Case of Immune Checkpoint Inhibitor Induced Myasthenia Gravis
Manoja Gullapalli, Narenraj Arulprakash, Mazin Safar, Emily Kocurek

TL;DR
An 85-year-old man with liver cancer developed myasthenia gravis-like symptoms after treatment with immune checkpoint inhibitors, highlighting the need for early recognition of such side effects.
Contribution
This case report highlights ICI-induced myasthenia gravis as a rare but important neurotoxicity to recognize in cancer treatment.
Findings
The patient developed myasthenic symptoms and respiratory failure after ICI treatment.
Immune suppression led to recovery, supporting the ICI toxicity diagnosis.
Aseptic meningitis in cerebrospinal fluid analysis further supported the diagnosis.
Abstract
An 85-year-old man was diagnosed with hepatocellular carcinoma (HCC) and was initially treated with transarterial chemoembolization (TACE) and sorafenib. He was then switched to nivolumab and ipilimumab in view of sorafenib intolerance and disease progression. Subsequently, he developed dysphagia and generalized dyspnea culminating in hypercapnic respiratory failure requiring intubation. After an extensive workup, the etiology of his fluctuating respiratory issues was narrowed down to a likely neuromuscular process. Although antibodies to acetylcholine receptors (anti-AChR Ab) were negative, he was treated with high-dose steroids due to clinical concern for Immune Checkpoint Inhibitor (ICI) neurotoxicity. His recovery post immune suppression and absence of recurrence after ICI cessation suggested the possibility of this being an ICI neurotoxicity manifesting with myasthenic symptoms.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
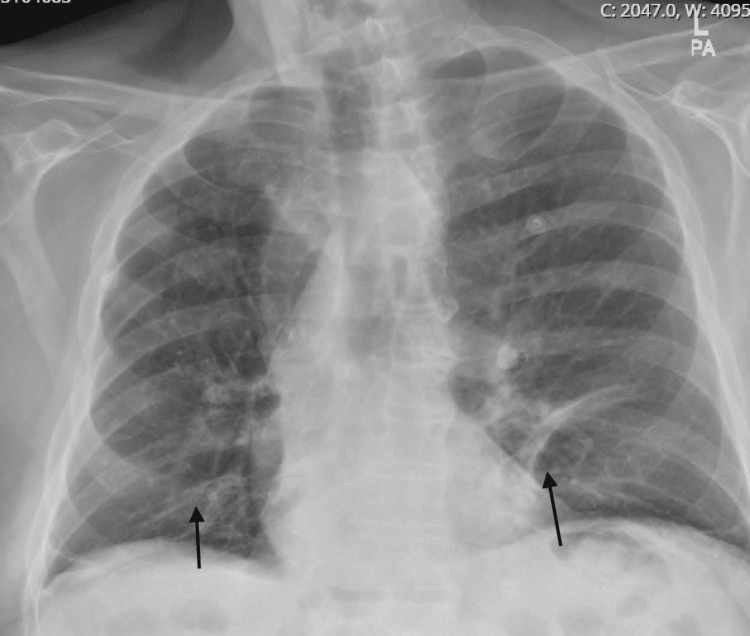 Figure 1
Figure 1| Pre-treatment | Post-treatment | |
| NIF | -49 | -38 |
| VC | 1.78 | 3.48 |
| CSF lab | Value |
| Protein mg/dL | 73 |
| CSF Glucose mg/dL | 86 |
| WBCs/ | 25 |
| RBCs/ | 0 |
| Gram Stain | Negative |
| CSF culture | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Brain Metastases and Treatment · Myasthenia Gravis and Thymoma
Introduction
Immune checkpoints are a normal part of the immune system and function to prevent immune response against normal healthy cells via inhibiting T cell responses. Cancer cells can use immune checkpoints to evade detection, and monoclonal antibodies that block immune checkpoints are a breakthrough in cancer therapeutics. Programmed death-1 receptor (PD-1), ligand (PDL-1), and cytotoxic T-lymphocyte antigen-4 (CTLA-4) are relatively well studied. T-cell modulators, CTLA4 blockade antibodies (ex: ipilimumab), and anti-PD1/PDL1 (ex: nivolumab) are some of the most widely used anti-tumor ICI agents [1-4]. The increased use of ICIs in the last decade has revealed the potential for systemic side effects, including severe adverse effects on the nervous system, and myasthenia gravis is a rare presentation of ICI neurotoxicity [5-8]. ICI-related Myasthenia Gravis (MG) has been reported to be the most common neuromuscular immune-related adverse event, and ICI-related MG appears to cause respiratory weakness more frequently than classical MG [7]. With ICI-related immune complications, cases have been reported to be associated with autoimmune conditions, and presentation is different compared to the typical presentation of autoimmune conditions. With high clinical suspicion, the diagnosis could be made quickly, leading to prompt treatment.
