Persistent pneumothorax after laparoscopic appendectomy in a patient who had undergone radical esophagectomy 5 years before: possible relationship with vulnerability of the hiatus after esophagectomy: a case report
Seiji Ishikawa, Masakazu Hayashida, Daizo Satoh, Shinji Mine, Izumi Kawagoe

TL;DR
A patient with a history of esophagectomy developed a persistent pneumothorax after laparoscopic surgery, possibly due to anatomical vulnerability.
Contribution
Highlights a possible link between prior esophagectomy and increased risk of pneumothorax after laparoscopic procedures.
Findings
A patient with a history of esophagectomy developed a persistent pneumothorax after laparoscopic appendectomy.
The pneumothorax resolved spontaneously after more than three days.
The anatomical vulnerability from prior surgery may allow air migration into the thoracic cavity.
Abstract
Postoperative pneumothorax is a well-known but relatively rare complication after laparoscopic surgery. Herein, we report a case of persistent pneumothorax after laparoscopic appendectomy. A 57-year-old male, with a history of minimally invasive esophagectomy and intrathoracic gastric tube reconstruction 5 years before, underwent a laparoscopic appendectomy. A chest X-ray taken on postoperative Day 1 revealed the development of the right pneumothorax, which took more than 3 days to resolve spontaneously. Although the mechanism of postoperative pneumothorax was unclear, it seemed likely that the air that had replaced carbon dioxide in the peritoneal cavity migrated into the thoracic cavity through the esophageal hiatus, which was not covered by the peritoneum or pleura after surgical resection. The present case, together with our previous similar case, suggests that a history of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
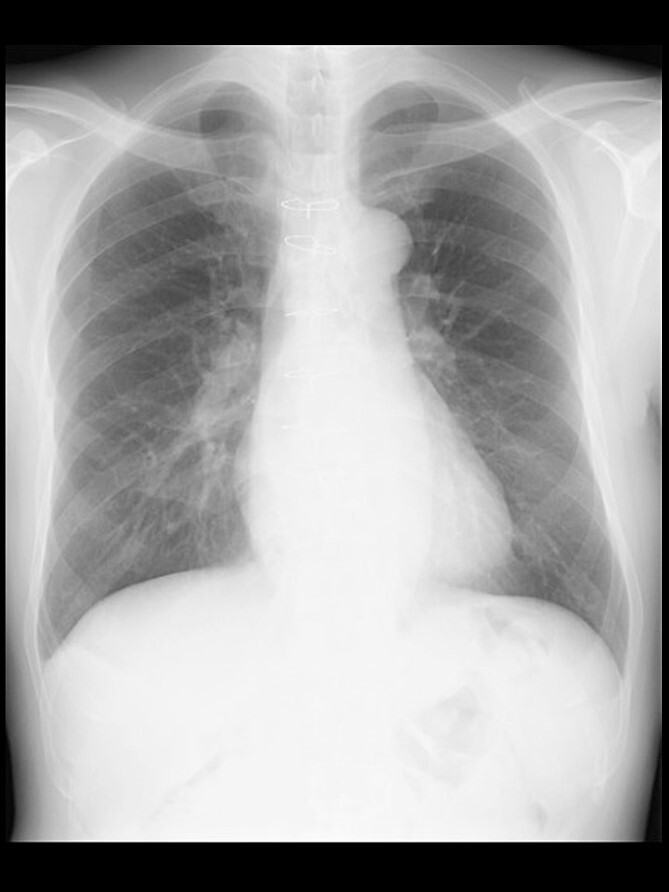 Figure 1
Figure 1 Figure 2
Figure 2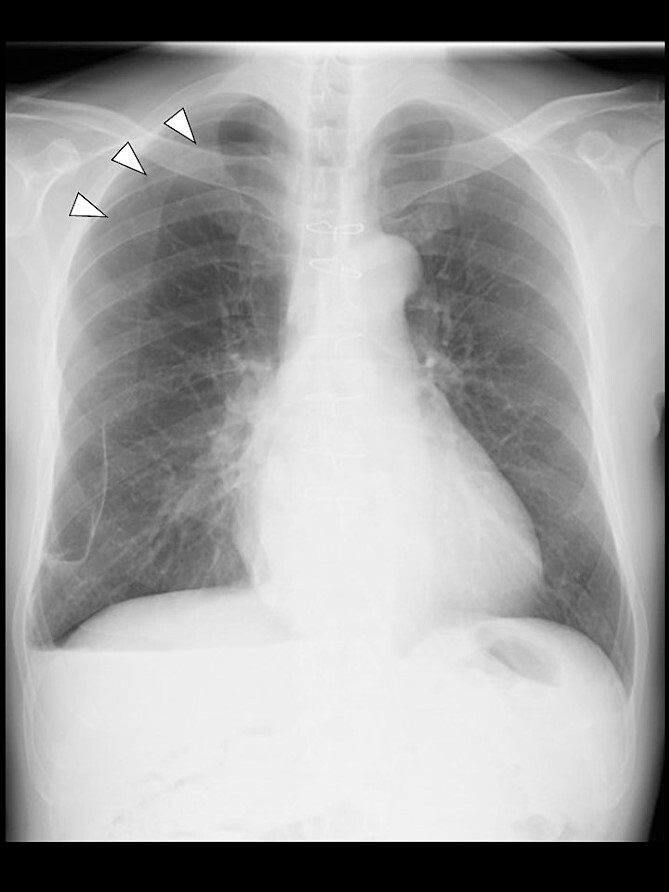 Figure 3
Figure 3- —Ministry of Education, Culture, Sports, Science and Technology10.13039/501100001700
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Abdominal Surgery and Complications · Esophageal and GI Pathology
Introduction
Pneumothorax after laparoscopic surgery is a well-known but relatively rare complication, with a reported frequency of 0.01%–1.9% [1–3]. We previously reported a case of pneumothorax that developed after laparoscopic surgery and persisted for more than a week in a patient who had undergone esophagectomy 4 months earlier, and concluded that esophagectomy, at least performed recently, may increase the risk of pneumothorax after laparoscopic surgery [4]. After the presentation of the previous case [4], we experienced a similar case.
