Navigating Diagnostic Uncertainty: Frontal Fibrosing Alopecia Versus Keratosis Pilaris Atrophicans Faciei With Genetic Testing Insights
Deesha D Desai, Ambika Nohria, Jerry Shapiro, Kristen I Lo Sicco

TL;DR
This paper discusses the diagnostic challenges between two skin conditions and explores how genetic testing can help improve accuracy.
Contribution
The paper presents a case study highlighting the potential of genetic testing in distinguishing similar skin conditions.
Findings
The case study involved a 36-year-old male with symptoms of both KPAF and FFA.
Genetic testing was used, though it tested negative for the mutation in question.
The study suggests genetic testing could enhance diagnostic accuracy and treatment outcomes.
Abstract
Keratosis pilaris atrophicans faciei (KPAF) and frontal fibrosing alopecia (FFA) present diagnostic challenges due to their similar clinical characteristics. Dermatologists often employ overlapping treatment regimens, which may hinder accurate diagnosis and treatment expectations. Genetic testing offers promise for precise diagnosis and tailored treatment strategies, yet its utility in these conditions remains underexplored. This manuscript presents a unique case study of a 36-year-old male with symptoms of both KPAF and FFA, who underwent genetic testing. Despite testing negative for this mutation, the case underscores the potential of genetic testing to enhance diagnostic accuracy and optimize treatment outcomes.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
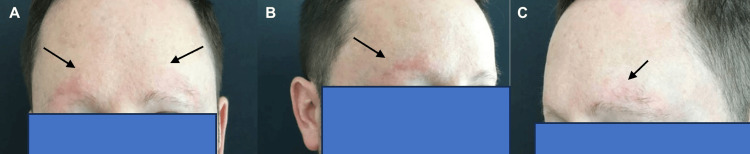 Figure 1
Figure 1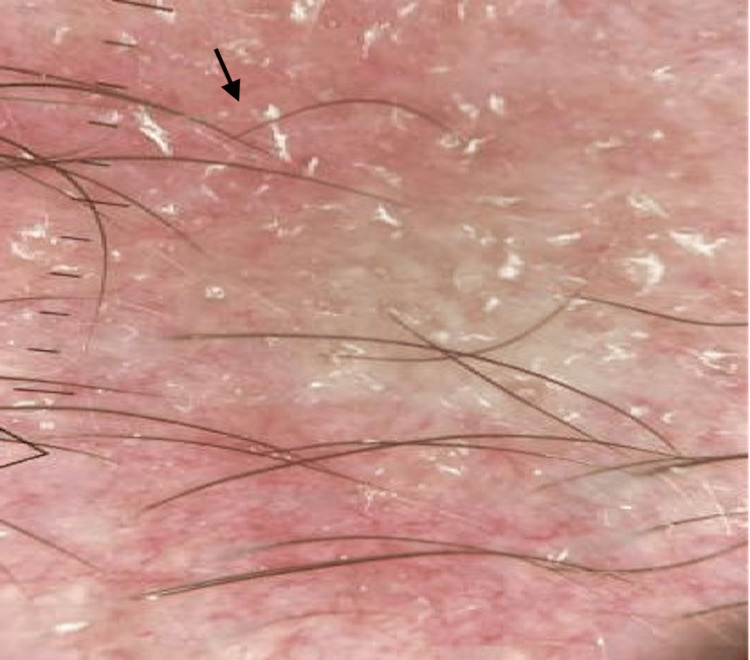 Figure 2
Figure 2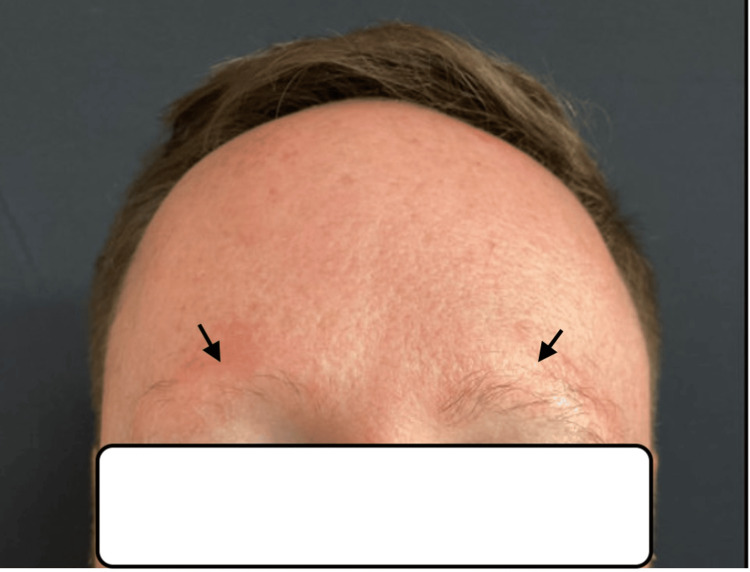 Figure 3
Figure 3| Keratosis Pilaris Atrophicans Faciei | Frontal Fibrosing Alopecia | |
| Cause | Abnormal keratinization of follicular infundibulum and/or autosomal dominant/recessive inheritance described with specific genetic markers | Unknown, though considered autoimmune |
| Onset | Infancy or childhood | Older adults, more common in women |
| Clinical Characteristics | Permanent loss of lateral margins of eyebrows, widespread keratosis pilaris on limbs and trunk and facial follicular papules (erythematous) | Receding frontal hairline, loss of eyebrows, perifollicular erythema and hyperkeratosis and facial follicular papules (flesh-colored) |
| Histopathology | Superficial perivascular lymphocytic infiltrate | Lymphocytic infiltrate around isthmus and infundibulum, replaced by fibrosis |
| Eyebrow Findings [ | Grouped keratotic follicular papules, perifollicular erythema along eyebrows, absence of follicular ostia, presence of telangiectasias, yellow dots and dystrophic hair | Yellow dots, multiple pinpoint dots, short thin hairs (vellus), black dots, tapered and broken hair and dystrophic hairs |
| Genetics [ |
|
|
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatological and Skeletal Disorders · Genetic and rare skin diseases. · Dermatologic Treatments and Research
Introduction
