COVID-19 was associated with the complications after allogeneic hematopoietic stem cell transplantation
Qi Wen, Ze Guo, Xiao-Hui Zhang, Lan-Ping Xu, Yu Wang, Chen-Hua Yan, Huan Chen, Yu-Hong Chen, Wei Han, Feng-Rong Wang, Yu-Qian Sun, Xiao-Jun Huang, Xiao-Dong Mo

TL;DR
This study shows that the severity and duration of COVID-19 affect complications and outcomes after stem cell transplants.
Contribution
The study links both the duration and severity of COVID-19 to transplant complications for the first time.
Findings
Long-term and serious COVID-19 infections increase risks of poor graft function and mortality after transplants.
Severe or critical illness is associated with lower overall survival rates in transplant patients.
Multivariable analysis confirms the impact of infection severity and duration on transplant outcomes.
Abstract
We aimed to identify the severity and duration of COVID-19 infection on complications after allo-HSCT. Enrolled 179 hospitalized patients with COVID-19 were categorized into long-term infection (> 18 days, n = 90) or short-term infection group (≤ 18 days, n = 89) according to the median duration of COVID-19. The severity of COVID-19 was categorized as asymptomatic infection, mild, moderate, severe, and critical illness according to guidelines of National Institutes of Health. Particularly, severe illness and critical illness were classified as serious infection. Asymptomatic infection, mild illness and moderate illness were classified as non-serious infection. The 150-day probabilities of poor graft function (PGF), cytomegalovirus (CMV) pneumonia and non-relapse mortality (NRM) were significantly higher in long-term infection group. The 150-day probabilities of CMV pneumonia and NRM…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
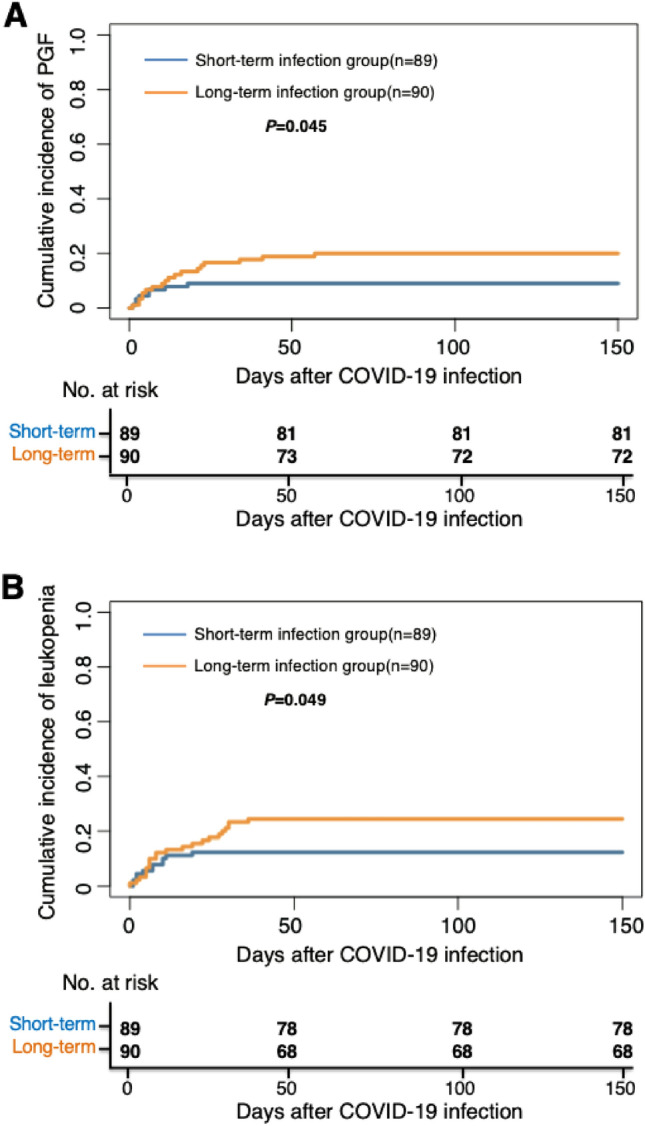 Figure 1
Figure 1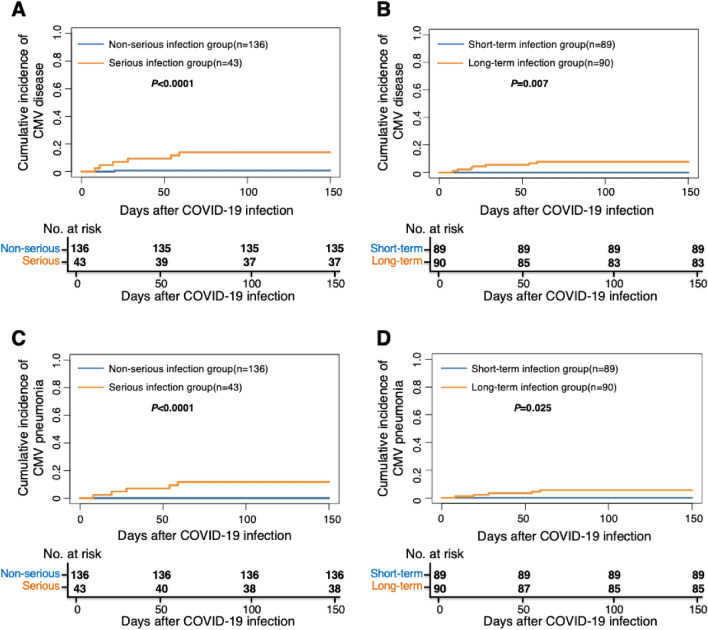 Figure 2
Figure 2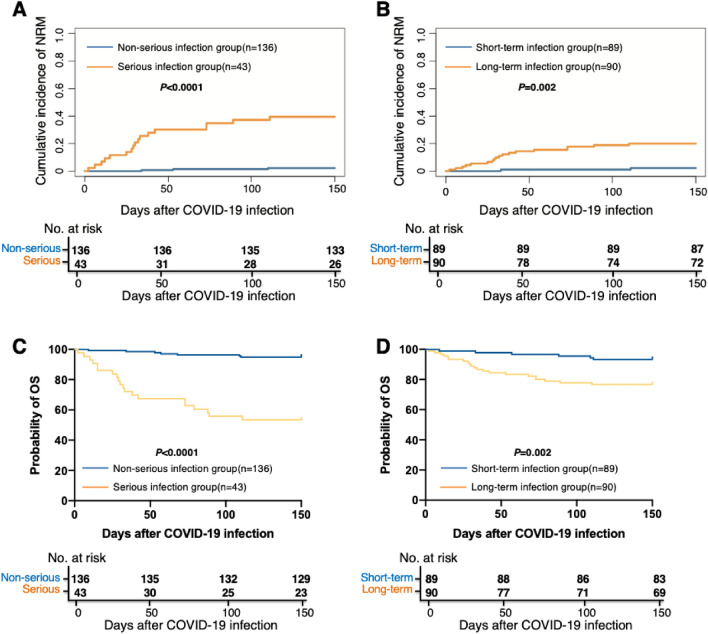 Figure 3
Figure 3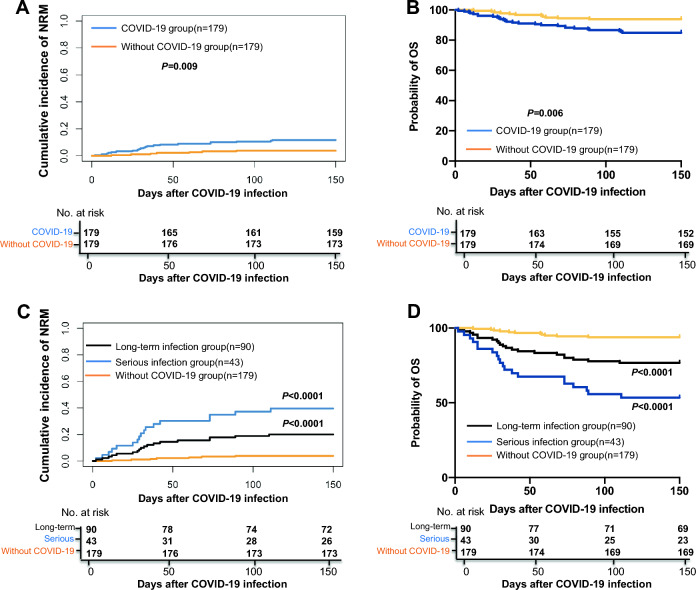 Figure 4
Figure 4- —http://dx.doi.org/10.13039/501100001809National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 Clinical Research Studies · Cytomegalovirus and herpesvirus research · Long-Term Effects of COVID-19
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) provides a potential curative therapy for patients with both malignant and nonmalignant hematological disease^1,2^. Nevertheless, infections, particularly the viral infection, remain one of the most life-threatening complications after allo-HSCT^3,4^.
