Sezary Syndrome: A Case Report and Review of Current Therapeutics
Jayasree Krishnan, Kannan Thanikachalam

TL;DR
This paper discusses a case of Sezary Syndrome, a rare skin cancer, and highlights the importance of early diagnosis and treatment.
Contribution
The paper presents a new case report and emphasizes the need for early referral to dermatology for suspected Sezary Syndrome.
Findings
A patient with Sezary Syndrome showed a good response to systemic therapy with bexarotene.
Persistent rashes unresponsive to treatment may indicate Sezary Syndrome and require dermatological evaluation.
Abstract
Sezary syndrome (SS) is a rare but aggressive type of cutaneous T-cell lymphoma (CTCL). Patients with SS have characteristic skin lesions (erythroderma) and a leukemic phase. The rash associated with CTCLs can often mimic common benign skin conditions such as psoriasis, atopic dermatitis, etc. and therefore can go undiagnosed until later stages. We present a case of a patient with SS who managed eczema for over one year with topical steroids before receiving a skin biopsy. Workup confirmed leukemic involvement, and the patient was started on systemic therapy with bexarotene. The patient continues to have a good response to systemic therapy. When treating patients with persistent rash of uncertain etiology and/or unresponsive to treatment, primary care physicians and internists need to consider SS/Mycosis fungoides as a possible differential and should have a low threshold to initiate…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2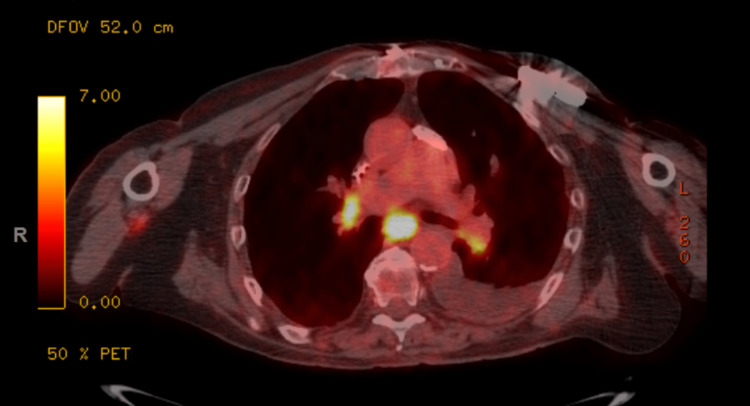 Figure 3
Figure 3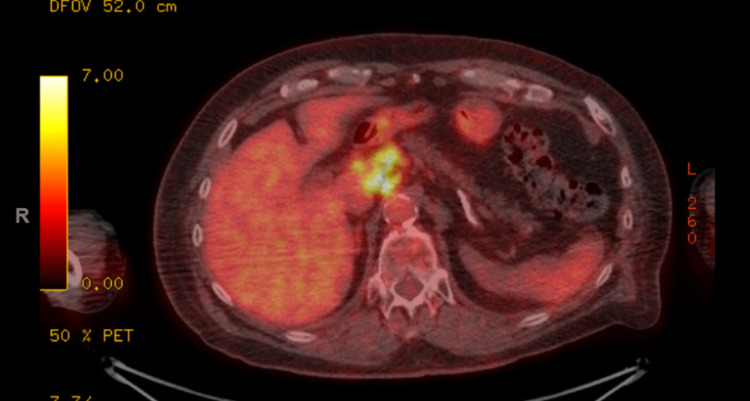 Figure 4
Figure 4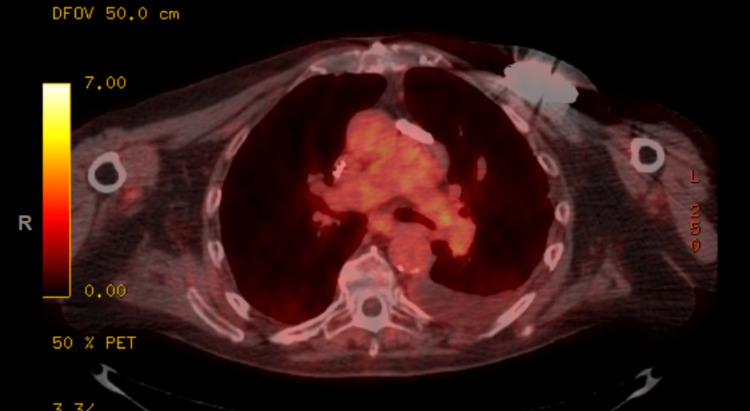 Figure 5
Figure 5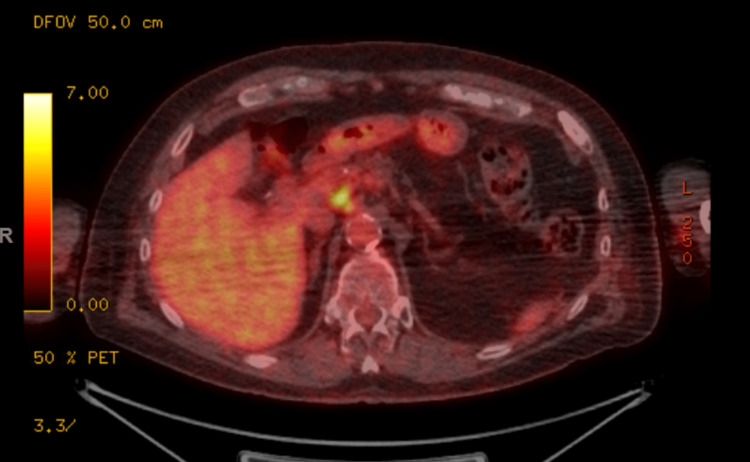 Figure 6
Figure 6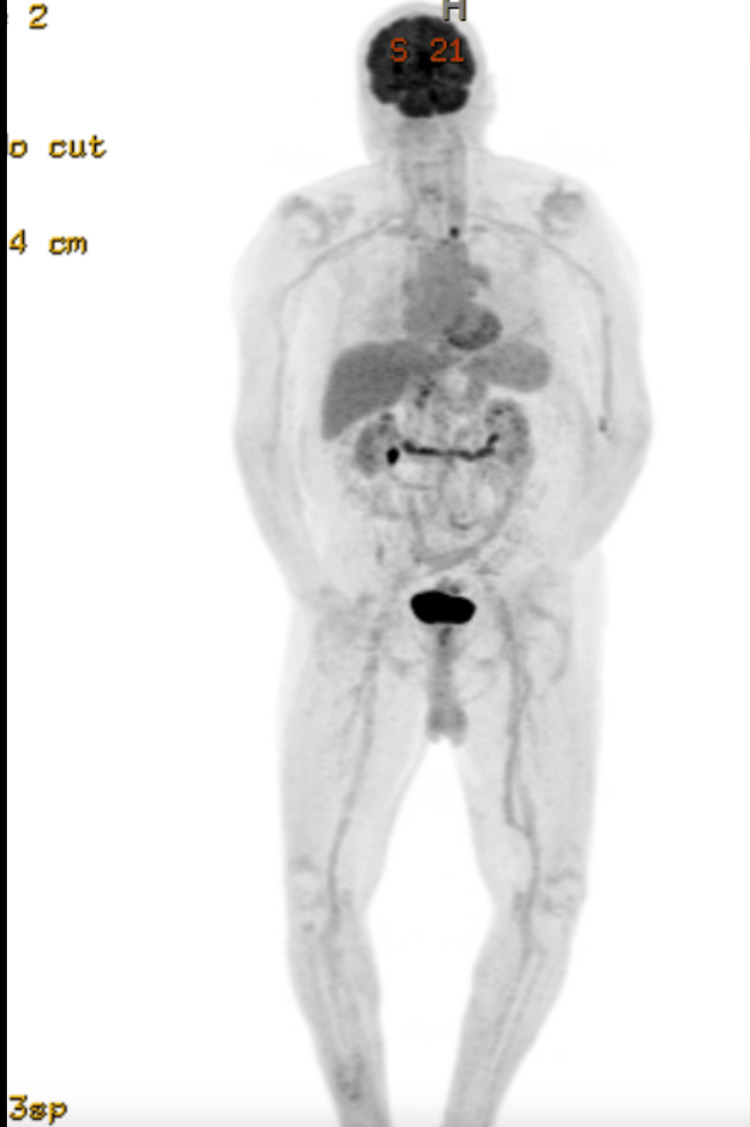 Figure 7
Figure 7 Figure 8
Figure 8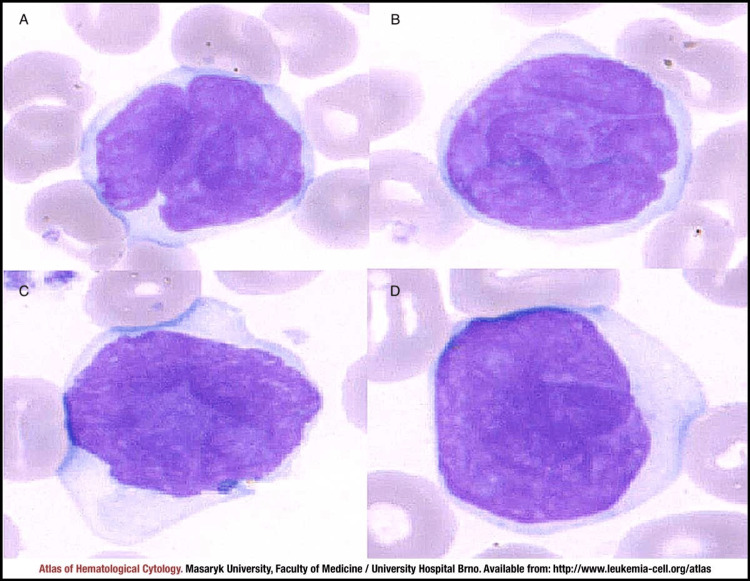 Figure 9
Figure 9Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCutaneous lymphoproliferative disorders research · Nail Diseases and Treatments · Fungal Infections and Studies
Introduction
Cutaneous T-cell lymphomas (CTCLs) are a rare group of lymphomas that primarily involve the skin. Mycosis fungoides (MF) is the most common type of CTCL accounting for approximately 57% of CTCLs [1]. MF presents with localized or widespread skin lesions (patch, plaque, or tumor) and in some cases, lymph nodes, blood, and viscera may also be involved [2]. Sezary syndrome (SS) is a rare type of CTCL characterized by erythroderma, generalized lymphadenopathy, and clonally related malignant T-cells in the skin and peripheral blood [2]. The incidence of SS/MF increases with age with the majority of cases over 40 years of age [1,2]. In the United States, the incidence is higher in men, non-Hispanic black patients, individuals in high socioeconomic status quintiles, and people living in metropolitan counties [1].
MF/SS can be challenging to diagnose since the skin lesions mimic inflammatory skin diseases like eczema and psoriasis, especially at an early stage. Increased awareness among physicians and education on heterogeneous presentation of this disease can lead to expedited specialist referrals and prompt diagnosis. Patients with early-stage MF/SS have favorable prognosis so early diagnosis and treatment are crucial to decrease the risk of progression and improve outcomes [3].
