Leukemia cutis simulating drug reaction with eosinophilia and systemic symptoms following beta-lactam antibiotic use
Jaclyn Abraham, Navid Farahbakhsh, Kiran Motaparthi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
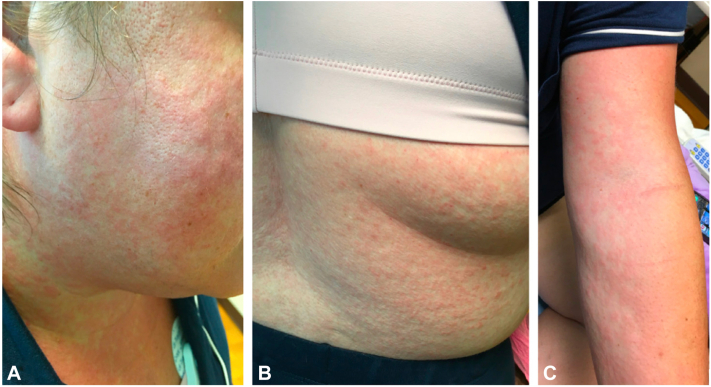 Figure 1
Figure 1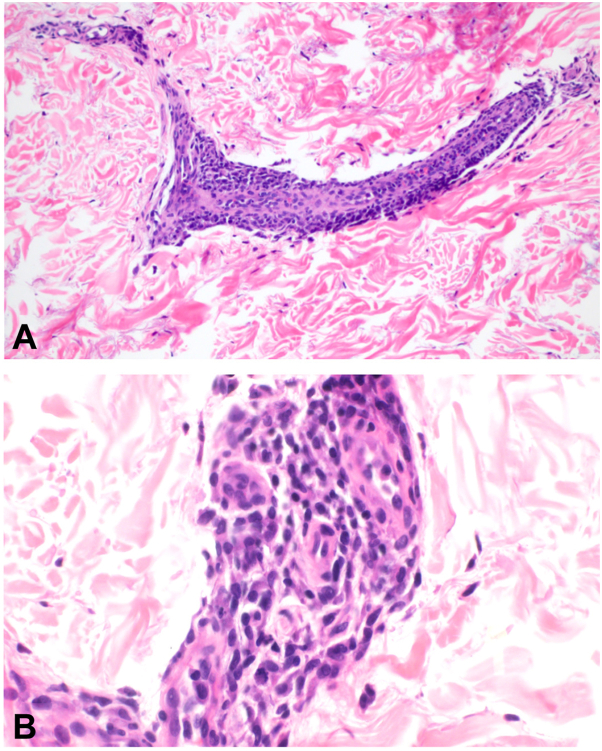 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEosinophilic Disorders and Syndromes · Acute Myeloid Leukemia Research · Drug-Induced Adverse Reactions
Introduction
Leukemia cutis (LC) is an extramedullary manifestation of leukemia that presents as discernible cutaneous lesions composed of neoplastic leukocytes.1^,^2 It is estimated that 10% to 15% of patients with acute myeloid leukemia (AML) develop LC, with varying frequency based on the subtype of AML.1 A wide range of morphological findings are associated with LC, including erythematous, red-brown, or violaceous papules, plaques, nodules, or tumors that can ulcerate or become bullous.3 Lesions often present on the head, neck, and trunk, with an affinity for sites of prior or concurrent inflammation.1 We describe an atypical presentation of LC which fulfilled RegiSCAR criteria for drug eruption with eosinophilia and systemic symptoms (DRESS) following the recent completion of a beta-lactam antibiotic course.
Case report
A 41-year-old woman was evaluated by the dermatology inpatient consult service for a 2-day history of a pruritic eruption involving the face, neck, trunk, and bilateral upper extremities. The patient was febrile (up to 38.6 °C) and reported facial swelling with a sore throat. Four days prior to hospital admission, the patient completed a 1-week prophylactic course of cefalexin following a double mastectomy for recently diagnosed stage IA breast cancer.
Numerous erythematous macules and papules involving the face, neck, trunk, upper extremities, and proximal thighs were present (Fig 1). Physical examination was also significant for cervical, axillary, and inguinal lymphadenopathy and facial edema.Fig 1. Diffuse erythematous macules and papules symmetrically distributed on the face and neck (A), flank (B), and forearm (C).
Initial laboratory studies showed leukocytosis (white blood cell count of 66.1 × 10^3^/μL), eosinophilia (absolute eosinophil count of 990 cells/μL), monocytosis (17%), elevated creatinine (1.31 mg/dL), and mild transaminitis (aspartate aminotransferase 57 U/L, alanine aminotransferase 92 U/L). Serological testing for Epstein-Barr virus, cytomegalovirus, human immunodeficiency virus, Treponema palladium IgG, and hepatitis B and C were negative. A peripheral blood smear showed atypical lymphocytes.