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) caused Coronavirus Disease 2019 (COVID-19) since the end of 2019 and had caused over 2 million deaths worldwide^5,6^. COVID-19 has also become one of the important viral infections in allo-HSCT recipients^7,8^. Since November 2021, the appearance of Omicron variant and its sublineages further worse the epidemiological situation. Although the lower replication competence of Omicron in the human lungs^9,10^ may cause lower the disease severity^11–13^, the Omicron variant pandemic in Hong Kong from January to March 2022 still cause a COVID-19 mortality rate of 37.7 per million population^14^. Thus, we should not underestimate the harm of Omicron variant infection in allo-HSCT recipients.
Virus could cause several serious complications after allo-HSCT. For example, virus is the most common pathogen of the late-onset severe pneumonia after allo-HSCT and the mortality rate could be as high as 60%^15^. Besides of the direct pathogenesis and injury, viral infections are also associated with several common complications after allo-HSCT. For example, parvovirus B19 infection could cause secondary poor graft function (PGF) and graft rejection^16^. In addition, herpes virus, particularly the human herpesvirus 6 and cytomegalovirus (CMV), is associated with the occurrence of acute graft-versus-host disease (aGVHD)^17–19^. Thus, we speculate that SARS-CoV-2 may also contribute to the occurrence of post-transplant complications.
Although several studies reported COVID-19 infection in allo-HSCT recipients, most of them only focused on the signs, symptoms, prognostics factors, and the treatments and they only reported the characteristics of COVID-19 before 2021 which might be not the same as the Omicron variants. In the Omicron era, several studies have identified the characteristics of COVID-19 in immunocompromised patients, but most of them also only focused on the clinical presentations and treatments of COVID-19, and the sample of allo-HSCT recipients was small^7,8,20–22^. Thus far, no study had focused on the association between occurrence, severity, and duration of COVID-19 infection and complications after allo-HSCT. Particularly, the influence of Omicron variant infection on the post-transplant complications is unclear.
Thus, we aimed to identify the severity and duration of COVID-19 on post-transplant complications in the Omicron era.
Results
Patients’ characteristics
The characteristics of consecutive 179 hospitalized COVID-19 patients were showed in Table 1. The comparison between serious and non-serious infection group was showed in Supplementary Table 1. Forty-three (24%) and 136 (76%) patients were diagnosed as serious and non-serious infection, respectively. The median duration of disease was 18 days (range 2–102) days, and duration of SARS-CoV-2 infection > 18 days and ≤ 18 days was defined as long-term (n = 90) and short-term infection (n = 89), respectively (Supplementary Table 2). The median time from transplantation to COVID-19 infection occurrence was 149 days (range 6–3038) days. A total of 116 (64.8%) patients received immunosuppressants, including cyclosporin (n = 85), tacrolimus (n = 8), ruxolitinib (n = 8), or glucocorticoids (n = 32) when COVID-19 occurrence. Seventeen patients received more than 1 type of immunosuppressants. A total of 144 (80.4%) patients received anti-viral treatment (140 for Paxlovid and 4 for Azvudine). Forty serious infection cases (93.0%) received anti-viral treatment (39 for Paxlovid and 1 for Azifudine), 85 long-term infection cases (94.4%) received anti-viral treatment (83 for Paxlovid and 2 for Azifudine). Sixty-two patients received newly added drugs corticosteroid treatment, that is, 23 (53.5%) and 39 (28.7%) patients were in the serious and non-serious infection group, 9 (10.1%) and 53 (58.9%) patients were in the short- and long-term infection group, respectively.Table 1. Characteristics of allo-HSCT recepient.CharacteristicsCOVID-19 (n = 179)Gender, male/female, n (%)108 (60.3)/71 (39.7)Age(years), range40 (5–75)Underlying disease, n (%) AL131 (73.2) MDS24 (13.4) AA5 (2.8) Lymphoma10 (5.6) Others9 (5.0)Donor match, n (%) HLA-matched sibling donor31 (17.3) HLA-matched unrelated donor6 (3.4) Haploidentical related donor142 (79.3)Blood group matched, n (%) Matched103 (57.5) Minor mismatched30 (16.8) Major mismatched46 (25.7)HCT-CI before HSCT, n (%) 0 (low risk)123 (68.7) 1–2 (intermediate risk)41 (22.9) ≥ 3 (high risk)15 (8.4) Median counts of MNC in graft, range (× 10^8^/kg)9.51 (3.83–19.90) Median counts of CD34^+^ cell in graft, range (× 10^6^/kg)3.08 (0.48–17.20)Conditioning, n (%) Chemotherapy-based168 (93.9) TBI-based11 (6.1)Median counts of lymphocytes at COVID-19 diagnosis, range (× 10^9^/L)1.00 (0.00–6.21)COVID-19, n (%) Asymptomatic infection14 (7.8) Mild illness78 (43.6) Moderate illness44 (24.6) Severe illness22 (12.3)Critical illness21 (11.7)AL acute leukemia, MDS myelodysplastic syndromes, AA aplastic anemia, HLA human leukocyte antigen, HCT-CI hematopoietic cell transplantation–specific comorbidity index, MNC mononuclear cell, TBI total body irradiation.
