Cardiac myxoma and cerebral vasculitis: Is there a link?
Samah El-Mhadi, Belghait El Hajjaj, Asmae Benatmane, Mariam El Harrak, Sara Ahchouch, Abderrahim Elktaibi, Fouad Nya, Najat Mouine, Aatif Benyass

TL;DR
This paper presents a case where a cardiac myxoma caused neurological symptoms, highlighting the importance of early diagnosis to prevent complications.
Contribution
The novelty lies in reporting a rare neurological presentation of cardiac myxoma, emphasizing diagnostic challenges.
Findings
A cardiac myxoma was diagnosed in a patient presenting with neurological symptoms like sudden leg weakness and slurred speech.
Imaging and echocardiography confirmed a left atrial myxoma extending into the left ventricle.
Successful surgical removal and histopathological confirmation led to an uneventful recovery.
Abstract
Cardiac myxomas present a diagnostic challenge due to their ability to mimic various cardiovascular and systemic conditions. Timely identification is crucial for implementing surgical intervention and averting life-threatening complications. We reported the case of a 49-year-old male patient who presented sudden legs weakness and slurred speech and was admitted 10 h later in emergency department. Physical examination was significant for paraparesis and paraphasia. Cardiac and carotid auscultation was normal. CT brain revealed multiple acute ischemic strokes and MRA was suggestive