Mathematical model for evaluating bicarbonate and lactate kinetics in metformin-associated lactic acidosis
João João Mendes, Mauro Pietribiasi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
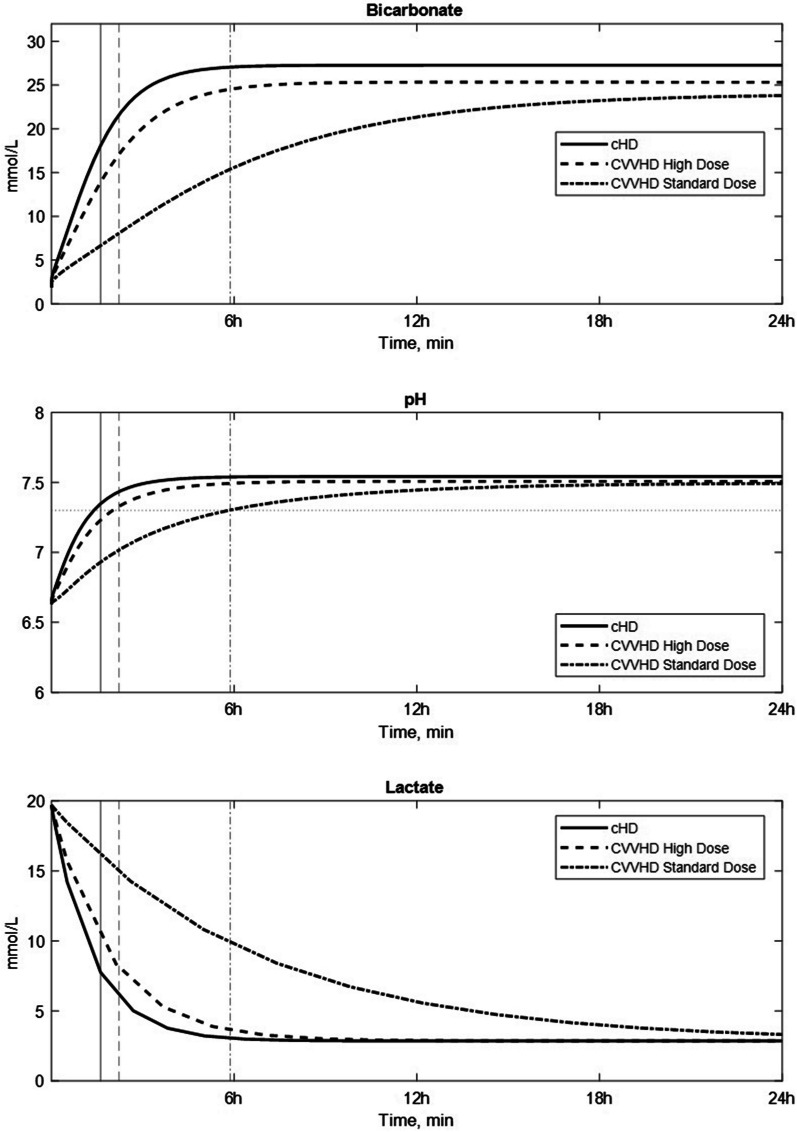 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal function and acid-base balance · Potassium and Related Disorders · Diet and metabolism studies
To the Editor,
Metformin-associated lactic acidosis (MALA) refers to a blood lactate concentration greater than 5 mmol/L and arterial pH less than 7.35 in association with metformin exposure [1]. The mainstay of therapy for MALA is resuscitation and supportive care. Extracorporeal treatments (ECTRs) are indicated if there is failure of standard supportive care, pH ≤ 7.0 or lactate concentration > 20 mmol/L [2].
The use of different ECTRs—conventional hemodialysis (cHD) or continuous renal replacement therapy (CRRT)—is dependent on both clinical factors (e.g., presence of hypotension or shock) and great heterogeneity in equipment availability [3].
There is no mathematical model in the literature describing the complex effect of ECTRs in MALA, which results from the interactions between the delivery of a base (e.g., bicarbonate) via diffusion from a dialysis solution, lactate clearance and metformin clearance.