Keratosis pilaris atrophicans faciei (KPAF) and frontal fibrosing alopecia (FFA) share similar clinical characteristics, presenting challenges in diagnosis. Both conditions may manifest features such as bilateral eyebrow loss and facial follicular papules, often accompanied by lymphocytic infiltrates observed in histopathology [1,2]. Dermatologists frequently employ overlapping treatment regimens in an attempt to manage both conditions simultaneously. However, this approach may lack clarity in diagnosis for patients, could result in unnecessary treatments based on the underlying condition, and prohibit providing appropriate treatment expectations. Genetic testing holds promise for precise diagnosis and enables more tailored treatment strategies. Despite this potential, previous studies have not explored cases comparing these conditions in clinical settings or the utility of genetic testing for diagnosis. Herein, we introduce a unique case study of a patient displaying symptoms of both conditions, who underwent genetic testing to uncover insights into the underlying pathology.
Case presentation
A 36-year-old male initially sought consultation at the dermatology clinic for a two-year history of hair loss, primarily affecting his eyebrows. The loss had progressed to near-complete absence at the time of consultation. He denied any concurrent loss of scalp hair, eyelash, or beard hair loss, as well as associated symptoms such as itching, pain, burning sensation, or excessive shedding. Despite using topical ruxolitinib 1.5% cream once daily for three months, there was no improvement noted. Physical examination revealed nearly complete bilateral eyebrow loss with dermatoscopic signs of erythema, telangiectasias, and scaling (Figures 1A-1C, 2). A left lateral eyebrow punch biopsy revealed sparse superficial perivascular lymphocytic infiltrate, rare eosinophils, and focal interface changes. Given the suspicion of FFA, Lichen planopilaris (LPP), or KPAF, treatment commenced with medications overlapping for all conditions: tacrolimus 0.1% topical ointment once daily, tretinoin 0.01% gel once daily, and oral minoxidil 2.5mg once daily.
(A-C) Bilateral eyebrow loss with background erythema
Left lateral eyebrow dermatoscopy demonstrating follicular dropout with background scaling, erythema, and telangiectasias
At the follow-up visit six months later, the patient reported mild regrowth of his eyebrows and new-onset irritation at the mid-frontal hairline. Physical examination revealed increased density in the left eyebrow with persistent erythema but no visible scaling (Figure 3). Thin, scattered perifollicular scaling was observed at the frontal hairline, along with flesh-colored forehead papules. Considering these developments, genetic testing was recommended, specifically targeting the Desmoglein - 4 (DSG-4) mutation. However, the patient tested negative for this specific mutation.
Bilateral eyebrows at the follow-up visit, left > right density
Discussion
KPAF is theorized to stem from aberrant keratinization within the follicular infundibulum [3]. This process results in the accumulation of scale within the follicle, obstructing the hair shaft and inciting inflammation. Over time, this chronic inflammation culminates in permanent atrophy that is highlighted by signs of telangiectasias that can be seen in trichoscopy of the eyebrows [3]. However, both autosomal dominant and recessive inheritance patterns have been described with specific genetic markers, notably DSG-4, implicated [4]. This condition typically manifests in infancy or childhood and is marked by the presence of facial follicular erythematous papules, permanent loss of lateral margins of bilateral eyebrows, and potentially widespread keratosis pilaris on the limbs and trunk.