Herein, we report another case of persistent pneumothorax after laparoscopic surgery in a patient who had undergone esophagectomy, but much earlier than 4 months. This case suggests that a history of esophagectomy per se can increase the risk of pneumothorax after laparoscopic surgery, regardless of when esophagectomy was performed.
Case report
A 57-year-old male, 178 cm and 69 kg, was scheduled for a laparoscopic appendectomy for chronic appendicitis. The patient had undergone mitral valve repair for infective endocarditis via a median sternotomy 16 years before and minimally invasive esophagectomy (MIE) with intrathoracic anastomosis using a gastric tube for esophageal cancer 5 years before. Preoperative tests, including a chest radiograph (Fig. 1), were unremarkable. The computed tomography (CT) revealed no emphysematous lung cyst. Anesthesia was induced with intravenous remifentanil (0.3 μg/kg/min) and propofol (100 mg). Intravenous rocuronium (50 mg) was administered to facilitate tracheal intubation. Anesthesia was maintained with inhaled sevoflurane (1.5%) and intravenous remifentanil (0.1–0.3 μg/kg/min). The lungs were ventilated with a volume-guarantee pressure-controlled mode employing an inspired oxygen concentration of 35%. Percutaneous arterial oxygen saturation (SpO_2_) was maintained at 96%–100%. In addition to local anesthetic wound infiltration, intravenous fentanyl (300 μg) and acetaminophen (1000 mg) were administered for immediate postoperative analgesia. Operation and anesthesia times were 121 and 156 min, respectively. The infusion volume was 1350 ml. Emergences from anesthesia and extubation were uneventful. SpO_2_ in the postanesthesia care unit was maintained above 95% without supplemental oxygen. The patient did not complain of chest pain or dyspnea.
A chest radiograph in the upright position before surgery.
Even though the patient did not receive supplemental oxygen in the ward, SpO_2_ remained at 98%. Chest radiographs were not taken on the day of surgery. However, a chest radiograph taken in the upright position on postoperative Day (POD) 1 revealed a pneumothorax on the right side (Fig. 2), although he had no respiratory symptoms. Radiographs on PODs 2 and 3 revealed the pneumothorax remaining unchanged (Fig. 3). The patient was discharged from the hospital on POD 3 without any respiratory symptoms. A chest radiograph taken on POD 19 showed no remaining pneumothorax.
A chest radiograph in the upright position on POD 1 showing a right pneumothorax (arrowheads).
A chest radiograph in the upright position on POD 3 showing a residual right pneumothorax (arrowheads).
Discussion
Most pneumothorax after laparoscopic surgery occurs during or immediately after surgery and disappears quickly without the need for specific treatment [5, 6]. Until our previous case report was published [4], only one report and no report had described pneumothorax becoming evident the day after laparoscopic surgery [7] and pneumothorax persisting for days after laparoscopic surgery, respectively.
Known mechanisms of pneumothorax after laparoscopic surgery include iatrogenic damage to the diaphragm [8], rupture of a bulla, and migration of carbon dioxide into the thoracic cavity through subcutaneous emphysema [9]. However, none of these mechanisms seemed applicable to our case, as no bulla was detected preoperatively, the diaphragm was not surgically manipulated, or no subcutaneous emphysema was observed perioperatively.
