Papillary Traction Due to the Posterior Form of a Bilateral Persistent Fetal Vasculature Mimicking Papilledema
Hamza Lazaar, Taha Boutaj, Meryem Sefrioui, Boutayna Azarkan, Saad Benchekroun, Noureddine Boutimzine, Abdellah Amazouzi, Lalla Ouafa Cherkaoui

TL;DR
A seven-year-old child presented with a rare bilateral eye condition mimicking papilledema, caused by persistent fetal vasculature.
Contribution
This case report describes a rare bilateral posterior form of persistent fetal vasculature with papillary traction.
Findings
Fundus examination showed congested pseudopapilledema with a brownish band in both eyes.
Ultrasound and OCT confirmed papillary traction due to persistent fetal vasculature.
The condition was diagnosed without a family or personal medical history suggesting it.
Abstract
Persistent fetal vasculature (PFV), or persistent hyperplastic primary vitreous (PHPV), is a congenital developmental disorder characterized by a failure of resorption of the hyaloid system. It typically presents unilaterally and has three forms: anterior, posterior, and mixed. In this case report, a seven-year-old patient, without specific personal or family medical history, was referred from the pediatric department for bilateral papilledema. The patient had a best-corrected visual acuity of 20/20 (Logarithmic Measure of Angle of Resolution (LogMAR): 0) in both eyes. Fundus examination of both eyes revealed congested pseudopapilledema with a short, mobile, brownish band extending from the optic disc towards the vitreous cavity. Ocular ultrasound of both eyes showed a fine hyperechoic line pulling on the optic nerve head, and papillary optical coherence tomography (OCT) showed a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
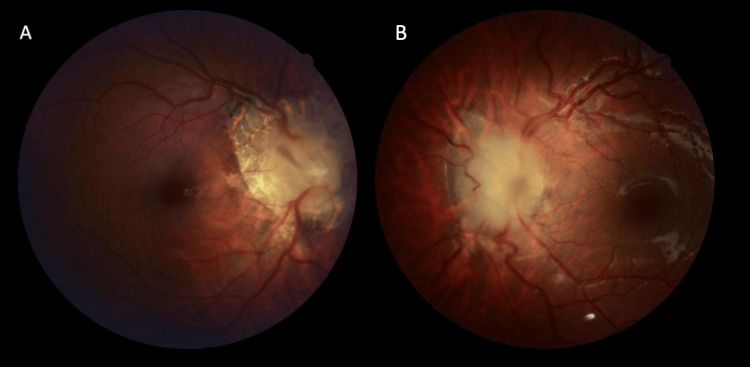 Figure 1
Figure 1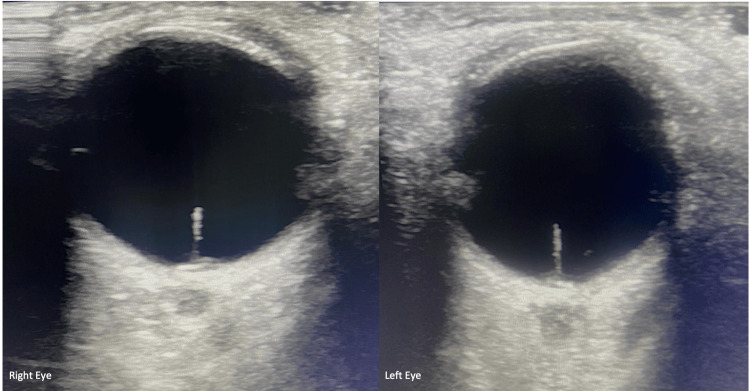 Figure 2
Figure 2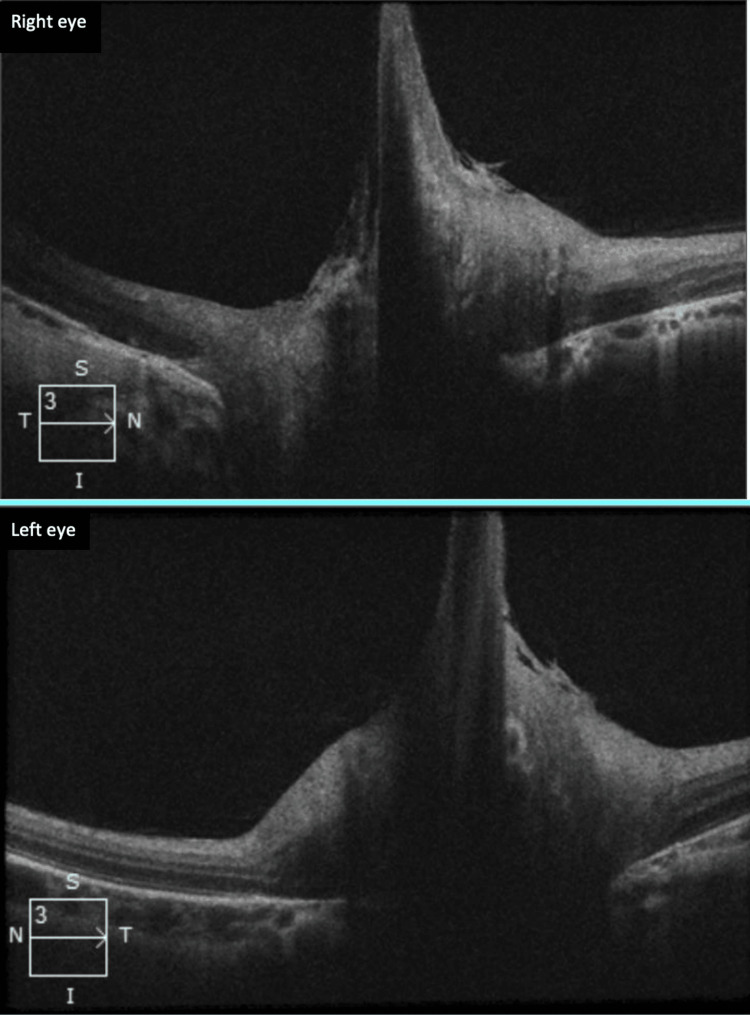 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurological Complications and Syndromes · Maternal and fetal healthcare · Fetal and Pediatric Neurological Disorders
Introduction
