Exposed Embolic Coils Observed in a 64-Year-Old Male With Head and Neck Cancer Following Transarterial Embolization for Carotid Blowout Syndrome
Jia-Zheng Huang, Wei-Chen Lu, Bo-Ching Lee

TL;DR
A 64-year-old cancer patient had embolic coils from a previous procedure exposed in a neck wound, managed by cutting the coils and monitoring.
Contribution
This case report highlights a rare complication of transarterial embolization and a conservative management approach.
Findings
Exposed embolic coils were observed in a malignant wound following transarterial embolization.
Computed tomography angiography is crucial for assessing embolic coils in such cases.
Transection of exposed coils with close monitoring is a viable conservative management strategy.
Abstract
Background: Delayed migration and exposure of embolic coils is a rare complication of endovascular therapy for carotid blowout syndrome. Methods: A 64-year-old man with recurrent tongue cancer noticed the presence of foreign body in the malignant wound on the right side of his neck. He had undergone transarterial embolization on his right vertebral artery, right common carotid artery (CCA), and internal carotid artery (ICA) for carotid blowout syndrome 1 month prior. On physical examination, exposed spring-like metallic coils were observed, covered in brownish granulation tissue, at the bottom of the malignant wound. Neck radiograph and computed tomography confirmed the extrusion and migration of the embolic coils. Results: In this case, the patient was managed by transection of the exposed coils at the wound surface with close monitoring. Conclusions: Computed tomography angiography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
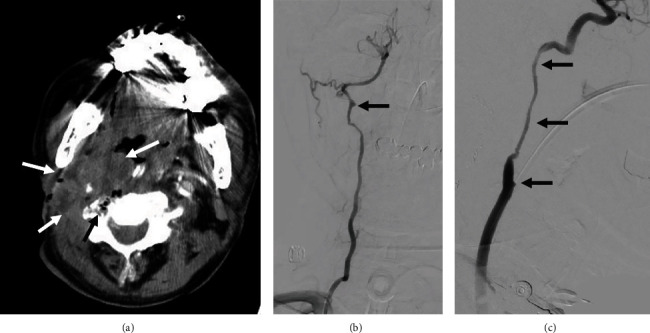 Figure 1
Figure 1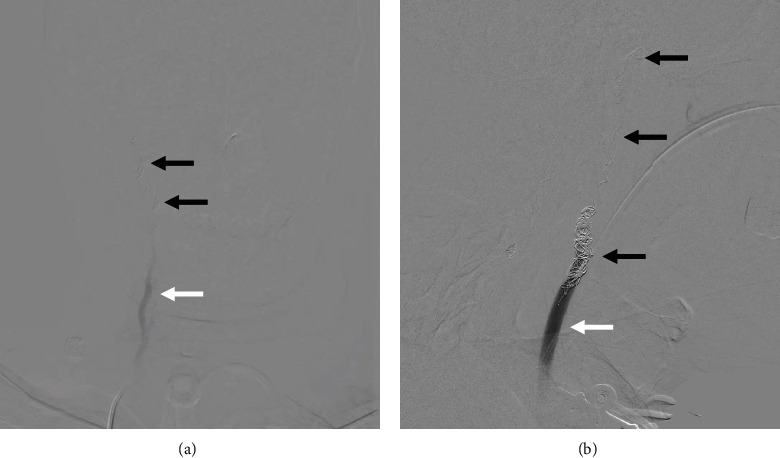 Figure 2
Figure 2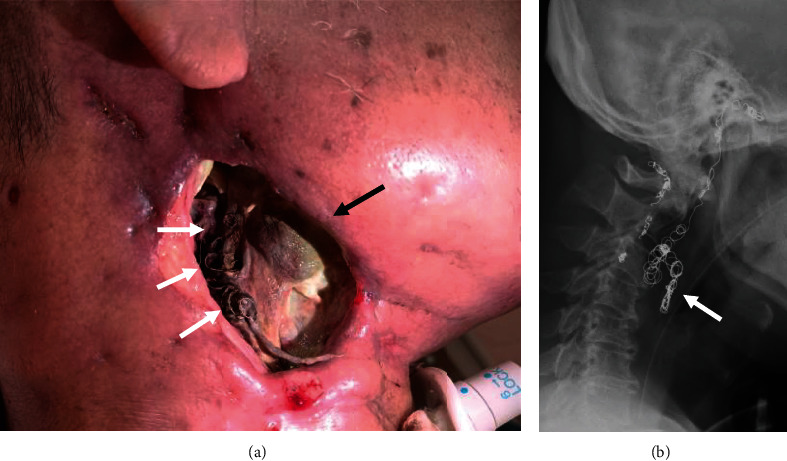 Figure 3
Figure 3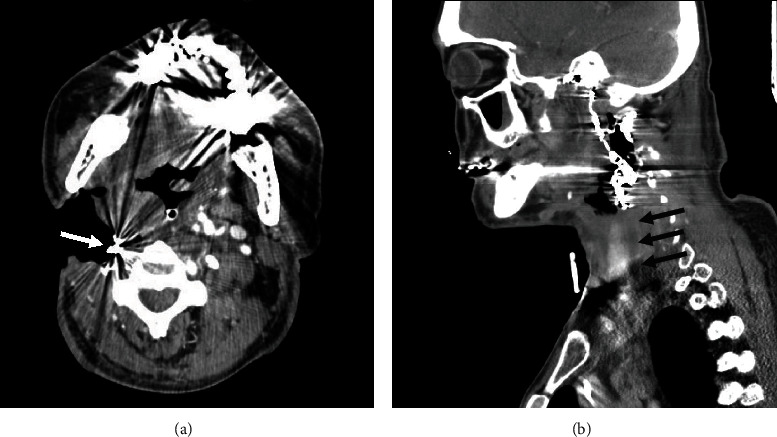 Figure 4
Figure 4- —National Science and Technology Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications
1. Introduction