Case presentation
Our patient is a 79-year-old Caucasian gentleman with a past medical history of hypertension, hyperlipidemia, history of cardiac arrest from ventricular fibrillation s/p AICD requiring prolonged hospitalization who presented with a pruritic erythematous rash (Figure 1) all over his body. He was never diagnosed with any dermatological condition in the past. He denied any personal history or family history of malignancy. He is a former light smoker with five packs a year smoking history, with no alcohol use or recreational drug use. He had no drug or environmental allergies. On examination, the patient's vital signs were normal, with a temperature of 98.8, a heart rate of 90 beats/min, a respiratory rate of 18 breaths/min, and a blood pressure of 134/82. Cardiovascular, pulmonary, abdominal, and neurological exams were normal. Examination of the lymphatic system did not reveal any lymphadenopathy. A dermatological examination revealed an erythematous macular rash all over his body, predominantly in his chest, trunk, and lower extremities. Though he did not have any known history of eczema, given his pruritic nature, his erythematous rash was managed as possible eczema for nearly 1.5 years with topical steroids of varying strength by his primary care physician without any significant improvement in symptoms. The patient was subsequently referred to dermatology who performed a skin biopsy of epigastric skin lesion that came back as atypical T-cell infiltrate, consistent with MF. By Immunohistochemistry (IHC), the cells were uniformly positive for CD3 with a CD4: CD8 ratio of greater than 10-1 and diminished CD7 expression. CD20 stains showed rare, scattered cells. He was then referred to hematology for further evaluation. Peripheral blood flowcytometry showed an abnormal T cell population involving 26% of total leukocytes (CD45+, CD1a-, CD2+, sCD3+, CD4+, CD5+, CD7 -/+, CD8-, CD10-, CD11b-, CD11c-, CD13-, CD14-, CD16-, CD19-, CD20-, CD25 -/+, CD26-, CD30-, CD34-, CD38-/+, CD52+, CD56-, CD57-, CD103-, CD117-, TCRGD-, TRBC1+). The absolute Sezary cell count was 2.8K/mm^3^, consistent with low-intermediate burden disease.
Erythematous skin rash in the chest wall before treatment
He underwent evaluation with bone marrow biopsy, positron emission tomography (PET) scan, and T-cell receptor (TCR) gene rearrangement clonality. Bone marrow biopsy showed normocellular bone marrow for age with trilineage hematopoiesis but with low-level involvement by SS. TCR gene rearrangement showed gamma chain clonal rearrangement. His PET scan showed 18F-fluorodeoxyglucose (FDG) avid lymphadenopathy in the mediastinum, hilar, and upper abdomen (Figures 2-4). Biopsy of FDG avid lymph nodes was not obtained given his advanced age, and comorbidities, and medical decision was made to monitor his response to therapy on subsequent imaging. Human T-cell lymphotropic virus (HTLV) serology was negative.
PET scan showing FDG avid lymphadenopathy in the mediastinum, hilar, and upper abdomenPET: Positron emission tomography; FDG: 18F-fluorodeoxyglucose
FDG-avid lymphadenopathy in the mediastinumFDG: 18F-fluorodeoxyglucose
FDG-avid lymphadenopathy in the upper abdomenFDG: 18F-fluorodeoxyglucose
The patient was diagnosed with SS, stage IVA1 T4N3M0, B2 disease. He was started on systemic bexarotene, a retinoid, given low systemic toxicity and also received topical triamcinolone 0.05% cream for skin-directed therapy. The patient developed hypertriglyceridemia and hypothyroidism as a side effect of bexarotene which responded to an increase in the dose of atorvastatin and initiating low-dose levothyroxine respectively. He also experienced mild diarrhea which was well controlled with Imodium as needed. PET scan was repeated in two months after initiating treatment, which showed improvement in size and metabolic uptake (Figures 5-7). The largest intra-abdominal decreased in size from 2.3 cm to 1.7 cm with a decrease in the standardized uptake value (SUV) from 14.7 to 4.7. The largest mediastinal lymph node decreased in size from 3 cm to 1.2 cm with a decrease in SUV from 16 to 2. His skin rash improved with treatment as well (Figure 8). He remains stable without disease progression, after five months of bexarotene therapy.