Persistent fetal vasculature (PFV), or persistent hyperplastic primary vitreous (PHPV), is a congenital developmental disorder marked by a failure of resorption of the hyaloid system [1]. It typically presents unilaterally, rarely bilaterally, and comes in three distinct forms: an anterior form, a posterior form (the rarest), and a mixed form [2]. It is considered one of the main differential diagnoses of retinoblastoma [2]. Also, it can cause serious complications such as angle-closure glaucoma, hyphemia, vitreous hemorrhage, and tractional retinal detachment [3]. We report an extremely rare case of a posterior and bilateral form complicated by papillary traction mimicking bilateral papilledema.
Case presentation
We report the case of a seven-year-old girl, without notable personal or family medical history, referred from the pediatric department in our institution for further management of bilateral papillary edema. She had previously undergone a brain MRI, which revealed no abnormalities.
Upon ophthalmological evaluation, the patient had a best-corrected visual acuity of 20/20 (Logarithmic Measure of Angle of Resolution (LogMAR): 0) in both eyes. Pupils were equal and reactive, with no leukocoria or strabismus. The anterior segment examination of both eyes showed clear corneas with normal diameter, well-depth anterior chambers, no aniridia, and clear lenses without opacities.
Fundus examination of both eyes (Figure 1) revealed congested peripapillary vessels, a markedly elevated and blurred-edged optic disc without hemorrhages or exudates, along with peripapillary chorioretinal atrophy for the right eye (Figure 1A). A short, mobile, brownish band extending from the optic disc towards the vitreous cavity was observed.
Fundus photographs of both eyes show an optic disc with blurred contours and elevated margins, from which emanates a short, brownish fibrous band. (A: right eye; B: left eye)
Ocular ultrasound of both eyes revealed a bilaterally fine hyperechoic line emanating from the optic nerve head, causing its elevation. The axial length was measured at 19.5 mm in both eyes (Figure 2).
Ocular ultrasound of both eyes shows a fine hyperechoic line pulling on the optic nerve head.
Papillary optical coherence tomography (OCT) (Figure 3) revealed papillary traction with a fibrous band pulling the optic disc towards the vitreous cavity. There was no traction on the macula and no evidence of retinoschisis.
Papillary OCT of both eyes shows bilateral papillary traction on persistent fetal vascularization.OCT: optical coherence tomography
The diagnosis of a posterior and bilateral form of persistent fetal vasculature with papillary traction was established.