The severity and duration of COVID-19 and PGF
A total of 26, 33, and 11 patients showed PGF, leukopenia and thrombocytopenia, respectively, after COVID 19 infection. The 150-day cumulative incidence of leukopenia, thrombocytopenia, and PGF was 18.4% (95% confidence interval [CI] 12.7–24.1%), 6.1% (95% CI 2.6–19.6%), and 14.5% (95% CI 9.3–19.7%) respectively, after COVID-19.
The 150-day cumulative incidence of PGF after COVID-19 was 11.8% (95% CI 6.4–17.2%) versus 23.3% (95% CI 10.5–36.1%) (P = 0.071) between non-serious and serious infection group, which was 9.0% (95% CI 3.0–15.0%) versus 20.0% (95% CI 11.7–28.3%) (P = 0.045) between short- and long-term infection group (Fig. 1A).Figure 1. The 150-day cumulative incidence of PGF and leukopenia after COVID-19 between short and long-term infection group. (A) PGF; (B) leukopenia. PGF poor graft function.
The 150-day cumulative incidence of leukopenia after COVID-19 was 19.9% (95% CI 13.2–26.6%) versus 14.0% (95% CI 3.5–24.5%) (P = 0.325) between non-serious and serious infection group, which was 12.4% (95% CI 5.5–19.3%) versus 24.4% (95% CI 15.5–33.3%) (P = 0.049) between short- and long-term infection group (Fig. 1B).
The 150-day cumulative incidence of thrombocytopenia after COVID-19 was 5.1% (95% CI 1.4–8.8%) versus 9.3% (95% CI 0.5–18.1%) (P = 0.331) between non-serious and serious infection group, which was 5.6% (95% CI 0.8–10.4%) versus 6.7% (95% CI 1.5–11.9%) between short- and long-term infection group (P = 0.779).
The median duration of leukopenia, thrombocytopenia, and PGF was 14 days (range 4–118) days, 10 days (range 8–78) days, and 17 days (range 9–78) days, respectively. Until the last follow up, leukopenia, thrombocytopenia and PGF were still persistence 22 patients.
In multivariable analysis, after adjusted by other factors, the duration of COVID-19 was associated with PGF (hazard ratio [HR], 2.31; 95% CI 1.04–5.11; P = 0.039) and leukopenia (HR 2.29; 95% CI 1.04–5.07; P = 0.04) (Table 2). The other risk factors for PGF and leukopenia were showed in Supplementary Table 4.Table 2. Multivariate analysis of risk factors for the 150-day clinical outcomes after COVID-19 infection.OutcomesHR (95% CI)P valuePGF after COVID-19 The duration of COVID-190.039 Short-term1 Long-term2.31 (1.04–5.11)Leukopenia after COVID-19 The duration of COVID-190.040 Short-term1 Long-term2.29 (1.04–5.07)CMV disease after COVID-19 The severity of COVID-190.005 Non-serious1 Serious20.15 (2.43–167.36)NRM after COVID-19 The severity of COVID-19 < 0.0001 Non-serious1 Serious17.26 (4.87–61.21)OS after COVID-19 The severity of COVID-19 < 0.0001 Non-serious1 Serious14.00 (5.87–33.42)PGF poor graft function, CMV cytomegalovirus, NRM non-relapse mortality, OS overall survival.
The severity and duration of COVID-19 and aGVHD
A total of 5 patients showed aGVHD after COVID 19 infection, and the cumulative incidence of total aGVHD was 2.8% (95% CI 0.4–5.2%) after COVID-19. The cumulative incidence of aGVHD after COVID-19 was 3.7% (95% CI 0.5–6.9%) versus 0% (P = 0.204), respectively, between non-serious and serious infection group, which was 3.4% (95% CI 0.4–7.2%) versus 2.2% (95% CI 0.9–5.3%) (P = 0.651), respectively, between short- and long-term infection group. No risk factors were associated with aGVHD in multivariable analysis.