Carotid blowout syndrome is a severe complication of the head and neck cancer with a mortality rate of around 50% [1]. The preferred treatment is endovascular due to its high efficacy in achieving hemostasis [2]. For patients with a robust collateral blood supply from the circle of Willis and a low risk of hypoperfusion, coil embolization of the carotid trunk can be an option, with a relatively lower risk of rebleeding compared to covered stents [3, 4]. While embolization of the external carotid artery typically has a high success rate with minimal complications, the complication rate, such as ischemic stroke, can be as high as 23.7% for embolization of carotid trunk [4, 5].
However, other complications, such as delayed migration of coil embolization for carotid blowout syndrome, are rarely reported in the literature. Therefore, we report the case of a carotid blowout syndrome status post coil embolization, which presented with an exposed embolization coil in the malignant wound.
2. Case Report
A 64-year-old man with a history of recurrent tongue cancer presented with exposed embolic coils in a malignant wound on his right neck. A decade prior, he had undergone wide excision and right neck lymph node dissection for right tongue cancer. Two years ago, a recurrence was detected in the right tongue base, leading to repeated tumor excision, lymph node dissection, and adjuvant chemoradiotherapy. However, 7 months ago, he developed skin metastasis and recurrent lymphadenopathies in the right neck. Oral uracil-tegafur (UFUR) was initiated as maintenance therapy, but the malignant wound continued to progress, necessitating wound dressing.
One month prior to this presentation, the patient experienced massive bleeding from the malignant wound, unresponsive to compression. Neck radiography and computed tomography angiography (Figure 1(a)) revealed threatened segments of the right vertebral artery, right common carotid artery (CCA), and right internal carotid artery (ICA) within the necrotic tumor. Angiography of these arteries revealed vascular irregularities resulting from tumor invasion (Figures 1(b) and 1(c)), and emergency coil embolization successfully controlled the bleeding (Figure 1(b)) using multiple MicroNester and Tornado pushable coils (up to 18-14-4, Cook Medical, Bloomington, IN) along with two Interlock-Fibered IDC Occlusion Systems (Boston Scientific, Natick, MA) until achieving flow stasis (Figure 2). No ischemic symptoms developed after coil embolization, and no antithrombotic therapy was administered. Afterward, this patient underwent targeted therapy for his head and neck cancer with nivolumab and afatinib. No radiotherapy or operation was performed during this period.