of cerebral vasculitis. As pre-therapy assessment, the EKG revealed no electrical abnormalities and the chest X-ray showed signs of left atrial enlargement. Transthoracic and transesophageal echocardiography showed a left atrial mass attached to the interatrial septum, measuring 9*5*4 cm and extending into the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
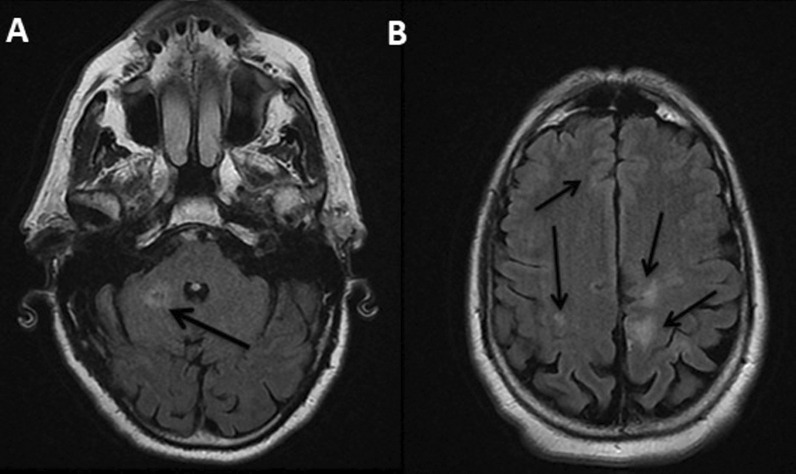 Figure 1
Figure 1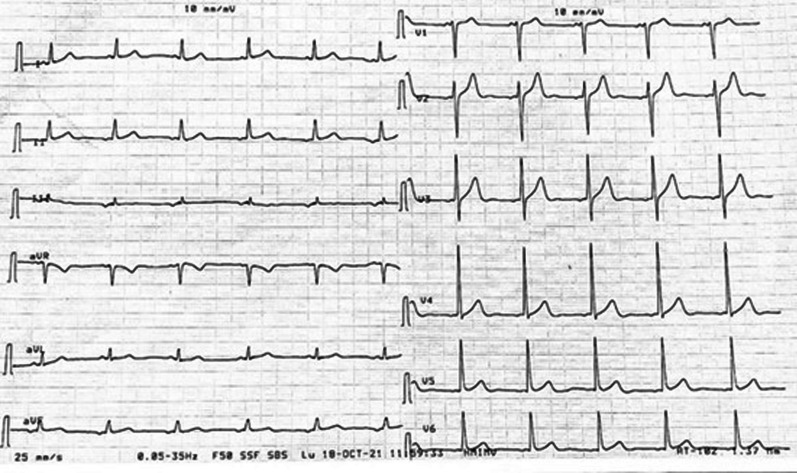 Figure 2
Figure 2 Figure 3
Figure 3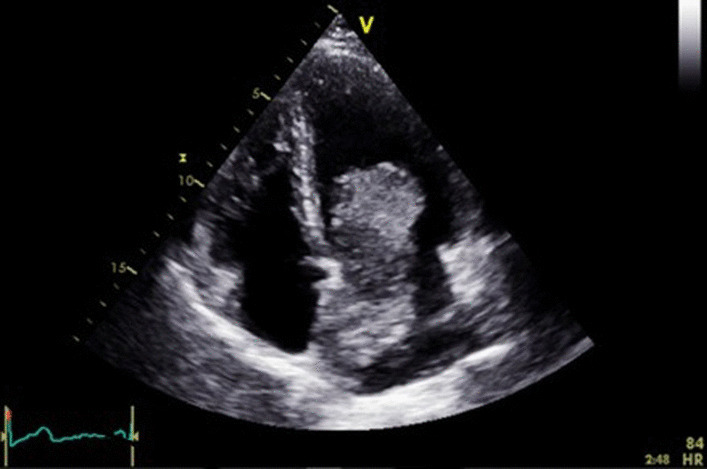 Figure 4
Figure 4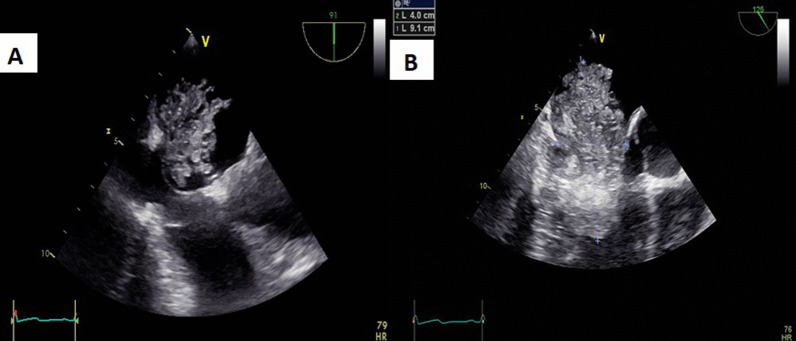 Figure 5
Figure 5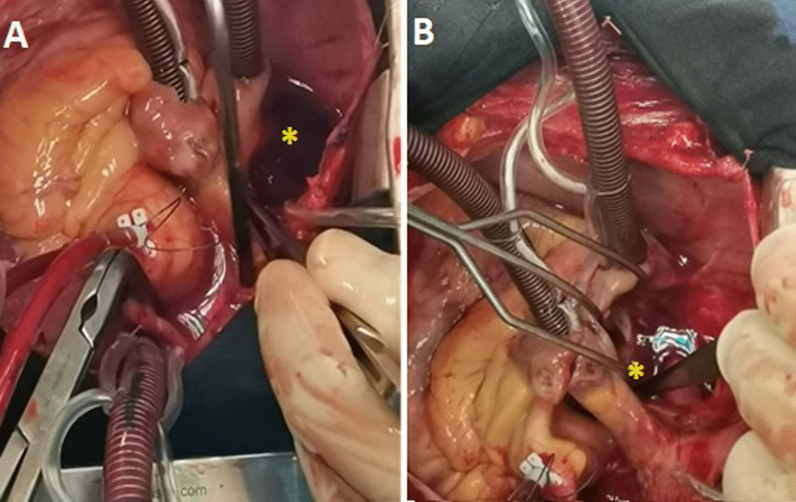 Figure 6
Figure 6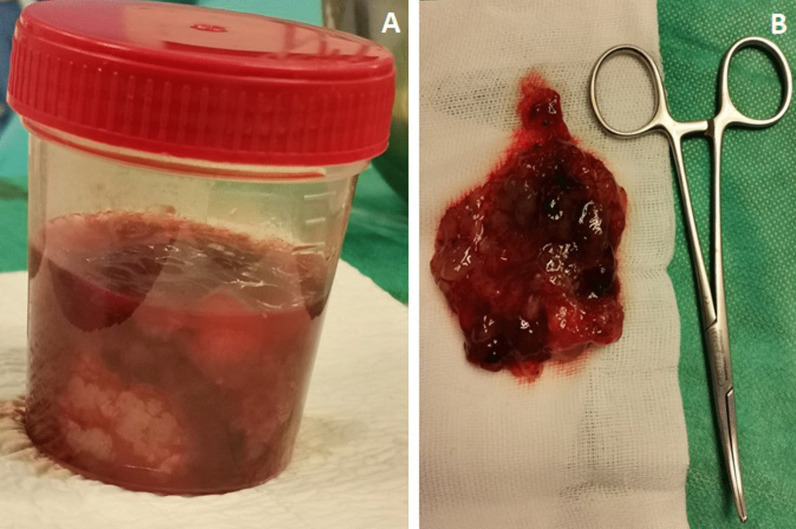 Figure 7
Figure 7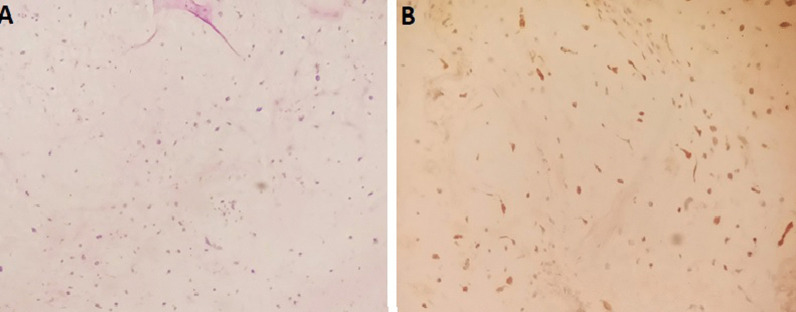 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Coronary Artery Anomalies · Cardiac Structural Anomalies and Repair
Background
Cardiac myxomas present a considerable diagnostic challenge in medical practice. These tumors, primarily originating from the endocardium, can masquerade as various cardiovascular and systemic conditions, complicating their timely diagnosis and management [1]. Literature underscores the importance of a high index of suspicion for cardiac myxomas, particularly in patients with unexplained cardiac or systemic symptoms, in order to provide surgical treatment and prevent life-threatening complications [1].
