna, AstraZeneca, and Pfizer-BioNTech for pediatric patients [4]. The vaccination process consists of two doses of the vaccine and a third booster dose. As of February 2022, 87.1% of the total population in Qatar had received at least one dose of the vaccine, while 77% of the population had been fully vaccinated [7]. According to studies conducted in Qatar between February and April 2020, there were 5,685 confirmed COVID-19 cases; 88.9% were male, and 8.7% were Qatari nationals. The highest number of infections occurred in patients from India (27.4%). Among these patients, 83.6% had no concomitant comorbidities, whereas only 3.0% had three or more comorbidities [6]. Qatar is a diverse multinational country with individuals from different ethnic backgrounds, each with unique behaviors, comorbidities, and immune system profiles. Further research is required to identify population-specific risk factors and evidence-based prevention and treatment strategies to reduce the incidence and mortality rate of COVID-19 in Qatar. While studies conducted in Europe and the USA have addressed the association between the severity of COVID-19 and potential risk factors such as ethnicity, no such studies have been conducted in the Middle East or Qatar. Consequently, the significance of nationality, which may affect disease transmission, prognosis, treatment, morbidity, and mortality rates in Qatar, remains unclear. Hence, additional research is necessary to understand and prevent COVID-19 in Qatar's multiethnic population.
This study was conducted to evaluate and disseminate information on the severity of COVID-19 among individuals of diverse nationalities residing in Qatar and identify potential risk factors. This study analyzed the impact of nationality on the severity and mortality rate of COVID-19 in Qatar. The findings of this study will contribute to a better understanding of the morbidity, mortality, and prognosis of COVID-19, aiding in assessing their implications in preventive and predictive medicine.
Materials and methods
Research framework and ethical considerations: This is a retrospective cross-sectional study. It includes laboratory-confirmed COVID-19 cases reported by the Ministry of Public Health (MOPH), Qatar, between January 2021 and February 2022. The study included secondary data provided by the MOPH for patients who were discharged from the hospital or died. The vaccination status, nationality, age, gender, and comorbidities were recorded.
Ethical approval (ERC-826-3-2020) was obtained from the MOPH Ethical Review Board. The Human Research Ethics Committee USM (HREC), University of Sains Malaysia (JEPeM-USM), also reviewed and approved the study protocol (USM/JEPeM/PP/23020198).
Sample size: Stratified random sampling was used to ensure that all WHO regions were sufficiently represented for the appropriate statistical analyses. The researchers stratified the sample by the WHO region and used the Epitools software for a simple random sample within each group. Epitools is a type of sampling tool that researchers and epidemiologists utilize to estimate disease prevalence and randomly select individuals from a population without introducing selection bias [8].
Variables: Patient data were categorized into groups based on WHO regional classifications (Africa, America, Eastern Mediterranean, Europe, Southeast Asia, and the Western Pacific region) [9]. The severity of the disease was categorized into asymptomatic (no symptoms), symptomatic (symptoms but no ICU admission), and severe (symptoms + hospital/ICU admission or death).
Inclusion/exclusion criteria: The inclusion criteria for this study included all confirmed COVID-19 patients living in Qatar, including those who had been discharged from the hospital or had passed away. Nonresident patients were excluded from the study.
Statistical analysis: The data were analyzed using SPSS. Descriptive statistics were used to summarize the demographic characteristics of the patients. Severity in numbers and percentages was analyzed, and the chi-squared test was used to compare the severity of COVID-19 among patients from different regions living in Qatar. Multiple logistic regression analysis was performed to determine the association between vaccination and the severity of COVID-19 among different nationalities living in Qatar. The independent variables were age, gender, and chronic diseases, with disease severity as the dependent variable. The vaccination status was included as an independent variable.
