Synergistic Manifestations in Cardiac Cysticercosis Complicated by Snake Bite: A Case Report and Literature Review
Raviprakash Meshram, Vikas Vaibhav, Yashpal S, Ashok Singh, Shailesh Parate, Gitanjali Khorwal, Kshitiza Sharma, Rahul Sharma

TL;DR
A young man with asymptomatic heart cysticercosis died after a snake bite, highlighting the need to consider multiple causes in tropical medical cases.
Contribution
This case report highlights the rare co-occurrence of asymptomatic cardiac cysticercosis and fatal snakebite.
Findings
Autopsy revealed cardiac cysticercosis with cystic nodules in the myocardium.
The patient had asymptomatic disseminated cysticercosis despite multiple organ involvement.
The cause of death was attributed to complications from the snakebite, not the cysticercosis.
Abstract
Cysticercosis presents a prevalent issue on a global scale. Nevertheless, disseminated cysticercosis (DCC) is infrequent; even rarer is asymptomatic DCC. Here, we present a unique case of asymptomatic DCC involving the heart in a young male who came to medical attention following a fatal snake bite, ultimately leading to his demise. Despite the widespread dissemination of cysticercosis affecting multiple organs, the individual remained asymptomatic for the condition. We present a case of a 23-year-old male who was brought to the emergency department with a history of alleged snake bites. The patient was declared dead upon arrival at the All India Institute of Medical Sciences (AIIMS), Rishikesh, India. Autopsy findings revealed multiple significant cardiac abnormalities, including atheromatous changes with calcification in the root of the aorta and aortic valve, along with numerous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
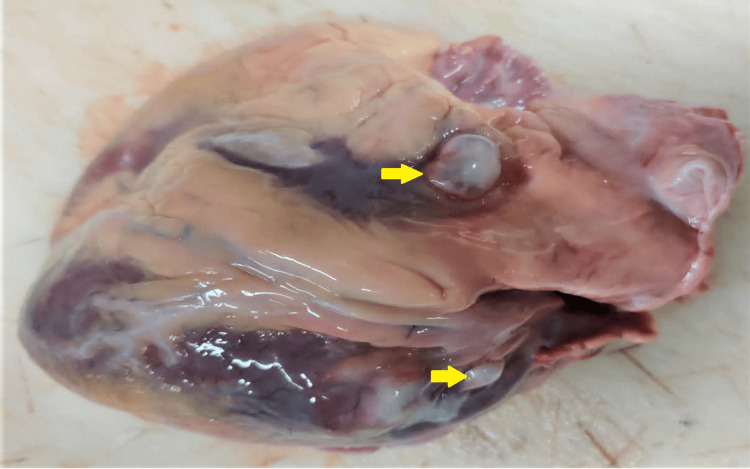 Figure 1
Figure 1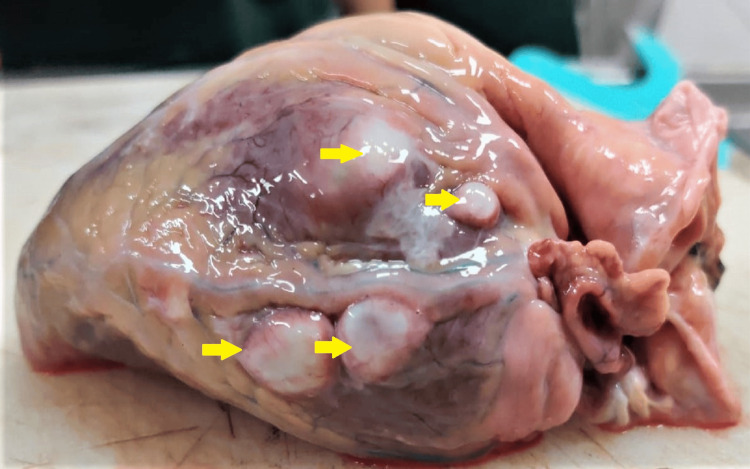 Figure 2
Figure 2 Figure 3
Figure 3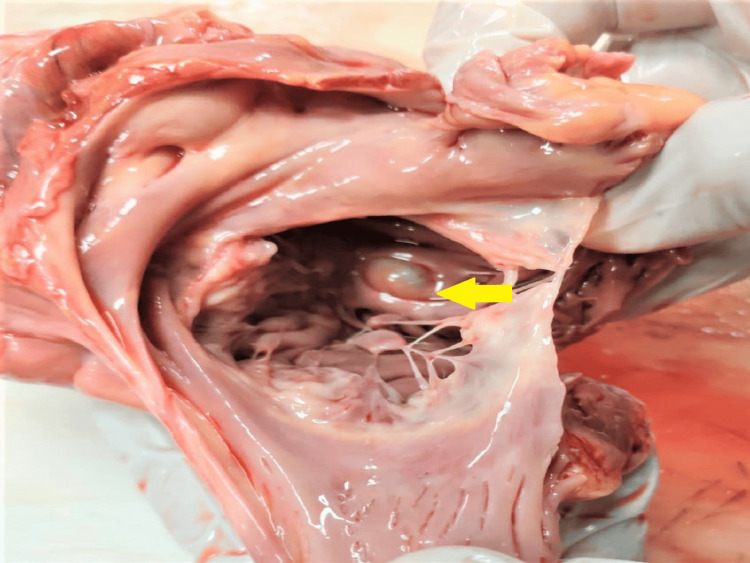 Figure 4
Figure 4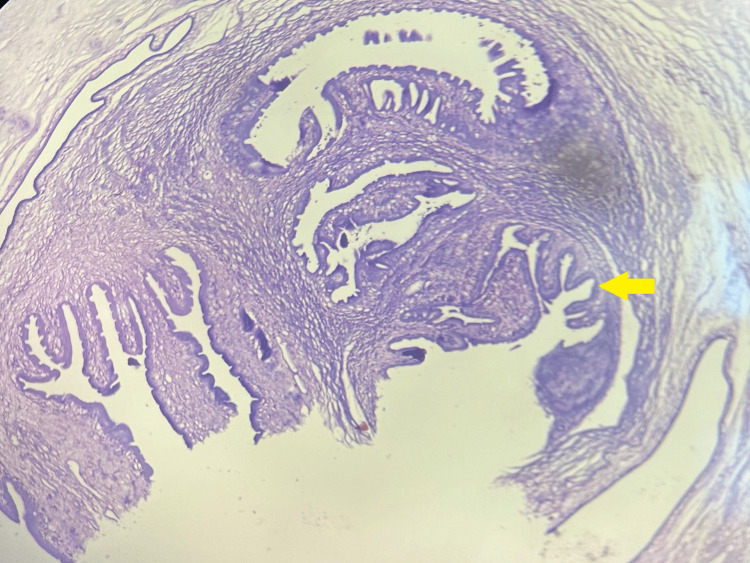 Figure 5
Figure 5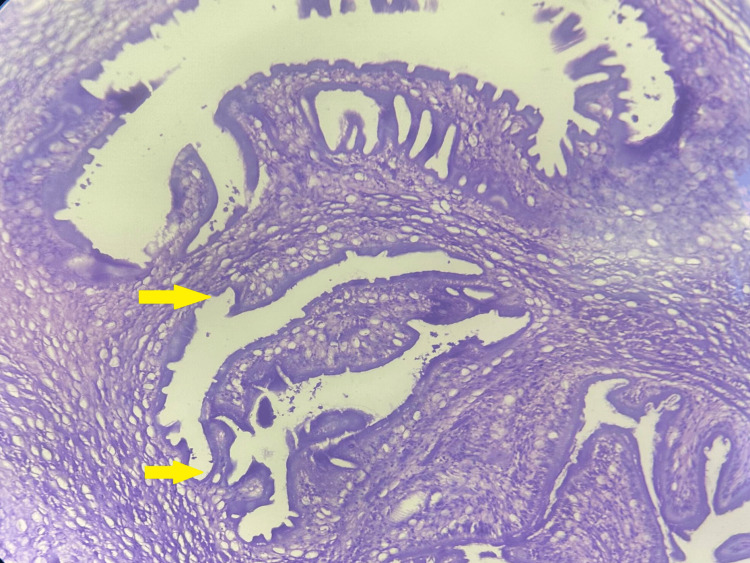 Figure 6
Figure 6| References | Case report location | Patient | Presentation | Site of disease |
| Prabhakar et al. [ | India | Male | Cyst invading the interventricular septum and papillary muscles, leading to ventricular arrhythmia and branch block | Heart |
| Jain et al. [ | Mumbai, India | 19-year-old male | Headache and vomiting, seizures, decreased vision, and bilateral proptosis | Heart, brain, extradural spinal space, muscles, lungs, pancreas, and eyes |
| Gill et al. [ | Rohtak, India | 30-year-old female | One or few cysts over the myocardium | Heart |
| Vaidya et al. [ | New Delhi, India | 27-year-old male | Multiple subcutaneous nodules all over the patient’s body | Heart, brain, face, orbit, lungs, pancreas, and spleen |