Similarly to our previous case [4], a pneumothorax was evident after laparoscopic surgery on POD 1 and persisted for days. The long-lasting pneumothorax suggested that the gas trapped in the thoracic cavity was air rather than carbon dioxide [4]. Although the precise mechanism of postoperative pneumothorax in this case was unclear, it seemed likely that the intraabdominal gas migrated into the thoracic cavity through the esophageal hiatus not covered by the peritoneum nor pleura, as esophagectomy and conduit reconstruction involve a large incision in the pleura adjacent to the esophagus and a partial incision in the peritoneum covering the diaphragm. These procedures should leave a transdiaphragmatic communication between abdominal and thoracic cavities, as could be suggested by developments of postesophagectomy diaphragmatic hernias (PEDHs) as an extreme manifestation of this communication, with a reported frequency of 0.7%–19.6% [10].
It is expected that a transdiaphragmatic communication via a hiatal or peri-conduit route would gradually close owing to tissue adhesion, since PEDHs most frequently develop within 2 years after esophagectomy, and thereafter, their occurrences decrease with the elapse of time [11, 12]. However, PEDHs can occur several years after esophagectomy in a proportion of patients [11, 12], and even more than 10 years after esophagectomy [13]. Further, an increase in intraabdominal pressure can cause a sudden PEDH by reopening a previously closed transdiaphragmatic communication [14]. Because a major transdiaphragmatic communication allowing migration of abdominal organs can persist or reopen several to more than 10 years after esophagectomy [11–13], a minor transdiaphragmatic communication allowing migration of the intraabdominal gas would persist much longer and much more frequently and/or would be much more easily reopened by increased intra-abdominal pressure from pneumoperitoneum. Indeed, the present case suggests that even 5 years after esophagectomy, gas migration can occur following laparoscopic surgery. Further, it should be noted that our previous [4] and present patients had undergone MIE, given that the incidence of PEDHs is higher after MIE than after open esophagectomy (6.5% vs. 2.4%) [15].
The above-mentioned data regarding PEDHs and our previous and present cases of persistent pneumothorax after laparoscopic surgery in postesophagectomy patients suggest that a history of esophagectomy, especially that of MIE can increase the risk of pneumothorax after laparoscopic surgery, regardless of the time elapsed since esophagectomy. Clinicians should be aware of the possible development of persistent pneumothorax after laparoscopic surgery in postesophagectomy patients.
In conclusion, the present case suggests that a history of esophagectomy, especially that of MIE can increase the risk of pneumothorax after laparoscopic surgery regardless of the time after esophagectomy, although further studies are required to elucidate whether previous esophagectomy actually increases the risk of pneumothorax after laparoscopic surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prystowsky JB , Jericho BG, Epstein HM. Spontaneous bilateral pneumothorax – complication of laparoscopic cholecystectomy. Surgery 1993;114:988–92.8236025 · pubmed ↗
- 2Dawson R , Ferguson CJ. Life-threatening pneumothorax during laparoscopic cholecystectomy. Surg Laparosc Endosc 1997;7:271–2. 10.1097/00019509-199706000-00022.9194296 · doi ↗ · pubmed ↗
- 3Murdock CM , Wolff AJ, Van Geem T. Risk factors for hypercarbia, subcutaneous emphysema, pneumothorax and pneumomediastinum during laparoscopy. Obstet Gynecol 2000;95:704–9.10775733 10.1016/s 0029-7844(00)00781-x · doi ↗ · pubmed ↗
- 4Ishikawa S , Shirakawa K, Kuroda Y, et al. Persistent bilateral pneumothorax after robotic-assisted inguinal hernia repair: possible relevance to recent esophageal cancer surgery – a case report. JA Clin Rep 2023;9:37. 10.1186/s 40981-023-00630-y.37347313 PMC 10287872 · doi ↗ · pubmed ↗
- 5Bartelmaos T , Blanc R, De Claviere G, Benhamou D. Delayed pneumomediastinum and pneumothorax complicating laparoscopic extraperitoneal inguinal hernia repair. J Clin Anesth 2005;17:209–12. 10.1016/j.jclinane.2004.05.009.15896590 · doi ↗ · pubmed ↗
- 6Wu Q , Zhang H. Carbon dioxide pneumothorax following retroperitoneal laparoscopic partial nephrectomy: a case report and literature review. BMC Anesthesiol 2018;18:202. 10.1186/s 12871-018-0662-x.30579345 PMC 6303981 · doi ↗ · pubmed ↗
- 7Mekaru K , Yagi C, Uezato T, et al. Delayed pneumothorax after laparoscopic ovarian cystectomy. Arch Gynecol Obstet 2009;280:157–9. 10.1007/s 00404-008-0866-2.19082835 · doi ↗ · pubmed ↗
- 8Han Q , Wang B, Xu A. Use of intraoperative ultrasonography for identification and management of pneumothorax caused by iatrogenic diaphragm defect: a case report and literature review. J Int Med Res 2020;48:300060519898048. 10.1177/0300060519898048.31964200 PMC 7113711 · doi ↗ · pubmed ↗