Case presentation
We reported the case of a 49-year-old male patient with no cardiovascular risk factors or medical history, who experienced sudden onset of leg weakness and slurred speech. He presented to the emergency department 10 h later, with a heart rate of 100 bpm and blood pressure of 130/85 mmHg in both arms. Physical examination revealed paraparesis and paraphasia. Cardiac and carotid auscultation was normal.
CT brain showed multiple acute ischemic strokes. MRA revealed frontal, occipital and cerebellar white matter signal abnormalities suggestive of cerebral vasculitis (Fig. 1). The patient was subsequently transferred to the internal medicine department for further investigations and vasculitis treatment.Fig. 1A + B Axial views of brain MRI showing frontal, occipital and cerebellar white matter signal abnormalities
Pre-therapy assessments included an EKG which revealed a coronary sinus rhythm without electrical abnormalities (Fig. 2), a chest X-ray which showed cardiomegaly with a double density sign and splaying of the carina indicative of left atrial enlargement (Fig. 3), and a transthoracic echocardiography (TTE) which revealed a mobile and heterogeneous mass measuring 954 cm in the left atrium, extending into the left ventricular cavity during diastole without significant inflow obstruction across the mitral valve (Fig. 4). Transesophageal echocardiography (TOE) confirmed that the mass was attached to the interatrial septum at the site of the fossa ovalis, consistent with a diagnosis of left atrial myxoma (Fig. 5).Fig. 2EKG showing coronary sinus rythmFig. 3Chest X-ray showing signs of left atrial enlargementFig. 4Cine four-chamber view of TTE revealing a huge left atrial myxomaFig. 5A + B Cine views of TOE showing the dimensions of myxoma and its attachment to the interatrial septum
The patient underwent preoperative supra-aortic trunk echo-Doppler and coronary calcium scan which were unremarkable.
Laboratory examinations revealed microcytic and hypochromic anemia (hemoglobin: 10 g/dL) and elevated inflammatory biomarkers (C-reactive protein: 39 mg/L, ferritinemia: 520 ng/mL), with no hydro-electrolyte disorder and normal liver and kidney functions. Serological tests for syphilis, HIV, VHB and VHC and autoimmune screening were negative.
The patient underwent open-heart surgery. An aorto-bicaval cannulation and a cardiopulmonary bypass were established. After left atriotomy, a giant tumor arising from the interatrial septum was resected, with cauterization of its implantation base in order to prevent local recurrence. The left atrium was closed, and the aortic cross-clamp was removed. The surgical intervention lasted 50 min (Fig. 6).Fig. 6A + B Intraoperative photographs showing the left atrial myxoma (*)
Macroscopically, the excised mass measured 944 cm and was soft-mulberry-shaped and friable, with gelatinous consistency and punctate hemorrhage on the outer surface (Fig. 7). Histopathological examination showed marked loose myxoid stroma with scattered spindle cells, but no mitotic figures or malignant features, confirming the diagnosis of myxoma (Fig. 8).Fig. 7A + B Macroscopical aspects of the resected specimenFig. 8A Low Power View of atrial myxoma showing the tumor cells within a myxoid stroma (Haematoxylin and Eosin stained sections); B Calretinin Immunoreactivity shown in myxoma’s cells
Postoperative TOE did not reveal an interatrial shunt. The patient was monitored in the ICU for 24 h. The postoperative period was uneventful. He was discharged home with long-term echocardiographic follow-up recommended. The patient reported complete neurological recovery one month later.
Discussion
Primary cardiac tumors are rare entities in medicine, with studies indicating an incidence ranging from 0.001% to 0.3% in non-selected populations.
Three-quarters of these tumors are benign, and 30% of benign cardiac tumors are represented by myxomas [2].