At this visit, the patient reported observing a coil-like metallic wire covered with brown granulation tissue at the wound's base. Neck X-rays confirmed the exposure and migration of embolization coils (Figure 3). Since there were still sufficient coils within the thrombosed lumen of the right CCA and right ICA on computed tomography angiography, conservative management by transection of the exposed coils was performed (Figure 4). During his 3-month hospitalization for treatment of malignant wound infection and pneumonia, no further episodes of massive bleeding occurred.
3. Discussion
This case emphasizes the occurrence of delayed exposure and migration of embolization coils, which is a rare complication of embolization in the carotid blowout syndrome [6]. Anoxia and necrosis are more prevalent and severe in head and neck cancer compared to many other types of malignancies [7], although the exact pathomechanism remains unclear. The presence of air-containing necrosis or abscess in patients with head and neck cancer serves as an important prognostic factor for patient survival and rebleeding [8, 9]. In this case, some air-containing necrosis was already evident on preprocedural CT before embolization, indicating its necrotic nature. Subsequently, prominent tumor necrosis and cavitation occurred following treatment of carotid blowout syndrome and antitumoral therapy, leading to exposure of the embolic coils. Since coils may become entangled with each other, we suggest to avoid directly pulling out the exposed coils until computed tomography angiography is performed, as this could potentially cause the displacement of other unaffected coils. When there are enough remaining embolic coils in the embolized artery and the lumen is thrombosed, a conservative management approach can be taken, as demonstrated in this case. If there is a high risk of recurrent carotid blowout syndrome due to insufficient intraluminal embolization coils, repeated embolization can be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen Y. J. Wang C. P. Wang C. C. Jiang R. S. Lin J. C. Liu S. A. Carotid blowout in patients with head and neck cancer: associated factors and treatment outcomes Head & Neck 201537226527210.1002/hed.235902-s 2.0-8492143972424375817 · doi ↗ · pubmed ↗
- 2Bond K. M. Brinjikji W. Murad M. H. Cloft H. J. Lanzino G. Endovascular treatment of carotid blowout syndrome Journal of Vascular Surgery 201765388388810.1016/j.jvs.2016.11.0242-s 2.0-8501406263328236928 · doi ↗ · pubmed ↗
- 3Lee B. C. Lin Y. H. Lee C. W. Liu H. M. Huang A. Prediction of borderzone infarction by CTA in patients undergoing carotid embolization for carotid blowout AJNR. American Journal of Neuroradiology 20183971280128510.3174/ajnr.A 56722-s 2.0-8504984474729773563 PMC 7655449 · doi ↗ · pubmed ↗
- 4Chang F.-C. Luo C.-B. Lirng J.-F. Endovascular management of post-irradiated carotid blowout syndrome P Lo S One 20151010, article e 013982110.1371/journal.pone.01398212-s 2.0-84947793113 PMC 459527626439632 · doi ↗ · pubmed ↗
- 5Zhao L. B. Shi H. B. Park S. Acute bleeding in the head and neck: angiographic findings and endovascular management AJNR American Journal of Neuroradiology 201435236036610.3174/ajnr.A 37612-s 2.0-8489415033624136646 PMC 7965746 · doi ↗ · pubmed ↗
- 6Ko H. Han A. Chang H. Min S. K. Carotid blowout syndrome of an infected pseudoaneurysm after radiation therapy of parotid cancer: successful multidisciplinary treatment with coiling, pseudoaneurysm excision, debridement, and plastic reconstruction Vascular Specialist International 202036426826910.5758/vsi.20008233408293 PMC 7790700 · doi ↗ · pubmed ↗
- 7Kuhnt T. Mueller A. C. Pelz T. Impact of tumor control and presence of visible necrosis in head and neck cancer patients treated with radiotherapy or radiochemotherapy Journal of Cancer Research and Clinical Oncology 20051311175876410.1007/s 00432-005-0018-z 2-s 2.0-2764453497716088405 PMC 12161190 · doi ↗ · pubmed ↗
- 8Chen C. T. Lin Y. H. Chen Y. F. Lee C. W. Lee B. C. Air-containing necrosis as the imaging predictor for imminent carotid blowout in patients with head and neck cancer Journal of the Formosan Medical Association 202212171266127210.1016/j.jfma.2021.09.00634593274 · doi ↗ · pubmed ↗