Using clinical data, we trained a comprehensive, multi-compartment, computational model of carbon dioxide and oxygen transport calculating the acid–base blood biochemistry during hemodialysis [4] to describe the correction of acidosis in MALA. Hyperlactataemia does not mechanistically contribute to acidaemia. Excess hydrogen ions do not result from glycolysis and production of lactate but from other metabolic pathways, namely, the hydrolysis of the ATP generated during anaerobic respiration [5]. We, therefore, described lactate removal by ECTR independently of bicarbonate delivery, using a simple single-pool kinetic model, as lactate clearance does not contribute to pH correction. We then used the models to simulate a comparison of different ECTRs for a virtual patient with MALA. The patient was assumed male, 80 kg, of which 50% as total body water; initial serum bicarbonate concentration was 1.9 mmol/L, pCO_2_ was 17.7 mmHg, and pO_2_ was 142 mmHg (data based on a single case patient admitted in the clinic with MALA).
For cHD, we used: (1) blood flow rate (Qb) of 200 mL/min, the average blood flow obtainable with a conventional provisory catheter; (2) dialysate flow rate (Qd) of 500 mL/min, the normal dialysate flow; and (3) bicarbonate dialysate concentration of 32 mmoL/L, the highest readily available concentration. For CRRT, we considered a standard dose and a high dose scenario. The standard dose scenario corresponds to continuous venovenous hemodialysis (CVVHD) mode with: (1) Qb of 200 mL/min; (2) Qd of 33.3 mL/min, corresponding to an effluent dose of 25 mL/Kg/h which is the maximum standard dose; and (3) bicarbonate dialysate concentration of 32 mmoL/L. The high dose scenario for CVVHD was modelled using Qd of 133.3 mL/min, and the maximum flow rate of the equipment which allows a near-complete saturation of the dialysate. Zero net fluid removal was assumed for all treatments.
The results of the simulation (Fig. 1) demonstrated a greater efficacy of cHD compared to CRRT, which when used should be delivered in maximum dose.Fig. 1. Predicted bicarbonate, pH and lactate concentration profile in the extracellular compartment with conventional hemodialysis (cHD), standard dose continuous venovenous haemodialysis (CVVHD) and high dose continuous venovenous haemodialysis (CVVHD). The vertical lines intersecting the dotted horizontal line represent the instants when the threshold pH of 7.30 is reached (for each treatment, coded as per legend): 97 min for cHD, 133 min for high dose CVVHD and 352 min for standard dose CVVHD)
This simulation provides evidence to support mathematical modelling for comparing the theoretical performance of different ECTRs and help in refining the guidelines for the use of dialysis in treating MALA.
Matlab code: https://doi.org/10.18150/GZRAXA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Luft D Deichsel G Schmulling RM Stein W Eggstein M Definition of clinically relevant lactic acidosis in patients with internal diseases Am J Clin Pathol 198380448448910.1093/ajcp/80.4.4846624712 · doi ↗ · pubmed ↗
- 2Calello DP Liu KD Wiegand TJ Roberts DM Lavergne V Gosselin S Extracorporeal treatment for metformin poisoning: systematic review and recommendations from the extracorporeal treatments in poisoning workgroup Crit Care Med 20154381716173010.1097/CCM.000000000000100225860205 · doi ↗ · pubmed ↗
- 3Dichtwald S Weinbroum AA Sorkine P Ekstein MP Dahan E Metformin-associated lactic acidosis following acute kidney injury. Efficacious treatment with continuous renal replacement therapy Diabet Med.201229224525010.1111/j.1464-5491.2011.03474.x 21977945 · doi ↗ · pubmed ↗
- 4Pietribiasi M Waniewski J Leypoldt JK Mathematical modelling of bicarbonate supplementation and acid-base chemistry in kidney failure patients on hemodialysis P Lo S ONE 2023182 e 028210410.1371/journal.pone.028210436827348 PMC 9955675 · doi ↗ · pubmed ↗
- 5Zilva JF The origin of the acidosis in hyperlactataemia Ann Clin Biochem 1978151404310.1177/00045632780150011124406 · doi ↗ · pubmed ↗