| Khandpur et al. [ | New Delhi, India | 48-year-old male | Innumerable soft to firm, deep-seated asymptomatic nodular swellings over the trunk and extremities | Heart, skin, central nervous system, skeletal muscles, eyes, and lungs |
| Dsilva et al. [ | Mumbai, India | 62-year-old male | Episodes of generalized tonic–clonic seizures and multiple subcutaneous nodules over both calves, arms, and nape of the neck | Heart, brain, subcutaneous tissue, liver, and muscles |
| Sanjay et al. [ | Rohtak, India | 40-year-old male | Unknown | Heart |
| Littlewood [ | UK | 38-year-old male | Chest pain and ECG changes suggestive of an ST-elevation myocardial infarction | |
| Bastos et al. [ | Brazil | 39-year-old male | Dyspnea, physical examination showed multiple subcutaneous nodules, which were predominant in the arms and thorax | Multiple ring-like enhancing brain, hypodense nodules present in heart musculature |
| Nery et al. [ | Brazil | 59-year-old man | Symptoms of typical angina 6 hours in duration | Cystic lesion on the myocardium |
| Himwaze et al. [ | Lusaka, Zambia | 8 cases, all were male, aged in b/w 28-56 years | Heart, central nervous system, kidney, lung, muscles, and omentum | |
| Lima et al. [ | Michigan, USA | 54-year-old male | Suspected appendicitis; however, a cecal tumor was found | Brain and heart |
| Spina et al. [ | Sydney, Australia | 24-year-old woman | Having intermittent frontal headaches, high fever, sweats, arthralgias, nausea, vomiting, and weight loss of about 6 kg in one month | Heart and brain |
| Melo et al. [ | Brazil | 46-year-old female | Exertional dyspnea, palpitations, peripheral edema, ascites, and hepatomegaly | Heart and brain |
| Thomas et al. [ | South Africa | 42-year-old male | Lightheadedness, bradycardia, and felt dizzy on getting up supine | Heart, brain, muscles, and subcutaneous tissues |
| Niakara et al. [ | Burkina Faso, West Africa | 37-year-old male | Seizures and bradycardia | Heart, brain, and skin |
| Sun et al. [ | China | 33-year-old male | Headache, nausea, vomiting, and bradycardia | Heart, skin, and brain |
| Dediunina et al. [ | Russia | 30-year-old female | Symptomatic bradycardia | Heart and brain |
| Farina et al. [ | USA | 33-year-old female | Undergoing cardiac surgery | Heart, inferior vena cava, skin, muscle, liver, brain, and larynx |
| Blandón et al. [ | Panama | 50-year-old male | New York Heart Association stage IV heart failure | Heart and brain |
| Mauad et al. [ | Brazil | 53-year-old female | Cardiogenic shock and acute myeloid leukemia | Heart, lungs, brain, musculature, and skin |