Case presentation
An 85-year-old Caucasian male with hepatocellular carcinoma was initially treated with transarterial chemoembolization (TACE) and sorafenib. He subsequently received 19 cycles of nivolumab after sorafenib intolerance and disease progression. Two months before the presentation, new lung metastases were detected, and he was started on ipilimumab. After receiving his fourth cycle of nivolumab/ipilimumab, he began to have dysphagia and weakness and eventually presented to the hospital with shortness of breath. He was found to be in respiratory failure and started on bilevel-positive airway pressure (BiPAP). Chest x-ray showed atelectatic changes (Figure 1). He was treated for chronic obstructive pulmonary disease (COPD) exacerbation with steroids and antibiotics. His respiratory distress resolved, and he was discharged home within two days. Four days later, he was re-admitted with worsening dyspnea. Shortly, he developed shock and bradycardia with electrocardiography (EKG) showing junctional bradycardia. His troponin was elevated, but his echocardiogram showed a grossly normal ejection fraction. An ICI cardiotoxicity was suspected, and a myocardial perfusion scan was performed which was positive for reversible perfusion defect, but an MRI could not be performed and a biopsy was not pursued [5,6]. His sputum culture showed Pseudomonas aeruginosa. His shock required vasopressor support and pulse dose steroids. On day 4 of hospitalization, he developed respiratory failure and altered mental status requiring emergent intubation. His antibiotic coverage was broadened, and he was given stress-dose steroids. He was extubated but subsequently developed hypercapnic respiratory failure requiring re-intubation. A neurologist was consulted given recurrent episodes of respiratory failure with concern for possible neuromuscular junction disorder causing the weakness. On neurological assessment, the clinical picture was consistent with myasthenia gravis (MG) as evidenced by dysphagia and episodic weakness which included respiratory muscles. The rest of the neurological exam was normal, but his negative inspiratory force (NIF) and vital capacity (VC) were low (Table 1). CSF findings were concerning for aseptic meningitis (Table 2). Myasthenia antibodies resulted in negative as well. Inflammatory myopathy (anti-Jo 1) and AIDP (anti-GM1 Abs). Due to clinical concern for ICI neurotoxicity, methylprednisolone was initiated (1 g intravenously daily for five days) [2,7]. Ultimately the clinical picture was thought to be most consistent with seronegative MG [7,9]. Since the patient exhibited fluctuating weakness, other causes including inflammatory myopathy and acute inflammatory demyelinating polyradiculoneuropathy were considered less likely. The patient showed remarkable recovery in his respiratory function and dysphagia with steroids, and his NIF and VC improved as well (Table 1). He was successfully extubated after four days of steroid treatment and transferred to the floor. He was stable for the remainder of his stay and, at follow up, he reported no further issues with swallowing or respiration. Since he was asymptomatic at a follow-up clinic appointment off of any medications, the plan was to follow him clinically without starting long-term immunosuppression.
Chest x-ray with subsegmental atelectasis in the lung bases in the setting of acute respiratory failure.