Based on the clinical and laboratory findings, the differential diagnosis included DRESS, favored based on the patient’s symptoms and laboratory findings with a latency of 1 week following beta-lactam administration. The patient had a calculated RegiSCAR score of 7 at the time of presentation, indicating a “definite case” of DRESS (Table I).3^,^4 However, the patient’s hyperleukocytosis prompted further workup to rule out other disease etiologies, including an underlying hematologic malignancy.Table IDiagnosis of drug eruption with eosinophilia and systemic symptoms based on RegiSCAR criteria3^,^4FeaturesNoYesUnknownFever (>38.5 °C)−11−1Lymphadenopathy (2 or more sites, >1 cm)010Atypical lymphocytes010Eosinophilia0−0 0.7-1.499 × 10^9^/L1 ≥1.5 × 10^9^/L2Skin rash extent >50%010At least 2 of: edema, purpura, infiltration, scaling010Biopsy suggesting DRESS−110Internal organ involved0−0 One1 Two or more2Resolution in >15 days−10**−1Alternative diagnoses excluded (by ≥3 biological investigations)01**0Final RegiSCAR group score interpretation: <2, no case; 2 to 3, possible case; 4 to 5, probable case; >5, definite case; bolded values represent features specific to the case presented (total = 7 points).DRESS, Drug eruption with eosinophilia and systemic symptoms.
A punch biopsy was performed. Hematoxylin-eosin–stained sections revealed a dermal and subcutaneous infiltrate of perivascular medium-sized mononuclear cells with enlarged hyperchromatic nuclei consistent with blasts (Fig 2).Fig 2. Dermal and subcutaneous infiltrate of perivascular medium-sized mononuclear cells (A) with enlarged hyperchromatic nuclei consistent with blasts (B) (A and B, Hematoxylin-eosin stain; original magnification: A and B, 400× magnification).
Immunohistochemical staining revealed CD4 and CD56 positive cells; medium-sized blasts expressed CD43, lysozyme, and CD68. Markers for CD34, CD117, CD123, and myeloperoxidase were negative. Bone marrow biopsy and flow cytometry of the bone marrow and blood matched the immunohistochemical profile from the skin, which was consistent with acute monocytic leukemia (AMoL). Lymph node biopsy demonstrated myeloid sarcoma. Based on these results, the diagnosis of LC secondary to AMoL was confirmed. Given that our patient had 2 new simultaneous, but unrelated malignancies, the oncology team prioritized the treatment for AMoL. The patient’s rash and systemic symptoms slowly improved following chemotherapy.
Discussion
This case of LC simulating DRESS underscores the high index of clinical suspicion required to diagnose LC, particularly in patients without a known hematologic malignancy. Cutaneous involvement as the presenting feature of leukemia is rare, as most patients who present with LC will already have an established diagnosis of leukemia.5 Moreover, our patient presented with an acute, pruritic morbilliform (exanthematous) eruption and systemic symptoms, which contrasts typical presentation of LC. LC usually presents with smooth, erythematous to violaceous papules, plaques, or nodules with a localized or disseminated distribution.5 Very few studies have described cases of LC simulating inflammatory dermatoses.6^,^7 For example, Donaldson et al reported a case of LC presenting as erythroderma shortly after induction chemotherapy for AML.6
In addition to our patient’s atypical cutaneous presentation, the temporal relationship between the patient’s symptom onset and recent beta-lactam antibiotic use posed an additional diagnostic challenge. While DRESS typically presents 2 to 8 weeks after administration of the inciting drug,3 recent studies have suggested there is a significantly shorter latency period for beta-lactam antibiotics compared to other drug classes. The median latency period for patients with suspected beta-lactam-induced DRESS was 4.5 days compared to 16 days for vancomycin-associated DRESS.3
Of note, our patient presented with markedly elevated leukocytosis (66 × 10^3^/μL). Although DRESS can present with leukemoid reactions including white blood cell counts upward of 50 × 10^3^/μL, hyperleukocytosis at the time of an AML diagnosis is a rare but notable feature that portends a poor prognosis.8 This significant hematologic abnormality prompted further workup, which led to the prompt diagnosis of LC secondary to AMoL in our patient.
