Delayed diagnosis of Swyer‐James‐MacLeod syndrome
Matthew T. Donnan, Eli Dabscheck, Belinda R. Miller, Samantha J. Ellis, Matthew T. Naughton

TL;DR
This paper discusses the delayed diagnosis of a rare lung disease, Swyer-James-MacLeod Syndrome, and highlights the importance of recognizing specific imaging signs for early detection.
Contribution
The paper emphasizes the role of imaging in identifying Swyer-James-MacLeod Syndrome for timely diagnosis.
Findings
Imaging findings include unilateral hyperlucency on chest x-ray.
Computed tomography shows hyperlucency, hypovascularity, and expiratory gas trapping.
Early recognition of these imaging features can lead to appropriate management.
Abstract
Swyer‐James‐MacLeod Syndrome is a rare obliterative lung disease typically caused by childhood infection resulting in arrested pulmonary development. Imaging findings include unilateral hyperlucency on chest x‐ray, and hyperlucency, hypovascularity and expiratory gas trapping on computed tomography. Recognition of abnormal imaging can lead to earlier diagnosis and institution of appropriate management. Swyer‐James‐MacLeod Syndrome is a rare obliterative lung disease typically caused by childhood infection resulting in arrested pulmonary development. Imaging findings include unilateral hyperlucency on chest x‐ray, and hyperlucency, hypovascularity and expiratory gas trapping on computed tomography. Recognition of abnormal imaging can lead to earlier diagnosis and institution of appropriate management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
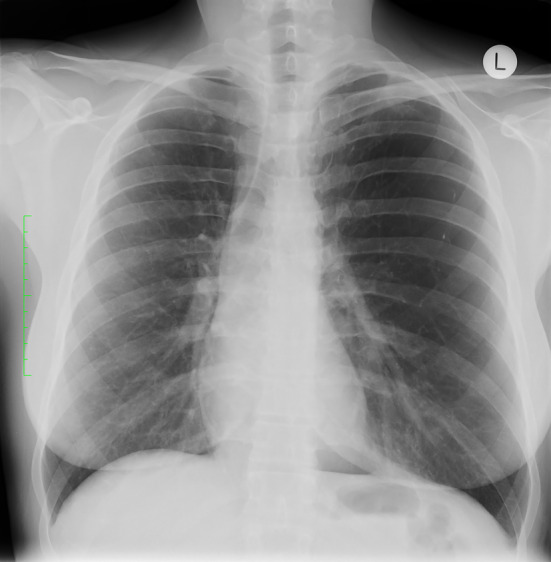 FIGURE 1
FIGURE 1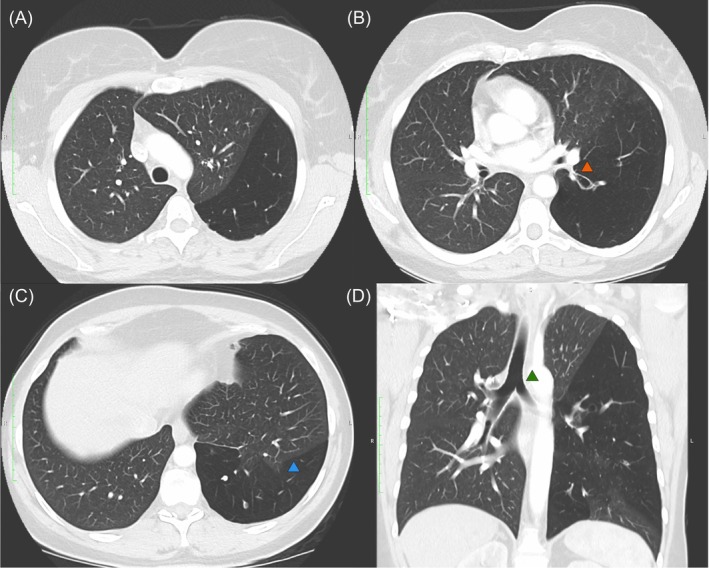 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Diaphragmatic Hernia Studies · Eosinophilic Disorders and Syndromes · Gestational Trophoblastic Disease Studies
CLINICAL IMAGE
A 51‐year‐old woman was referred to respiratory outpatients with 2 years of chronic productive cough. She was a never smoker but had recurrent respiratory infections during childhood, and pneumonia requiring hospitalization in her 20's. Computed tomography (CT) of the chest revealed hyperlucency, hypovascularity and bronchiectasis of the left lower lobe, with stenosis of the left lower lobe bronchus giving rise to Swyer‐James‐MacLeod Syndrome (SJMS). Hyperinflation with mediastinal shift was noted, with an incomplete oblique fissure and associated parenchymal intrusion of the left upper lobe into the left lower lobe. Chest x‐ray 10 years prior revealed left sided hyperlucency with mediastinal shift; no follow‐up had occurred (Figures 1 and 2). Respiratory function tests revealed an obstructive defect (FEV_1_/FVC 0.59) with an FEV_1_ 2.37 L (84% predicted), FVC 4.04 L (114%), and TLCO 23.76 mL/mmHg/min (113%).
Plain chest x‐ray demonstrating left sided hyperlucency and mediastinal shift.
Sagittal and coronal computed tomography images (clockwise from top left; A–D) showing left lower lobe hyperlucency and hypovascularity. (A) demonstrates hyperlucency and hypovascularity of the left lower lobe. (B) demonstrates stenosis at the origin of the left lower lobe bronchus with distal ballooning (orange arrow). (C) demonstrates an incomplete oblique fissure and subsequent parenchymal intrusion into the left lower lobe (blue arrow). In SJMS the volume of the affected lung is normal or, more commonly, reduced. It is seldom if ever increased. In this case collateral air drift through the incomplete fissure is the likely cause of the hyperinflation and subsequent mass effect. (D) demonstrates the degree of mediastinal shift with rightward tracheal deviation (green arrow). Hyperinflation is not typically a feature of SJMS and is often more suggestive of congenital lobar emphysema. If hyperinflation is present, this suggests presence of collateral air flow either from adjacent unaffected lung, or across an incomplete fissure as seen in this case.
SJMS is a rare obliterative lung disease typically caused by childhood infection resulting in arrested pulmonary development.1 Classical CT findings of SJMS include unilateral hyperlucency, hypovascularity and gas trapping on expiratory films.2 Differential diagnoses include an obstructing endobronchial lesion and congenital lobar emphysema. In order not to delay diagnosis and institute appropriate management, an abnormal chest x‐ray should be followed by CT imaging and consideration of bronchoscopy to exclude an endobronchial lesion.2
AUTHOR CONTRIBUTIONS
All authors were involved in patient care. MTD and SE were involved in preparation of the manuscript and images. All authors approved the final manuscript.
CONFLICT OF INTEREST STATEMENT
None declared.
ETHICS STATEMENT
The authors declare that appropriate written informed consent was obtained for the publication of this manuscript and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hamada K , Oishi K , Hirano T , Shiinoki T , Shibuya K , Matsunaga K . Swyer‐James syndrome. Am J Respir Crit Care Med. 2017;197(1):130–131.10.1164/rccm.201708-1691 IM 29064268 · doi ↗ · pubmed ↗
- 2Moore AD , Godwin JD , Dietrich PA , Verschakelen JA , Henderson WR . Swyer‐James syndrome: CT findings in eight patients. Am J Roentgenol. 1992;158(6):1211–1215.1590109 10.2214/ajr.158.6.1590109 · doi ↗ · pubmed ↗