Interval improvement in FDG-avid mediastinal lymphadenopathy after two months of bexarotene treatmentFDG: 18F-fluorodeoxyglucose
Interval improvement in FDG-avid abdominal lymphadenopathy after two months of bexarotene treatmentFDG: 18F-fluorodeoxyglucose
Radiological response after two months of treatment with bexarotene
Improvement in erythematous skin rash one month after treatment
Discussion
SS and MF are the most common types of cutaneous T-cell lymphomas. The overall incidence of CTCL was 8.55 per million according to the data from the Surveillance, Epidemiology, and End Results (SEER) program from 2000 to 2018 which has increased from 6.4 per million persons during the period 1973-2002 [1,4]. The annual percentage change of CTCL was highest in Sezary syndrome with an increase of 3.83% during this period [1]. An increase in incidence is postulated due to better diagnostic tools and increased physician awareness however diagnostic delay persists due to the indolent nature of the disease, heterogeneous, nonspecific skin manifestations mimicking benign inflammatory dermatosis such as psoriasis, eczema, lichenoid dermatoses, etc.., leading to misdiagnosis. One study reported a mean diagnostic delay of 4.2 years overall with a delay of five years in patients without erythroderma at the initial visit [5].
The exact etiology of SS is unclear; however human T-lymphotropic viruses type 1 and 2 (HTLV-I/II) have been identified as a risk factor. Certain medications that may induce an antigen-driven T-cell lymphoproliferation or dyscrasia could serve as a trigger for MF [6]. SS may arise de novo or may precede MF. The diagnosis of SS is usually based on clinical, histopathological, and molecular findings. Since the skin and/or lymph node biopsy findings can be nonspecific and often not confirmatory but only suspicious for SS, the International Society for Cutaneous Lymphomas (ISCL) has proposed strict hematologic criteria to avoid misdiagnosis [7]. Sezary cells are characterized by variable amounts of non-granular cytoplasm along with the characteristic convoluted to cerebriform nuclei (Figure 9). The criteria for SS diagnosis require generalized erythroderma and the following hematologic criteria: 1. An absolute Sézary cell count of 1000 cells/mm^3^ or more 2. A CD4/CD8 ratio of 10 or more due to an increase in CD3+ or CD4+ cells by flow cytometry 3. Aberrant expression of pan-T cell markers (CD2, CD3, CD4, CD5) by flow cytometry. Deficient CD7 expression on T cells (or expanded CD4+CD7- cells ≥ 40%) represents a tentative criterion of SS at this time. 4. Increased lymphocyte counts with evidence of a T-cell clone in the blood by Southern blot or PCR technique 5. A chromosomally abnormal T-cell clone. ISCL recommends that patients without erythroderma but with blood findings of SS should not be diagnosed as having SS and instead be designated as MF with leukemic involvement.
Peripheral blood smear of Sezary syndromeA-D: Typical morphology of Sezary cells with cerebriform nuclei [8]
Patients with a definitive diagnosis of MF/SS are classified based on the TNMB (tumor, node, metastasis, blood) staging system proposed by ISCL/EORTC (The European Organization for Research and Treatment of Cancer) [9]. The treatment for MF/SS should involve a multidisciplinary treatment team with hematology, dermatology, pathology, and radiation oncology. Due to the rarity of malignancy, patients with Sezary syndrome should be seen in a tertiary care referral center. Patients with limited-stage MF have an excellent prognosis and can be treated with several options including Involved site radiation therapy, phototherapy with ultraviolet (UV), topical corticosteroids, topical retinoids, topical imiquimod, and total skin electron beam therapy [10]. Skin-directed therapies can be offered alone or in combination with other therapies. In advanced stages with skin erythroderma, or with SS, treatment often involves systemic therapy used in combination with skin-directed therapies.