Discussion
ICI neurotoxicity is known to cause an array of symptoms involving the brain, spinal cord, nerves, and neuromuscular junction. Manifestations include aseptic meningitis, autoimmune encephalitis, Guillain-Barre syndrome, MG and inflammatory myopathy among others [1-4]. The diagnosis of neurological complications associated with ICIs is usually challenging as these disorders are usually a diagnosis of exclusion. The incidence of myasthenia gravis due to ICI neurotoxicity is estimated to be approximately 0.1%-0.2% [1]. ICI-MG tends to occur in men with a median age of 70. Symptoms are most commonly noted two to 12 weeks after ICI initiation [1]. The anti-PD-1 treatment appears to cause myasthenia gravis more often than other ICIs. Patients often present with fluctuating muscular weakness involving bulbar, ocular, and even respiratory muscles, sometimes associated with axial and proximal limb weakness and/or severe dyspnea. The coexistence of myasthenia gravis and myositis frequently occurs, and this coexistence is a risk factor for the myasthenic crisis that requires intensive care [6,7]. Corticosteroids are generally used as a first therapy when other possible causes are eliminated. Patients may develop immune-related toxicities simultaneously in other organ systems. For example, cases of ICI-related MG coinciding with myositis or myocarditis have been described [5,6]. Anti-acetylcholinesterase receptor or anti-striated muscle antibodies were positive in only about 66% of ICI-related MG cases, and 60% of patients demonstrated electrodiagnostic evidence of MG or myositis [7].
Conclusions
Seronegativity is reported to be higher in ICI-related MG than in classic MG. Practitioners should monitor for autoimmune adverse effects associated with ICIs closely since presentations could be atypical. Gathering and describing the clinical and serologic characteristics of a larger cohort of patients with ICI-related MG would be beneficial in order to clarify the unique features of this ICI neurotoxicity and potentially facilitate earlier diagnosis. Efforts to store sera of afflicted patients should be encouraged to enable future research focused on the development of more precise diagnostic testing and targeted therapy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Immune checkpoint inhibitors and neurotoxicity Curr Neuropharmacol Zhao Z Zhang C Zhou L Dong P Shi L 124612631920213338030310.2174/1570159 X 19666201230151224 PMC 8719293 · doi ↗ · pubmed ↗
- 2Clinical characteristics and treatment of immune-related adverse events of immune checkpoint inhibitors Immune Netw Choi J Lee SY 020202010.4110/in.2020.20.e 9PMC 704958632158597 · doi ↗ · pubmed ↗
- 3Immune-related adverse events associated with immune checkpoint blockade N Engl J Med Postow MA Sidlow R Hellmann MD 15816837820182932065410.1056/NEJ Mra 1703481 · doi ↗ · pubmed ↗
- 4Toxicities associated with checkpoint inhibitors-an overview Rheumatology (Oxford) Spiers L Coupe N Payne M 058201910.1093/rheumatology/kez 418PMC 690091731816085 · doi ↗ · pubmed ↗
- 5Checkpoint inhibitor-induced myocarditis and myasthenia gravis in a recurrent/metastatic thymic carcinoma patient: a case report Eur Heart J Case Rep Szuchan C Elson L Alley E 184202010.1093/ehjcr/ytaa 051PMC 731980532617460 · doi ↗ · pubmed ↗
- 6The terrible triad of checkpoint inhibition: a case report of myasthenia gravis, myocarditis, and myositis induced by cemiplimab in a patient with metastatic cutaneous squamous cell carcinoma Case Reports Immunol Jeyakumar N Etchegaray M Henry J Lelenwa L Zhao B Segura A Buja L Mu 5126717202020203269553310.1155/2020/5126717 PMC 7355354 · doi ↗ · pubmed ↗
- 7Immune checkpoint inhibitor-induced myasthenia gravis Front Neurol Huang YT Chen YP Lin WC Su WC Sun YT 6341120203276539710.3389/fneur.2020.00634 PMC 7378376 · doi ↗ · pubmed ↗
- 8Immune checkpoint inhibitor related myasthenia gravis: single center experience and systematic review of the literature J Immunother Cancer Safa H Johnson DH Trinh VA 319720193175301410.1186/s 40425-019-0774-y PMC 6868691 · doi ↗ · pubmed ↗