The severity and duration of COVID-19 and chronic GVHD (cGVHD)
A total of 4, 4 and 3 patients showed mild, moderate, and severe cGVHD after COVID 19 infection, and the cumulative incidence of cGVHD was 6.70% after COVID-19. The 150-day cumulative incidence of cGVHD after COVID-19 was 7.4% (95% CI 2.9–11.8%) versus 4.7% (95% CI − 1.7–11.1%), respectively, between non-serious and serious infection group (P = 0.544). The 150-day cumulative incidence of cGVHD after COVID-19 was 6.7% (95% CI 1.5–11.9%) versus 5.6% (95% CI 0.8–10.4%), respectively, between short- and long-term infection group (P = 0.741). No risk factors were associated with cGVHD in multivariable analysis.
The severity and duration of COVID-19 and other infection
A total of 34 and 7 patients showed CMV DNAemia and CMV disease (CMV pneumonia: 5, CMV gastrointestinal disease: 1, CMV encephalitis + retinitis: 1) after COVID 19 infection. The 150-day cumulative incidence of CMV DNAemia after COVID-19 was 19.9% (95% CI 13.2–26.6%) versus 11.6% (95% CI 1.9–21.3%) (P = 0.204), respectively, between non-serious and serious infection group, which was 14.6% (95% CI 7.2–22.0%) versus 23.3% (95% CI 14.5–32.1%) (P = 0.118), respectively, between short- and long-term infection group. The 150-day cumulative incidence of CMV disease after COVID-19 was 0.7% (95% CI 0.7–2.1%) versus 14.0% (95% CI 3.5–24.5%) (P < 0.0001, Fig. 2A), respectively, between non-serious and serious infection group, which was 0% versus 7.8% (95% CI 2.2–13.4%) (P = 0.007, Fig. 2B), respectively, between short- and long-term infection group. Particularly, the 150-day cumulative incidence of CMV pneumonia after COVID-19 was 0% versus 11.6% (95% CI 1.9–21.4%) (P < 0.0001, Fig. 2C), respectively, between non-serious and serious infection group, which was 0% versus 5.6% (95% CI 0.8–10.4%) (P = 0.0245, Fig. 2D), respectively, between short- and long-term infection group. In multivariable analysis, after adjusted by other factors, the severity of COVID-19 was associated with CMV disease (HR, 20.15; 95% CI 2.43–167.36, P = 0.005) (Table 2).Figure 2. The association between COVID-19 and CMV disease. The 150-day cumulative incidence of CMV disease after COVID-19 between (A) non-serious and serious infection group; (B) short and long-term infection group. The 150-day cumulative incidence of CMV pneumonia after COVID-19 between (C) non-serious and serious infection group; (D) short and long-term infection group. CMV cytomegalovirus.
A total of 11 and 3 patients showed Epstein-Barr virus (EBV) DNAemia and EBV associated posttransplant lymphoproliferative disorders (PTLD) after COVID-19. The 150-day cumulative incidence of EBV DNAemia after COVID-19 was 7.4% (95% CI 3.0–11.8%) versus 0.00% (P = 0.068), respectively, between non-serious and serious infection group. The 150-day cumulative incidence of EBV DNAemia after COVID-19 was 5.6% (95% CI 0.8–10.4%) versus 5.6% (95% CI 0.8–10.4%) (P = 0.968), respectively, between short- and long-term infection group. All the 3 PTLD patients were in the non-serious group. No risk factors were associated with EBV DNAemia and PTLD in multivariable analysis.
The severity and duration of COVID-19 and mortality and survival
A total of 27 patients died after COVID-19, and the caused were summarized in Table 3. The most common cause was infection besides of COVID-19 (n = 9, 33.3%), followed by relapse (n = 7, 25.9%) and COVID-19 (n = 4, 14.8%).Table 3. Cause of death.Cause of deathn (%)Infection besides of COVID-199 (33.3)CMV pneumonia2 (7.4)CMV gastrointestinal disease1 (3.7)Klebsiella pneumoniae sepsis1 (3.7)Severe pneumonia of unknown etiology5 (18.5)Relapse7 (25.9)COVID-194 (14.8)Cerebrovascular disease4 (14.8)PGF1 (3.7)aGVHD1 (3.7)Arrhythmia1 (3.7)PGF poor graft function, CMV cytomegalovirus, aGVHD acute graft versus disease.