| Bhalla et al. [ | India | 35-year-old female | Generalized seizures, proptosis of the right eye, and bilateral calf hypertrophy | Heart, skin, brain, eyes, and musculature |
| Goldsmid et al. [ | Cambridge University, Cambridge, UK | Case 1 | Died from head trauma. One cyst was found in the autopsy of the myocardium. | Heart |
| Case 2 | Died from cirrhosis. In the autopsy, 43 cysts were found in the heart. | Heart | ||
| Sun et al. [ | Beijing, China | 21-year-old | Patient with complete atrioventricular block, with subcutaneous and cerebral cysticercosis diagnosis. | Heart and brain |
| Cutrone et al. [ | Unkown | Man with chest pain and multivessel coronary disease. Ultrafast computed tomography showed multiple cysts in the myocardium of both the right and left ventricles. | Heart | |
| Foyaca-Sibat et al. [ | Echocardiogram found multiple cysts in papillary muscles and interventricular septum. The patient had bradycardia and II grade AV block. | Brain and heart | ||
| Ade et al. [ | Brazil | 26-year-old male | Cerebral and subcutaneous cysticercosis; multiple cysts were found myocardium by echocardiogram. | Brain and heart |
| Eberly et al. [ | USA | 16-year-old boy | A left ventricular cyst was discovered during a screening echocardiogram. | Heart |
| Shogan et al. [ | USA | 17-year-old boy | Hypertension with non-enhancing, exophytic, ovoid mural-based fluid density in the left ventricle; biopsy confirmed CC. | Heart |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsParasitic infections in humans and animals · Parasite Biology and Host Interactions · Parasites and Host Interactions
Introduction
Cysticercus represents the larval stage of the tapeworm Taenia solium. In humans, the definitive host, adult tapeworms, inhabit the small intestine, while the larval forms are located in the skeletal muscle of the intermediate host, typically pigs. The development of cysticercosis in humans involves their role as an alternative to pigs in the T. solium life cycle, where eggs must mature within the human small intestine as they would in a pig's intestine. The entry of eggs into the human small intestine can occur through autoinfection, ingestion, or inhalation of food or water contaminated with eggs. Subsequently, these cysticercus migrate through the intestinal wall and are transported by the bloodstream to various tissues, including muscles, brain, and subcutaneous tissues, resulting in clinical symptoms. Disseminated cysticercosis (DCC) represents a rare presentation of a prevalent illness [1]. In 2010, the World Health Organization (WHO) designated it as a neglected tropical disease (NTD), while in 2014, the Food and Agriculture Organization of the United Nations (FAO) classified it as a negligible zoonotic disease (NZD) [2].