There are several systemic therapy options for advanced MF/SS including bexarotene, brentuximab, methotrexate, mogamulizumab, romidepsin, alemtuzumab, pembrolizumab, pralatrexate, vorinostat, gemcitabine, and liposomal doxorubicin [10,11]. In a trial of physician choice therapy (bexarotene or methotrexate) vs Brentuximab vedotin in CD-30 positive CTCLs, Brentuximab vedotin, antibody-drug conjugate against CD-30, had a superior response rate when compared to physician choice therapy (56.3% vs 12.5%) [12]. In patients with previously treated MF/SS, Mogamulizumab, a recombinant humanized monoclonal antibody against chemokine receptor 4 (CCR-4) had significantly higher progression-free survival over Vorinostat, a histone deacetylase inhibitor - 7.7 months vs 3.1 months [13]. Pembrolizumab, a monoclonal antibody against PD-1 has shown significant anti-tumor activity in heavily pretreated relapsed/refractory MF/SS with an overall response rate of 38%, with a significant durable response [14]. Clinical trial participation should always be strongly encouraged.
Bexarotene is a synthetic retinoid that selectively activates the retinoid X receptor (RXR). It was FDA-approved for the treatment of CTCL in 1999. We chose bexarotene as the initial therapy for our patient due to the patient’s advanced age and to limit potential side effects from systemic chemotherapy. The most common toxicities associated with bexarotene are hypertriglyceridemia and central hypothyroidism. Myelosuppression is an uncommon side effect. Our patient experienced both hypertriglyceridemia and hypothyroidism but was successfully managed with dose adjustment of statin and thyroid hormone supplementation.
Conclusions
Though differential diagnosis for pruritic erythematous skin rash is wide, comprising both benign and malignant etiology, any persistent skin rash that is unresponsive to conservative management should raise suspicion for cutaneous malignancies including cutaneous lymphoma. Prompt diagnosis and early treatment of cutaneous lymphomas will improve outcomes including overall survival. Primary care physicians should have a high index level of suspicion for atypical symptoms including persistent skin rash and should evaluate for other systemic B symptoms, leading to timely diagnosis. Patients with rare cutaneous lymphomas such as SS should be evaluated in tertiary care centers for a multidisciplinary treatment approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence trends of primary cutaneous T-cell lymphoma in the US from 2000 to 2018: a SEER population data analysis JAMA Oncol Cai ZR Chen ML Weinstock MA Kim YH Novoa RA Linos E 16901692820223604845510.1001/jamaoncol.2022.3236 PMC 9437821 · doi ↗ · pubmed ↗
- 2Mycosis fungoides and Sézary syndrome: clinical presentation, diagnosis, staging, and therapeutic management Front Oncol Miyashiro D Sanches JA 11411081320233712451410.3389/fonc.2023.1141108 PMC 10140754 · doi ↗ · pubmed ↗
- 3Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal J Clin Oncol Agar NS Wedgeworth E Crichton S 473047392820102085582210.1200/JCO.2009.27.7665 · doi ↗ · pubmed ↗
- 4Incidence of cutaneous T-cell lymphoma in the United States, 1973-2002 Arch Dermatol Criscione VD Weinstock MA 85485914320071763872810.1001/archderm.143.7.854 · doi ↗ · pubmed ↗
- 5Early clinical manifestations of Sézary syndrome: a multicenter retrospective cohort study J Am Acad Dermatol Mangold AR Thompson AK Davis MD 7197277720172870969410.1016/j.jaad.2017.05.036 · doi ↗ · pubmed ↗
- 6Drug-induced reversible lymphoid dyscrasia: a clonal lymphomatoid dermatitis of memory and activated T cells Hum Pathol Magro CM Crowson AN Kovatich AJ Burns F 1191293420031261287910.1053/hupa.2003.4 · doi ↗ · pubmed ↗
- 7Update on erythrodermic cutaneous T-cell lymphoma: report of the International Society for Cutaneous Lymphomas J Am Acad Dermatol Vonderheid EC Bernengo MG Burg G 951064620021175695310.1067/mjd.2002.118538 · doi ↗ · pubmed ↗
- 8Atlas of Haematological Cytology 4 2024 2016 http://www.leukemia-cell.org/atlas