Results
Demographics: Overall, data were obtained from 96,728 patients with confirmed COVID-19. A total of 94,739 data points were analyzed (1,989 individuals had missing data, representing 2.06%, and were excluded from the analysis). The results showed that the Eastern Mediterranean had the highest number of cases, 40,906 (42.3%), followed by Southeast Asia with 38,087 (39.4%), and the Western Pacific with 10,965 (11.3%) groups (see Figure 1). The countries with the most cases were India (24.8%), the Philippines (10.9%), and Nepal (6.6%). The 20-39 age group had the highest number of cases (39.7%), and the average age of the participants was 35.39 years (standard deviation: 15.5) (Table 1).
Number of COVID-19 cases among different nationalities
In this study, there were more males (65.2%) than females (34.8%). Most of the patients were asymptomatic (64.9%). The data also indicated that most patients (77.1%) were vaccinated, while 22.9% were unvaccinated. Among vaccinated individuals, the highest number of cases (44.9%) occurred after the second dose (Table 1).
Table 1 shows that most patients received Pfizer (51.6%), followed by Moderna (24.4%) and AstraZeneca (0.8%).
The analysis revealed a significant association between severity and nationality (p < 0.001).
Hospital/ICU admission and death: A total of 426 patients were hospitalized, 169 of whom required ventilation, and 75 died. There were 31 deaths (41%) among patients aged 29-39 years (Appendix A).
Compared with individuals in other groups, the Western Pacific group reported the highest number of symptoms (7.9%). African patients experienced a slight increase in tracheostomies and ICU admissions (Table 2). The majority of fatalities occurred among Indian patients (23 deaths, 30.7%), followed by Qataris (nine deaths, 12%), Nepalese (eight deaths, 10.7%), and Filipinos (seven deaths, 9.3%) (Appendix B).
Comorbidities: The most prevalent underlying medical conditions in COVID-19 patients were hypertension (10.7%), diabetes (9.7%), and dyslipidemia (7.8%). Patients from the Western Pacific region had the highest incidence of hypertension (19.4%), followed by those from Southeast Asia. Africans were the least vulnerable to hypertension. We also found that Southeast Asians had a higher prevalence of diabetes (12%) and cardiovascular disease (CVD) (2.5%) than other groups. The prevalence of obesity was highest among patients from the Eastern Mediterranean region (8.5%), while Americans had the highest incidence of dyslipidemia (9.1%). Patients from the Eastern Mediterranean region were also at a greater risk of asthma and chronic obstructive pulmonary disease (COPD) (6%) than those from other regions, with the American group showing a lower risk (3.8%). African patients had the lowest prevalence of comorbidities, such as hypertension, diabetes, CVD, dyslipidemia, asthma, and obesity, compared to other groups (Table 3). Our data showed that patients from the Eastern Mediterranean and Southeast Asian groups had a higher prevalence of severe COVID-19 (40% and 38.5%, respectively) than those from the Western Pacific region (12.4%) (Table 4).
Impact of Vaccination on COVID-19 Outcomes in Various Ethnic Groups in Qatar
The results of this study indicated that most COVID-19 patients were vaccinated (77.1%). Among vaccinated individuals, the highest number of cases (44.9%) was observed among those who received the second dose of the COVID-19 vaccine. Of the vaccinated patients, 51.6% received the Pfizer vaccine, followed by Moderna (24.4%), and AstraZeneca (0.8%) vaccines. There was a significant correlation between disease severity and vaccination status (Table 5). Disease severity was greater among individuals who received a single vaccine dose.
Table 5: Vaccination status among different ethnic groups*Statistically significant if the P value was <0.05, calculated using the chi-squared test.
Multinomial logistic regression analysis was performed with severity as the dependent variable and nationality, group, and sex as factors. The logistic regression model fit was significant (p < 0.05). The data show that nationality was a significant predictor (p < 0.05).