The 150-day cumulative incidence of non-relapse mortality (NRM) after COVID-19 infection was 11.2% (95% CI 6.6–15.8%), which was 2.2% (95% CI 0.3–4.7%) and 39.5% (95% CI 24.6–54.4%) between non-serious and serious infection group (P < 0.0001, Fig. 3A), and was 2.2% (95% CI 0.9–5.3%) and 20.0% (95% CI 11.7–28.3%) (P = 0.002, Fig. 3B) between short- and long-term infection group.Figure 3. The association between COVID-19 and survival. The 150-day cumulative incidence of NRM after COVID-19 between (A) non-serious and serious infection group; (B) short and long-term infection group. The 150-day probability of OS after COVID-19 infection between (C) non-serious and serious infection group; (D) short and long-term infection group. NRM non-relapse mortality, OS overall survival.
The 150-day probability of overall survival (OS) after COVID-19 infection was 84.9% (95% CI 79.6–90.2%), which was 94.9% (95% CI 91.2–98.6%) and 53.5% (95% CI 38.1–68.5%) between non-serious and serious infection group (P < 0.0001, Fig. 3C), and was 93.3% (95% CI 88.1–98.5%) and 76.7% (95% CI 67.9–85.5%) (P = 0.002, Fig. 3D) between short- and long-term infection group.
In multivariable analysis, after adjusted by other factors, the severity of COVID-19 was associated with NRM (HR, 17.26; 95% CI 4.87–61.21, P < 0.0001). The severity of COVID-19 were associated with OS (HR, 14.00; 95% CI 5.87–33.42, P < 0.0001) (Table 2), The other risk factors for NRM and OS were showed in Supplementary Table 4.
Clinical outcomes of patients with and without COVID 19 infection
A total of 179 patients without COVID-19 infection were enrolled as controlled and the characteristics between patients with and without COVID-19 were showed in Supplementary Table 5. The 150-day probability of NRM and OS were 11.2% (95% CI 6.6–15.8%) versus 3.9% (95% CI 1.1–6.7%) with P = 0.009 and 84.9% (95% CI 79.6–90.2%) versus 93.9% (95% CI: 88.7%–99.1%) with P = 0.006, respectively, for patients in the group with and without COVID-19 infection (Fig. 4A,B). The probability of NRM and OS for patients without COVID-19 infections were superior to those in serious infection group or long-term infection group (Fig. 4C,D).Figure 4. Clinical outcomes of patients with and without COVID 19 infection. (A) The 150-day cumulative incidence of NRM in the group with and without COVID-19 infection; (B) The 150-day cumulative incidence of OS in the group with and without COVID-19 infection; (C) The 150-day cumulative incidence of NRM in the group without COVID-19 infection, serious infection and long-term infection; (D) The 150-day cumulative incidence of OS in the group without COVID-19 infection, serious infection and long-term infection, NRM non-relapse mortality, OS overall survival.
Discussion
In the present study enrolled consecutive hospitalized COVID-19 patients, 24% of them showed serious infection, and more than half of the patients experienced long-term COVID-19 infection (i.e., more than 18 days). The 150-day cumulative incidence of PGF, leukopenia, CMV disease, CMV pneumonia, NRM, and OS after COVID-19 was significantly higher in long-term infection group compared with short-term infection group. In addition, the 150-day cumulative incidence of CMV disease, CMV pneumonia, NRM, and OS after COVID-19 was also significantly higher in serious infection group compared with non-serious infection group. Thus far, this is the first study identify the influence of severity and duration of SARS-CoV-2 infection on complications after allo-HSCT in the Omicron era.
Viral infection is one of the most important causes of PGF. Parvovirus B19 was the most common virus which can lead to rejection and PGF^24,25^. In addition, herpes virus could also induce PGF. For example, the association of HHV-6 infections and thrombocytopenia has been reported since 1990s^26^, and several studies observed the association between HHV-6 infections and delayed platelet engraftment in allo-HSCT recipients^27,28^. Some studies also reported that CMV infection was associated with thrombocytopenia^29^ and PGF^16^. The potential mechanism including impairment of virus on hematopoietic microenvironment or hematologic toxicities of anti-virus drugs. Herpes simplex virus and CMV can infect hematopoietic progenitor cells^30–32^, and the treatments of CMV such as gancilovir and forscarnet could lead to myelosuppression. Similarly, several studies also reported SARS-CoV-2 infection could cause anemia^33–35^, thrombocytopenia^34–36^, and aplastic anemia^37^. Thus, it is suggested that we should pay attention to PGF in patients with SARS-CoV-2 infection, particularly for those with long-term infection.