We present a case of a young male who suffered a snakebite, and upon examination, significant cardiac abnormalities and cysticercosis were discovered, ultimately contributing to his demise.
Case presentation
A 23-year-old male was brought to the emergency department on 06/08/2022 with a reported history of a snakebite that occurred around 2 PM the same day. Upon examination, two incised wounds were noted on the upper limb, where the nearby individuals attempted to suck out the venom. Despite efforts to save the patient, he was declared dead upon arrival at All India Institute of Medical Sciences (AIIMS), Rishikesh, India, at 07:22 PM on 06/08/2024.
Autopsy findings
The body was of average build, with a red tourniquet present over the left upper arm. The eyes were congested, and their corneas were hazy. Postmortem hypostasis was present over the dependent parts and the back, except the pressure points, and was fixed. Rigor mortis was present all over the body and well-developed.
The heart of the deceased was examined during the postmortem examination, revealing a heart weighing 320 grams. The root of the aorta and aortic valve exhibited atheromatous changes with calcification. Multiple collateral vessels were observed, originating from the left main coronary artery and extending along its course. The left main coronary artery itself showed atheromatous changes with a 40% lumen blockage, situated 0.5 cm distal to its origin. Furthermore, numerous cystic nodules with calcified margins containing muddy fluid were discovered on the surface of the left ventricle, the base of the aorta, and the left atrium (Figures 1-3). A similar cystic nodule was identified on the interventricular septum (Figure 4).
Cystic lesions over the surface of the left atrium
Cystic lesions over the surface of the left ventricle
Cystic lesion over the interventricular septum with cysticercus larvae as zoomed in the right corner of this image
Cystic lesion seen over the root of the aorta
Microscopic examination of heart sections revealed unremarkable cardiac myocytes with focal areas of fibrosis, indicative of an old infarct. Additionally, one of the coronary arteries showed thrombosis with hyalinization of the wall, accompanied by a dense chronic inflammatory cell infiltrate. Intriguingly, during the histopathological examination, a cyst was identified within the myocardium, which was confirmed to contain a cysticercus larva. These features were consistent with cardiac cysticercosis (Figures 5, 6).
Transverse section showing the hooklets of cysticercus larvae within the myocardium (100x H&E)
Transverse section showing the hooklets of cysticercus larvae (zoomed in) within the myocardium (100x H&E)
Discussion
This case illustrates the complexity of clinical presentations and the importance of a comprehensive autopsy examination. The patient's history of a snakebite initially seemed to be the apparent cause of death. However, upon further investigation, several significant cardiac abnormalities, including atheromatous changes, coronary artery blockage, and the presence of collateral vessels, were identified. The larval stage of the parasite T. solium causes cysticercosis. In regions where the infection is expected, the prevalence of cysticercosis is approximately 1%-2%. The condition primarily affects the central nervous system, subcutaneous tissues, skeletal muscles, abdominal organs, and eyes. Cardiac involvement is considered uncommon in cases of cysticercosis [3]. Autopsy studies have shown that the frequency of cardiac involvement among individuals with DCC can reach up to 27%.