Myxomas are typically diagnosed between the ages of 30 and 60 years. They mostly develop in the left atrium, specifically from the interatrial septum at the fossa ovalis, compared to right atrial and ventricular locations [2].
Clinical features of cardiac myxomas are determined by their size, location, consistency, and mobility. Constitutional symptoms attributed to myxomas, such as fever, weight loss, and arthralgia, suggest systemic inflammatory responses that could extend to the vascular endothelium [3].
The understanding of cardiac myxomas extends beyond their local impact within the heart, with emerging considerations for systemic manifestations, including their potential association with cerebral vasculitis [4].
Studies have highlighted that cardiac myxomas can lead to ischemic acute cerebral strokes through embolic phenomena, either from thrombi formation on the tumor’s surface or by detachment of tumor fragments into the systemic circulation. These emboli may result in cerebral infarctions, and there is growing interest in whether myxomas could also trigger inflammatory responses affecting cerebral blood vessels, resembling aspects of vasculitis [5].
Diagnosing cardiac myxomas can be challenging. TTE is the primary imaging modality due to its high sensitivity, allowing the assessment of the tumor’s characteristics (morphology, size, mobility, and attachment site). Doppler evaluation assesses the hemodynamic consequences of the mass. Complementary TOE provides a more detailed evaluation, and cardiac MRI can be useful in establishing a differential diagnosis with other cardiac masses [5].
Currently, there is no effective medical treatment to stop myxomas growth, and surgical removal is necessary to prevent life-threatening complications [6].
The timing of surgery is controversial in patients with recent neurological ischemic injuries, due to the risk of bleeding conversion during cardiopulmonary bypass [7].
Surgical resection is optimized by inducing cardioplegic arrest to provide a motionless operative field and realize a piecemeal removal. Aortic cross-clamping helps minimize perioperative tumor dislodgement and massive embolization, particularly with papillary and friable myxomas.
The usual approach is via left atrial incision, posterior to interatrial groove to explore the tumor. In cases of giant myxomas or restricted left atrial access, the approach can be via right atriotomy. There is controversy regarding radical resection with excision of a full-thickness portion of the interatrial septum versus conservative excision, especially with sporadic myxomas [8].
Surgical excision has an excellent long-term prognosis. The overall risk of recurrence is 22% for Carney complex myxomas, 12% for familial myxomas, and only 1% to 3% for sporadic cases [9].
Although surgical resection is curative with a low recurrence rate, patients should undergo regular follow-up with serial TTE [10].
Conclusion
We presented an interesting case featuring an uncommon and misleading neurological presentation of cardiac myxoma.
This case underscores the critical need for heightened clinical suspicion and thorough diagnostic evaluation to achieve early recognition among a broad range of differential diagnoses.
Recognizing and promptly treating cardiac myxomas is imperative to prevent life-threatening complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Griborio-Guzman AG Aseyev OI Shah H Sadreddini M Cardiac myxomas: clinical presentation, diagnosis and management Heart 20221081182783310.1136/heartjnl-2021-31947934493547 · doi ↗ · pubmed ↗
- 2Yuan SM Yan SL Wu N Unusual aspects of cardiac myxoma Anatol J Cardiol 20171732412472832110910.14744/Anatol J Cardiol.2017.7557 PMC 5864986 · doi ↗ · pubmed ↗
- 3Fabijanic D CarevićV BečićT Pešutić-Pisac V Cardiac myxoma: benign, but deadly disease Med Ultrason 202224224824910.11152/mu-367835617612 · doi ↗ · pubmed ↗
- 4Yuan SM Humuruola G Stroke of a cardiac myxoma origin Rev Bras Cir Cardiovasc 20153022252342610745510.5935/1678-9741.20150022 PMC 4462969 · doi ↗ · pubmed ↗
- 5Grebenc ML Rosado-de-Christenson ML Green CE Burke AP Galvin JR Cardiac myxoma: imaging features in 83 patients Radiographics 200222367368910.1148/radiographics.22.3.g 02ma 0267312006696 · doi ↗ · pubmed ↗
- 6Samanidis G Khoury M Balanika M Perrea DN Current challenges in the diagnosis and treatment of cardiac myxoma Kardiol Pol 202078426927710.33963/KP.1525432207702 · doi ↗ · pubmed ↗
- 7Schaff HV Mullany CJ Surgery for cardiac myxomas Semin Thorac Cardiovasc Surg 2000122778810.1053/ct.2000.507910807430 · doi ↗ · pubmed ↗
- 8Gür AK AykaçMC Surgical treatment of cardiac myxomas: a 23-case experience Heart Surg Forum 2018215 E 370E 37410.1532/hsf.198730311887 · doi ↗ · pubmed ↗