In addition, we observed that the incidence of CMV disease, particularly the CMV pneumonia, significantly increased in those with serious and/or long-term SARS-CoV-2 infection. Some data suggested that some viruses, such as HHV-6 and HHV-7, could take part in CMV reactivation or progression in immunosuppressed patients^38,39^. Lymphopenia is the hallmark of severe COVID-19 presentation, and previous studies observed that both the numbers of circulating T, B, and NK cells and antiviral cytokine production capability decreased in patients with COVID-19, particularly in those required intensive care^40–42^. Drylewicz et al.^43^ show that reconstitution of CD4^+^ T cells and NK cells after allo-HSCT is important for CMV prophylaxis. Thus, we speculated that COVID-19 infection may increase the susceptibility of CMV reactivation after allo-HSCT, which should be further confirmed in the future.
Previous studies have shown that the mortality rate range 12.5–22% in allo-HSCT recipients after COVID-19 infection^44–46^. While in the immunodeficient patients infected with Omicron variant, the mortality rate was 10.5% in the advanced malignancy cohort^23^. Our data suggested the 150-day cumulative incidence of NRM after COVID-19 infection was 11.2% in allo-HSCT recipients, which was similar to the previous studies. In addition, we only enrolled the hospitalized COVID-19 patients, which may also contribute to the relatively high NRM.
As mentioned above, long-term SARS-CoV-2 infection increased the risk of PGF, CMV disease, and NRM, this suggested that how to clear the SARS-CoV-2 timely is critical to improve the outcomes of these patients. Besides of the anti-viral drug (e.g., Nirmatrelvir/Ritonavir), the intense of immunosuppressive therapy could influence the viral clearance and was associated with severity and persistence of infection. Thus, allo-HSCT recipients may taper the immunosuppressive therapy after SARS-CoV-2 infection.
There were some limitations in the present study. This was a single center, observational cohort study and the followed-up was still relatively short, so we should further identify the long-term impact of Omicron variant infection on post-transplant complications in future.
In summary, we observed that the severity and duration of COVID-19 infection were associated with PGF, leukopenia, CMV disease, CMV pneumonia, NRM, and survival after allo-HSCT. Thus, how to prevent and clear the SARS-CoV-2 infection effectively is still critical for allo-HSCT recipients in the Omicron era.
Materials and methods
Patients
We performed an observational prospective study in Peking University, Institute of Hematology (PUIH, n = 179). Including criteria were as followed: 1) the hospitalized patients had received an allo-HSCT in PUIH at any time before the diagnosis of COVID-19, and 2) have laboratory-confirmed (polymerase chain reaction or antigenic test) COVID-19. In order to compare the clinical outcome between patients with and without COVID-19, a historical cohort included patients receiving allo-HSCT from August 1 2016 to December 1 2022 were enrolled and they were matched for age, sex, underlying disease, allo-HSCT time and time after allo-HSCT in a 1: 1 ratio. The study was approved by the Ethics Committee of Peking University People’s Hospital, and written informed consent was obtained from all subjects before study entry, in accordance with the Declaration of Helsinki.
Transplantation protocols
Donor selection, human leukocyte antigen typing, graft harvesting, conditioning regimen, GVHD, and infection prophylaxis were performed as previously described^1^. Comorbidities in HSCT recipients were assessed according to the hematopoietic cell transplantation–specific comorbidity index (HCT-CI).
Clinical definitions and assessments
During our study period, the Omicron variant was predominant in Beijing, China. The severity of COVID-19 was categorized as asymptomatic infection, mild, moderate, severe, and critical illness according to guidelines of National Institutes of Health (Supplementary methods). Severe illness and critical illness were classified as serious infection, and asymptomatic infection, mild illness and moderate illness were classified as non-serious infection in the present study. The duration of COVID-19 infection was defined as the time of the patients with persistent signs and symptoms with polymerase chain reaction or antigenic test positivity.