For an acute exanthematous eruption with fever and lymphadenopathy, the differential diagnosis includes mononucleosis with recent beta-lactam use, acute retroviral syndrome due to human immunodeficiency virus, secondary syphilis, DRESS, and angioimmunoblastic T-cell lymphoma (Table II). Although rare, physicians should also consider LC in patients presenting with morbilliform rash, fever, and lymphadenopathy.Table IIDifferential diagnosis for acute exanthematous eruption with fever and lymphadenopathyLCDRESSMononucleosisARSSecondary syphilisAITLOnsetVariesTwo-8 wk following drug exposureDay ∼4 of illness; recent beta-lactam antibiotic useThree-6 wk following HIV exposureThree-10 wk following chancreVariesDistribution of lesionsFace, trunk, extremitiesFace, upper trunk, extremitiesTrunk and proximal extremitiesWidespreadWidespreadWidespreadAdditional featuresMalaise, headache, arthralgias, hepatosplenomegalyFacial edema, pruritusMalaise, pharyngitis, splenomegalyMalaise, myalgias, pharyngitis, orogenital ulcerationsFlu-like illness, weight loss, pharyngitis, mucosal lesions, alopecia, hepato-splenomegalyPruritus, weight loss, night sweats, hepatosplenomegalyDiagnosisSkin biopsyRegiSCAR criteriaMonospot testHIV serological assaysT palladium IgGLymph node biopsyTreatmentChemotherapy for underlying malignancyWithdrawal of offending agentSupportiveAntiretroviral therapy (ART)Intramuscular benzathine penicillin GChemotherapyAITL, Angioimmunoblastic T-cell lymphoma; ARS, acute retroviral syndrome; DRESS, drug eruption with eosinophilia and systemic symptoms; LC, leukemia cutis.Adapted from Dermatology.9
LC often indicates advanced disease and a poorer prognosis, since 90% of patients will have additional sites of extramedullary disease involvement.1^,^2^,^10 Diagnosis is made based on clinical presentation, cytology, and the immunophenotype of malignant cells.1 Peripheral blood findings and bone marrow biopsy can also help establish the diagnosis.1 Remission of the hematologic abnormalities and partial to complete resolution of the cutaneous infiltrates typically follows chemotherapy.5^,^7
Although the RegiSCAR criteria are widely used to clinically diagnose DRESS, these were initially established for research studies but were not validated for use in the clinical setting.4 Limitations include lack of specificity for certain criteria, including hematologic abnormalities, organ involvement, and skin biopsy findings. For example, the presence of atypical lymphocytes may also be observed in viral infections; conversely, patients with DRESS and pancytopenia may not develop atypical lymphocytes or eosinophilia.4 RegiSCAR also requires the exclusion of at least 3 of the following: hepatitis A/B/C, Chlamydia or Mycoplasma infection, antinuclear antibody, and blood culture. However, RegiSCAR does not require testing for other viral infections that may be clinically indiscernible from DRESS, such as Epstein-Barr virus or cytomegalovirus infection.4 Therefore, we aim to raise awareness of these important limitations when utilizing diagnostic criteria in any clinical scenario where DRESS enters the differential diagnosis.
Conflicts of interest
None disclosed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cho-Vega J.H.Medeiros L.J.Prieto V.G.Vega F.Leukemia cutis Am J Clin Pathol 1291200813014210.1309/wyacywf 6ngm 3wbrt 18089498 · doi ↗ · pubmed ↗
- 2Ratnam K.V.Khor C.J.Su W.P.Leukemia cutis Dermatol Clin 12219944194318045053 · pubmed ↗
- 3Waldron J.L.James F.Vogrin S.A shorter time to drug reaction with eosinophilia and systemic symptoms (DRESS): redefining beta-lactam-associated DRESS Clin Infect Dis 764202377277410.1093/cid/ciac 79836190825 · doi ↗ · pubmed ↗
- 4Sibbald C.Shear N.H.Verstegen R.H.J.Flaws and limitations of classification criteria for drug reaction with eosinophilia and systemic symptoms J Allergy Clin Immunol Pract 11920232693269610.1016/j.jaip.2023.05.01737236348 · doi ↗ · pubmed ↗
- 5Parsi M.Go M.S.Ahmed A.Leukemia Cutis 2023 Stat Pearls 31082180 · pubmed ↗
- 6Martínez-EscanaméM.Zuriel D.Tee S.I.Fried I.Massone C.Cerroni L.Cutaneous infiltrates of acute myelogenous leukemia simulating inflammatory dermatoses Am J Dermatopathol 354201341942410.1097/DAD.0b 013e 31826 ffe 6f 23221486 · doi ↗ · pubmed ↗
- 7Donaldson M.Ebia M.I.Owen J.L.Choi J.N.Rare case of leukemia cutis presenting as erythroderma in a patient with acute myeloid leukemia JAAD Case Rep 52201912112310.1016/j.jdcr.2018.10.01930671526 PMC 6330369 · doi ↗ · pubmed ↗
- 8Daver N.Kantarjian H.Marcucci G.Clinical characteristics and outcomes in patients with acute promyelocytic leukaemia and hyperleucocytosis Br J Haematol 1685201564665310.1111/bjh.1318925312977 PMC 4323735 · doi ↗ · pubmed ↗