In contrast, FFA is believed to have an autoimmune etiology, primarily affecting older adults, notably post-menopausal women. FFA shares similar clinical features with KPAF, including bilateral eyebrow loss (madarosis), perifollicular erythema, follicular hyperkeratosis (noted in the frontal hairline rather than eyebrows), and facial follicular flesh-colored papules, but it is differentiated by a receding frontal hairline (Table 1) [5].
These two conditions share clinical overlap. Moreover, the histopathological characteristics of KPAF demonstrate superficial perivascular lymphocytic infiltrate and FFA exhibits lymphocytic infiltrate around the isthmus and infundibulum, eventually replaced by fibrosis. The lymphocytic nature of both conditions adds complexity to their differentiation. Given these similarities, the pivotal question revolves around identifying techniques that can effectively guide therapeutic decisions for these complex conditions.
In light of these challenges, exploring techniques such as genetic testing may offer insights into accurate diagnosis and guide therapeutic decisions. Specific genetic mutations, particularly in genes like DSG-4, LDL receptor-related protein (LRP-1 gene), membrane-bound transcription factor protease 2 (MBTPS-2 gene), and chromosome 18p arm, have been implicated in KPAF's underlying pathology [9,10]. Genetic testing can provide diagnostic clarity, preventing unnecessary treatments based on the true underlying condition and facilitating tailored treatment strategies. In this context, we present a case where genetic testing was utilized in patient care in the hopes of underscoring the potential of this approach. Nonetheless, further studies are imperative to navigate therapeutic decisions effectively in the face of these challenging conditions.
Conclusions
In conclusion, this case study highlights the intricate diagnostic and therapeutic challenges posed by the clinical overlap between KPAF and FFA. Despite their distinct etiologies, both conditions present notable similarities in clinical presentation and histopathological features, often complicating accurate diagnosis and treatment selection. The case serves as a poignant reminder of the imperative to explore innovative diagnostic modalities, such as genetic testing, to potentially unravel the underlying genetic basis and guide tailored therapeutic interventions. While the patient yielded negative for the specific DSG-4 mutation associated with KPAF, the utilization of genetic testing exemplifies a promising avenue for enhancing diagnostic precision and optimizing treatment outcomes in complex dermatological conditions. Nevertheless, further research endeavors are warranted to elucidate the utility and efficacy of genetic testing in navigating therapeutic decisions amidst the intricate clinical landscape of KPAF and FFA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Keratosis pilaris atrophicans faciei: an observational, descriptive, retrospective clinical study Exp Ther Med Fekete GL Fekete L Neagu N Bacârea V Drăgănescu M Brihan I 13312220213463068510.3892/etm.2021.10766 PMC 8495552 · doi ↗ · pubmed ↗
- 2Lichen planopilaris and frontal fibrosing alopecia: review and update of diagnostic and therapeutic features An Bras Dermatol Fechine CO Valente NY Romiti R 3483579720223537950810.1016/j.abd.2021.08.008PMC 9133245 · doi ↗ · pubmed ↗
- 3Keratosis pilaris atrophicans: case series and review Pediatr Dermatol Callaway SR Lesher JL Jr 14172120041487131910.1111/j.0736-8046.2004.21103.x · doi ↗ · pubmed ↗
- 4Desmoglein 4 mutation underlies autosomal recessive keratosis pilaris atrophicans Acta Derm Venereol Cohen-Barak E Danial-Farran N Hammad H 8098109820182979669010.2340/00015555-2976 · doi ↗ · pubmed ↗
- 5Frontal fibrosing alopecia Clin Dermatol Kerkemeyer KL Eisman S Bhoyrul B Pinczewski J Sinclair RD 1831933920213427200710.1016/j.clindermatol.2020.10.007 · doi ↗ · pubmed ↗
- 6Trichoscopy findings of frontal fibrosing alopecia on the eyebrows: a study of 151 cases J Am Acad Dermatol Anzai A Pirmez R Vincenzi C Fabbrocini G Romiti R Tosti A 113011348520213185710810.1016/j.jaad.2019.12.023 · doi ↗ · pubmed ↗
- 7The role of trichoscopy in keratosis follicularis spinulosa decalvans: case report and review of the literature Skin Appendage Disord Alessandrini A Brattoli G Piraccini BM Di Altobrando A Starace M 2935720213361471610.1159/000510525 PMC 7879284 · doi ↗ · pubmed ↗
- 8Genome-wide association study in frontal fibrosing alopecia identifies four susceptibility loci including HLA-B*07:02Nature Commun Tziotzios C Petridis C Dand N 11501020193085064610.1038/s 41467-019-09117-w PMC 6408457 · doi ↗ · pubmed ↗