Parameter estimates: The reference category was symptomatic, and this parameter was set to zero because it was redundant. The addition of gender and ethnic group variables significantly improved model fit, as indicated by the likelihood ratio tests. The chi-square value for the gender variable was 14.292, with three degrees of freedom and a P value of 0.003, whereas the chi-square value for the ethnic group variable was 476.624, with 15 degrees of freedom and a P value less than 0.001 (Appendix C).
Discussion
This study indicated a statistically significant difference in disease severity among different nationalities. The highest number of patients were from the Eastern Mediterranean group, followed by Southeast Asia. The severity of COVID-19 increased in Eastern Mediterranean individuals, followed by patients from Southeast Asia and the Western Pacific region. To investigate the factors contributing to the global spread of COVID-19, it is important to examine the potential influence of nationality on the disease. Therefore, we analyzed national surveillance reports and articles on COVID-19, focusing on race and ethnicity data and comparing them with surveillance data from Qatar. Many studies have linked poor outcomes of COVID-19 to different nationalities [10-14]. Our study included patients from various countries who received equal levels of healthcare within Qatar's health facilities. Our diverse sample comprised men and women of all ages, representing a broad range of exposure categories. In this study, the severity of COVID-19 varied from asymptomatic to severe.
We hypothesized that nationality and comorbidities would affect the severity of COVID-19. Apparent disparities in infection rates and clinical outcomes exist across different countries. However, there is still a lack of information regarding the effect of nationality on COVID-19 clinical outcomes. Therefore, we focused on the COVID-19 outcomes among residents of Qatar. Our findings revealed that individuals from the Eastern Mediterranean region had the highest percentage of COVID-19 cases, followed by those from Southeast Asia and the Western Pacific. These findings are significant because previous studies have shown that South Asian patients have the highest incidence of COVID-19 [14]. Certain groups, including South Asians, also present higher rates of comorbidities such as diabetes, hypertension, and cardiovascular diseases. These conditions are associated with severe disease and mortality in COVID-19 patients [3]. Our findings align with those of previous research, as we demonstrated that Southeast Asian patients had the highest rates of diabetes (12%) and CVD (2.5%), surpassing those of other groups. Additionally, we found that the majority of patients were males (65.2%), which is consistent with previous reports from China and Italy that also showed associations between risk factors such as sex, age, smoking status, cardiac comorbidities, and increased adverse effects [3]. However, mortality rates differ between Chinese and Italian populations, suggesting that race may impact outcomes [3]. Moreover, among African patients, we observed slight increases in severe symptoms, hospitalizations, and ICU admissions. This finding is consistent with a CDC report that showed that African Americans tend to have an incidence rate of approximately 2.1 times greater and a hospitalization rate of 4.7 times greater than those of the general population [10]. Other studies have demonstrated a significantly increased mortality rate for COVID-19 among Black and minority ethnic populations. In contrast, another study attributed the higher COVID-19-related mortality rate among African American, Black, and Hispanic ethnic groups to disparities in access to healthcare [11,12,14].
One study in Louisiana showed that Blacks accounted for 76.9% of hospitalized patients and 70.6% of deaths, while they constituted only 31% of the Ochsner Health population [13]. In contrast, our findings revealed that African individuals had the lowest comorbidity rate.
The findings of this study highlight the high risk of disease in specific groups, such as Southeast Asians, and the severity of disease associated with comorbidities such as hypertension, diabetes, and obesity. The data showed that patients from the Eastern Mediterranean and Southeast Asian groups had a higher prevalence of diabetes, CVD, asthma, and COPD than those from the other groups. These findings correlate with those of many studies that have found a relationship between comorbidities and disease severity progression in patients. These studies indicate that patients with comorbidities such as hypertension, diabetes, asthma, COPD, and chronic kidney disease were significantly affected in higher proportions, resulting in the requirement of ICU admission and ventilator aid in some cases. In many cases, this increases the risk of developing severe COVID-19 infections and increases the risk of severe clinical outcomes [15-17]. Moreover, several studies on the clinical efficacy and safety of COVID-19 vaccines have shown that the effectiveness of the coronavirus vaccine was 66% in preventing symptomatic disease, 88% for hospitalization, 90% for ICU admission, and 86% for preventing COVID-19-related deaths [18,19]. These findings are consistent with those of our study, which showed a significant correlation between disease severity and vaccination status, consistent with previous studies. Moreover, we observed that disease severity was greater among individuals who received only a single vaccine dose and waned after the second dose.