Cysticerci, the larval stage of T. solium, can be detected in various heart parts, including the subendocardium, myocardium, and epicardium. They have been found in the left and right ventricular walls, the interventricular septum, the valvular apparatus, and the papillary muscles. These cysticerci typically appear as thin-walled, semi-transparent structures filled with serous fluid. They are oval, measuring up to 30 mm in diameter, and possess a characteristic scolex [3]. As far back as 1912, British Army medical officers stationed in India reported the widespread dissemination of cysticerci throughout the human body [4]. Following those initial reports, subsequent studies should have emphasized this clinical presentation due to its relative rarity [5]. The primary characteristics of DCC encompass intractable epilepsy, dementia, muscle enlargement, and subcutaneous and lingual nodules.
Notably, focal neurological signs or apparent indications of raised intracranial pressure are generally absent, at least until the later stages of the disease [3,6]. The precise impact of immunity on restricting the frequency or widespread occurrence of the disease in humans is not firmly established. However, an autopsy survey conducted in Mexico revealed a connection between immunodeficiency and neurocysticercosis in children [7]. As observed in this case report, the generalized form of cysticercosis may remain asymptomatic, often detected only during autopsies. Nonetheless, it is plausible that the ultimate cardiac dysfunction exhibited by our patient was exacerbated by the extensive cardiopulmonary infestation [8]. Cysticercosis involving the pulmonary and cardiac systems is infrequent. Typically, the diagnosis is confirmed by observing the resolution of lesions following medical treatment with praziquantel or albendazole [9]. Identifying a scolex within a cystic lesion often indicates a diagnosis of cysticercosis [10]. Recognizing DCC clinically and conducting suitable radiological investigations are crucial as this condition requires well-structured therapeutic management. Patients under treatment with active cysts still carry the risk of encountering severe complications [11].
Additionally, the unexpected discovery of cardiac cysticercosis highlights the importance of considering alternative etiologies in cases with atypical findings. Cysticercosis, caused by the larval stage of T. solium, is not typically linked with incidents such as snakebites. Nevertheless, its presence in this case emphasizes the significance of a thorough autopsy examination to uncover all potential contributing factors to the patient's demise. A literature review of cases reported worldwide involving the heart is presented in tabulated form (Table 1) [12-40].
Conclusions
This case report describes a snakebite complicated by significant cardiac abnormalities and cardiac cysticercosis. The findings underscore the importance of conducting detailed autopsy examinations to evaluate complex clinical cases comprehensively. Recognizing atypical presentations and concurrent pathologies is crucial for gaining a comprehensive understanding of the cause of death, thus informing future medical practices and interventions. Diagnosing disseminated cardiac cysticercosis and conducting required investigations are essential as this condition necessitates strategic therapy. Patients undergoing treatment and still exhibiting active cysts remain vulnerable to severe complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cysticercosis Tropical Infectious Diseases (Second Edition): Principles, Pathogens, & Practice Garcia HH Wittner M Coyle CM Tanowitz HB White AC 12891303 London, UK Churchill Livingstone 22006
- 2Taeniasis/cysticercosis 2 2024 2024 https://www.who.int/news-room/fact-sheets/detail/taeniasis-cysticercosis
- 3Cardiac cysticercosis Int J Cardiol Spina R Sandaradura I Puranik R Lee AS 55755920201310.1016/j.ijcard.2013.01.18323465559 · doi ↗ · pubmed ↗
- 4Cysticercosis Manson's Tropical Disease Baily GG 15841595 London, UK Saunders 2003
- 5Disseminated cysticercosis. New observations, including CT scan findings and experience with treatment by praziquantel Brain Wadia N Desai S Bhatt M 5976141111988338291310.1093/brain/111.3.597 · doi ↗ · pubmed ↗
- 6Human cysticercosis and Indian scenario: a review J Biosci Prasad KN Prasad A Verma A Singh AK 5715823320081920898210.1007/s 12038-008-0075-y · doi ↗ · pubmed ↗
- 7Host response in childhood neurocysticercosis. Some pathological aspects Childs Nerv Syst Sanz CR 20620731987369055610.1007/BF 00274046 · doi ↗ · pubmed ↗
- 8Operational studies on the control of Taenia solium taeniasis/cysticercosis in Ecuador Bull World Health Organ Cruz M Davis A Dixon H Pawlowski ZS Proano J 401407671989 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 2491261/pdf/bullwho 00062-0059.pdf 2805217 PMC 2491261 · pubmed ↗