PGF was defined as the presence of 2 or 3 cytopenic counts (ANC ≤ 0.5 × 10^9^/L, platelet ≤ 20 × 10^9^/L, or hemoglobin ≤ 70 g/L) for at least 3 consecutive days beyond day 28 post-transplantation or dependence on transfusion and granulocyte colony-stimulating factor (G-CSF), in the presence of complete donor chimerism. Leukopenia was defined as ANC ≤ 0.5 × 10^9^/L alone for at least 3 consecutive days beyond day 28 post-transplantation or dependence on G-CSF, thrombocytopenia was defined as engraftment of peripheral blood cell lines (ANC > 0.5 × 10^9^/L and hemoglobin > 70 g/L without transfusion support) other than a platelet count < 20 × 10^9^/L or dependence on platelet transfusions for at least 7 consecutive days, in the presence of complete donor chimerism. Patients with evidence of hematological relapse post-HSCT were excluded. GVHD was diagnosed and graded based on international criteria^47^. CMV infection was diagnosed according to the definition of CMV Drug Development Forum^48^. PTLD was diagnosed according to the Sixth European Conference on Infections in Leukemia guidelines^49^.
Relapse was defined by morphologic evidence of disease in peripheral blood, bone marrow, or extramedullary site samples or by the recurrence and sustained presence of pre-transplantation chromosomal abnormalities. NRM was defined as death without disease progression or relapse. OS was defined as the time from transplantation to death from any cause.
Statistical analysis
Characteristics of patients were summarized by descriptive statistics, that is, using counts and percentages for categorical variables and using median and range for continuous variables. Subject variables were compared using the χ^2^ test for categorical variables and the Mann–Whitney U test for continuous variables. Multivariate analyses were performed using the Cox proportional hazards model for survival to identify the independent prognostic variables (Supplementary methods). The parameters with P < 0.10 according to the univariate analysis were entered into a multivariate model (Supplementary Table 3). Cumulative incidence curves were used in a competing risk setting, with relapse treated as a competing event, to calculate NRM probabilities, and with death and relapse as the competing risks for PGF, infection, and GVHD. The probability of survival was estimated with the Kaplan–Meier method and were compared using the log-rank test. Statistical analyses were performed using 1-way analysis of variance (ANOVA) for comparisons among the groups. Analyses were performed using GraphPad Prism 6.0 (GraphPad Software), SPSS 24 (SPSS Inc./IBM, Armonk, NY, USA) and R version 3.4.4 (The R Foundation for Statistical Computing). Unless otherwise specified, all P values were 2-sided and P < 0.05 was considered significant.
Supplementary Information
Supplementary Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Xu LP The consensus on indications, conditioning regimen, and donor selection of allogeneic hematopoietic cell transplantation for hematological diseases in China-recommendations from the Chinese Society of Hematology J. Hematol. Oncol.2018113310.1186/s 13045-018-0564-x 29495966 PMC 5833104 · doi ↗ · pubmed ↗
- 2Lv M Shen MZ Mo XD Development of allogeneic hematopoietic stem cell transplantation in 2022: Regenerating "Groot" to heal the world Innovation 2023410037310.1016/j.xinn.2023.10037336794169 PMC 9923186 · doi ↗ · pubmed ↗
- 3Arnaout K Complications of allogeneic hematopoietic stem cell transplantation Cancer Invest.20143234936210.3109/07357907.2014.91930124902046 · doi ↗ · pubmed ↗
- 4Pei XY Comparable anti-CMV responses of transplant donor and third-party CMV-specific T cells for treatment of CMV infection after allogeneic stem cell transplantation Cell. Mol. Immunol.20221948249110.1038/s 41423-021-00829-y 35017718 PMC 8975930 · doi ↗ · pubmed ↗
- 5Chakraborty I Maity PCOVID-19 outbreak: Migration, effects on society, global environment and prevention Sci. Total Environ.202072813888210.1016/j.scitotenv.2020.13888232335410 PMC 7175860 · doi ↗ · pubmed ↗
- 6Liu Y Rocklöv J The effective reproductive number of the Omicron variant of SARS-Co V-2 is several times relative to Delta J. Travel Med.20222903710.1093/jtm/taac 037PMC 899223135262737 · doi ↗ · pubmed ↗
- 7Busca A Outcome of COVID-19 in allogeneic stem cell transplant recipients: Results from the EPICOVIDEHA registry Front. Immunol.202314112503010.3389/fimmu.2023.112503036911708 PMC 9999728 · doi ↗ · pubmed ↗
- 8Shahzad M Impact of COVID-19 in hematopoietic stem cell transplant recipients: A systematic review and meta-analysis Transpl. Infect. Dis.202224 e 1379210.1111/tid.1379235030267 · doi ↗ · pubmed ↗