This study also revealed a significant association between nationality and deaths due to COVID-19. However, further research is needed to support this finding because of the limited sample size.
The results of this study may be utilized to compare disease outcomes among people of various nationalities residing in different environments and affected by various factors. By comparing the results of this study with data from other countries, it is possible to investigate a range of factors that may influence COVID-19 outcomes and contribute to these differences, this includes culture, genetics, age distribution, health policies, access to healthcare, and wealth. This comparison provides valuable insights into the unique characteristics of each population, which may influence variations in severity and mortality rates. Nonetheless, it is essential to acknowledge that the relationship between nationality and health outcomes is intricate and multifaceted.
Recommendations
We believe that further research should be conducted to evaluate the role of nationality in determining COVID-19 incidence and mortality and to identify screening methods, detection methods, and early response strategies.
Limitations of the study
Although this study revealed that certain nationalities may be at a higher risk of developing severe COVID-19 and other diseases, these findings cannot be generalized to all members of a particular group. Moreover, it is important to note that the countries in the WHO region may have different ethnicities. Further research is needed to evaluate the role of ethnicity in the outcomes of COVID-19, which will enable us to better understand the severity of the disease.
Conclusions
This study provides new insights into the severity of COVID-19 among individuals of various nationalities. Furthermore, it emphasizes the importance of healthcare interventions to mitigate disparities in COVID-19 mortality within these groups. Understanding the impact of nationality on the severity of infectious diseases will enable the development of effective methods for detecting and responding to future pandemics, leading to improved national and international surveillance of infectious diseases.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A sporadic COVID-19 pneumonia treated with extracorporeal membrane oxygenation in Tokyo, Japan: a case report J Infect Chemother Nakamura K Hikone M Shimizu H 7567612620203231722510.1016/j.jiac.2020.03.018PMC 7166031 · doi ↗ · pubmed ↗
- 2The continuing 2019-n Co V epidemic threat of novel coronaviruses to global health - the latest 2019 novel coronavirus outbreak in Wuhan, China Int J Infect Dis Hui DS I Azhar E Madani TA 2642669120203195316610.1016/j.ijid.2020.01.009PMC 7128332 · doi ↗ · pubmed ↗
- 3Ethnicity and COVID-19: an urgent public health research priority Lancet Pareek M Bangash MN Pareek N 1421142239520203233042710.1016/S 0140-6736(20)30922-3PMC 7173801 · doi ↗ · pubmed ↗
- 4Cytokine storm in COVID-19: the current evidence and treatment strategies Front Immunol Tang Y Liu J Zhang D Xu Z Ji J Wen C 11202010.3389/fimmu.2020.01708 PMC 736592332754163 · doi ↗ · pubmed ↗
- 5WHO COVID-19 dashboard 4 2024 2024 https://data.who.int/dashboards/covid 19/cases?n=c
- 6Epidemiological investigation of the first 5685 cases of SARS-Co V-2 infection in Qatar, 28 February-18 April 2020 BMJ Open Al Kuwari HM Abdul Rahim HF Abu-Raddad LJ 12202010.1136/bmjopen-2020-040428 PMC 754292733033033 · doi ↗ · pubmed ↗
- 7Total number of vaccine doses administered 7 2023 2023 https://covid 19.moph.gov.qa/EN/Pages/default.aspx
- 8Epitools - random number sampling 7 2023 2023 https://epitools.ausvet.com.au/randomnumbers