Although surgical intervention could have been considered for treatment, a careful evaluation of the benefit-risk balance, given the patient's visual acuity of 20/20 and the absence of visual symptoms, led to the decision to opt for a conservative and non-surgical approach with close monitoring. The patient's condition remained stable, both anatomically and functionally, throughout the follow-up.
Discussion
Described initially by Reese in 1945 [4], PFV, or PHPV, is a rare vitreoretinal malformation resulting from a failure of resorption of the primitive vitreous and the hyaloid vascular system during embryonic life [1]. Our case stands out due to three rare features: the form of its clinical presentation (pure posterior involvement), its bilaterality, and papillary traction giving the appearance of pseudopapilledema.
The clinical presentation is subdivided into three forms. An anterior form, representing 25% to 35.5% of cases [5, 6], typically presents with leukocoria related to the retrolental fibrovascular membrane or posterior capsular cataract, with an unremarkable posterior pole [7]. A mixed form, the most common, represents 42% to 77% according to series [5], combining a fibrovascular membrane and a vascular band linking to the posterior capsule of the lens [7]. The posterior form, or Bergmeister papilla, the rarest, represents 12% to 22% of cases [5, 6].
In most series, hyperplastic persistence of the primitive vitreous is typically unilateral in over 90% of cases [4]. Bilateral forms account for less than 2.4% in certain series, such as the series of Pollard et al. [8]. They are generally associated with other ocular and genetic malformations [1], such as trisomy 13, trisomy 18, and Norrie disease [9]. In our case, there were no ocular or visceral malformations.
The main differential diagnosis is congenital cataract and retinoblastoma. To our knowledge, this is the first case of bilateral posterior fetal vascularization persistence complicated by papillary traction. A unilateral form of Bergmeister papilla with traction has been reported in the literature [10].
Other rare complications have been described, such as tractional retinal detachment, macular retinoschisis, and vascular thrombosis with vitreous hemorrhages [11, 12].
Conclusions
Persistent fetal vasculature can be a devastating developmental anomaly that remains an important cause of amblyopia and visual disabilities in children. The patient presents an exceptional case with good visual acuity characterized by an atypical form of fetal vascularization, including three rare clinical features, bilaterality, posterior form, and papillary traction, which is a complication rarely described in the literature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Persistent fetal vasculature (PFV): an integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV). LIV Edward Jackson Memorial Lecture Am J Ophthalmol Goldberg MF 5876261241997937271510.1016/s 0002-9394(14)70899-2 · doi ↗ · pubmed ↗
- 2Bilateral persistent hyperplastic primary vitreous Indian J Ophthalmol Jain TP 53545720091907541210.4103/0301-4738.44487 PMC 2661510 · doi ↗ · pubmed ↗
- 3Surgical treatment and visual outcomes of cataract with persistent hyperplastic primary vitreous Int J Ophthalmol Li L Fan DB Zhao YT Li Y Cai FF Zheng GY 3913991020172839303010.18240/ijo.2017.03.11PMC 5360774 · doi ↗ · pubmed ↗
- 4Persistence and hyperplasia of the primary vitreous : tunica vasculosa lentis or retrolental fibroplasia Trans Am Ophthalmol Soc Reese AB Payne F 163192431945 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 1315166/16693375 PMC 1315166 · pubmed ↗
- 5Persistent hyperplastic primary vitreous Clin Eye Vis Care Silbert M Gurwood AS 1311371220001113742710.1016/s 0953-4431(00)00054-0 · doi ↗ · pubmed ↗
- 6Persistent hyperplastic primary vitreous: a retrospective study (Article in French)J Fr Ophtalmol Roche O Orssaud C Beby F Sylla FK Allali L Dufier JL 48349130 https://www.em-consulte.com/article/113459/persistance-et-hyperplasie-du-vitre-primitif%C 2%A 0-etud 10.1016/s 0181-5512(07)89628-817568341 · doi ↗ · pubmed ↗
- 7Vitreous pathology Ophtalmologie Pédiatrique N'Guyen E Gastaud P Paris, France Elsevier Massonhttps://www.em-consulte.com/em/SFO/2017/file_100015.html 2017 https://www.em-consulte.com/em/SFO/2017/file_100015.html
- 8Persistent hyperplastic primary vitreous: diagnosis, treatment and results Trans Am Ophthalmol Soc Pollard ZF 487549951997 https://pubmed.ncbi.nlm.nih.gov/9440186/9440186 PMC 1298374 · pubmed ↗