Interstitial Lung Disease With Respiratory Failure After COVID-19 mRNA Vaccination
Soichi Maruyama, Taro Takahashi, Daisuke Kobayashi, Yoneko Hayase, Yukihiko Sugiyama

TL;DR
A woman in her 70s developed lung disease requiring oxygen after her fifth COVID-19 mRNA vaccine dose, showing a rare and persistent reaction.
Contribution
This case highlights a rare post-vaccination interstitial lung disease with unique clinical features and resistance to corticosteroid treatment.
Findings
A chest X-ray showed bilateral diffuse ground-glass opacities after the fifth vaccination.
Lung biopsy revealed alveolar epithelium growth and polypoid granulation tissues.
Corticosteroids were ineffective, leading to persistent fibrosis and long-term oxygen therapy.
Abstract
A septuagenarian woman developed dyspnea on the day following a fifth vaccination. Just before vaccination, a chest X-ray showed no abnormalities, but after the fifth vaccination, bilateral diffuse ground-glass opacities were detected. Bronchoalveolar lavage revealed a lymphocyte predominance and transbronchial lung biopsy revealed growth of the alveolar epithelium, along with organized polypoid granulation tissues in the alveolar ducts and bronchioles. Despite the administration of corticosteroids, imaging revealed persistent fibrosis, and she required long-term oxygen therapy. Although recent reports indicated that corticosteroids are effective for drug-induced interstitial lung disease related to COVID-19 mRNA vaccination, this case presented a somewhat different clinical manifestation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
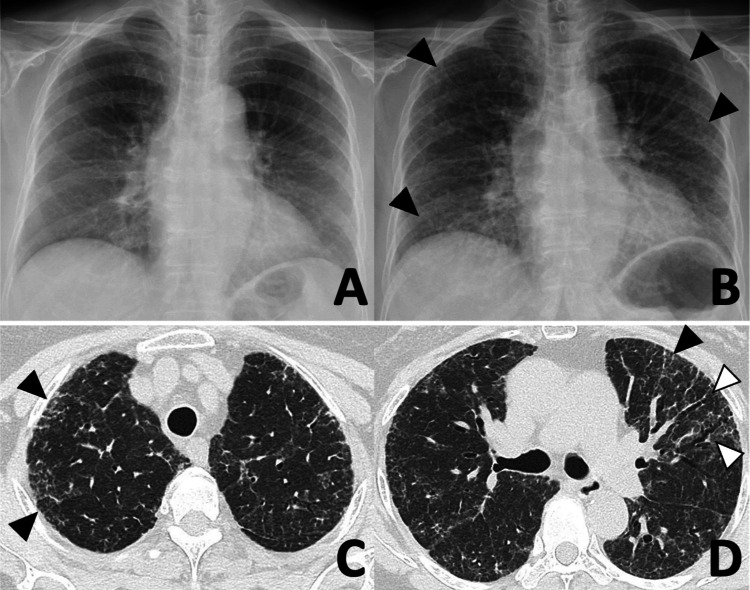 Figure 1
Figure 1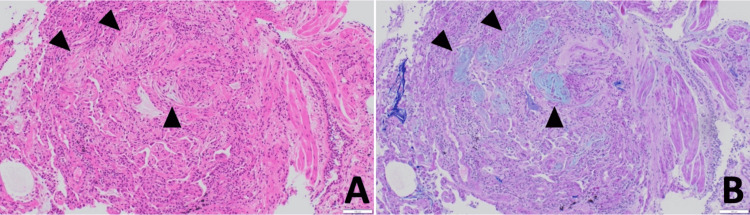 Figure 2
Figure 2| Range | Range | ||||
| Complete blood cell count | Immunoserological examination | ||||
| WBC, /μL | 6260 | 3300-8600 | C-reactive protein, mg/dL | 0.19 | <0.14 |
| Neutrophil count, % | 70.7 | - | antinuclear ab, times | ||
| Lymphocyte count, % | 14.7 | - | KL-6, IU/mL | 4191 | 105.3-401.2 |
| Monocyte count, % | 6.5 | - | SP-D, ng/mL | 1008 | <110 |
| Eosinophile count, % | 7.5 | - | Rheumatoid factor, IU/mL | 5 | 5.0-15.0 |
| Basophile count, % | 0.6 | - | Anti CCP ab | (-) | (-) |
| Haemoglobin, g/dL | 13.2 | 11.6-14.8 | Anti dsDNA ab | (-) | (-) |
| Platelet, /μL | 37.4×104 | 15.8-34.8 | Anti Sm ab | (-) | (-) |
| Biochemical examination | Anti SS-A ab | (-) | (-) | ||
| Total bilirubin, mg/dL | 0.6 | 0.4-1.5 | Anti SS-B ab | (-) | (-) |
| AST, IU/L | 28 | 13-30 | Anti U1-RNP ab | (-) | (-) |
| ALT, IU/L | 17 | 7-23 | Anti Scl-70 ab | (-) | (-) |
| LD, IU/L | 399 | 124-222 | Anti ARS ab | (-) | (-) |
| ALP, IU/L | 150 | 104-338 | Anti Jo-1 ab | (-) | (-) |
| Albumin, g/dL | 4.5 | 4.1-5.1 | Anti MDA5 ab | (-) | (-) |
| BUN, mg/dL | 10.3 | 8.0-20.0 | MPO-ANCA | (-) | (-) |
| Creatinine, mg/dL | 0.57 | 0.46-0.79 | PR3-ANCA | (-) | (-) |
| Sodium, mEq/L | 141 | 138-145 |
| (-) | (-) |
| Potassium, mEq/L | 4.2 | 3.6-4.8 | |||
| Chlorine, mEq/L | 107 | 101-108 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Respiratory viral infections research
Introduction
One of the COVID-19 mRNA vaccines, BNT162b2 (Pfizer-BioNTech), exhibits remarkable efficacy, boasting a 95% success rate in preventing disease exacerbation [1]. Common adverse effects associated with these vaccines include mild symptoms such as fever, fatigue, and headache [2]. However, severe adverse events such as anaphylaxis and thrombosis, though rare, have been reported [3,4]. Notably, drug-induced interstitial lung disease (DI-ILD) following vaccination is exceedingly uncommon. Despite this rarity, we encountered a case where dyspnea manifested immediately post-BNT162b2 vaccination, with subsequent imaging revealing interstitial lung disease. Histopathological examination confirmed DI-ILD. This case underscores the importance of vigilance within the medical community.
Case presentation
A septuagenarian woman was admitted to our hospital complaining of dyspnea on exertion. In December 2022, a chest radiograph taken as part of a medical check-up revealed no abnormalities in the lung fields. Ten days later, the patient received a fifth dose of BNT162b2. Subsequently, she began to experience dyspnea the following day, and her condition deteriorated throughout the month before her first hospital visit.
The patient had no history of exposure to dust inhalation, birds, mold, or humidifiers. Furthermore, she had no previous history of smoking or COVID-19 infection. She had been receiving fenofibrate therapy for several years. On admission, she required nasal cannula oxygenation at 4 L/min during physical exertion. Auscultation revealed fine crackles, audible predominantly in the lower thoracic region. No rashes or arthralgia were noted. Blood tests revealed an elevation of Krebs von den Lungen-6 (KL-6) and surfactant protein-D (SP-D) (Table 1). Antibodies associated with connective tissue disease and the Trichosporon asahii antibody were not detected. Urine Streptococcus pneumoniae antigen, urine Legionella pneumophila antigen, and sputum cultures were all negative. Two PCR samples (one from the nasopharynx and the other from saliva) were negative for acute respiratory syndrome coronavirus-2 (SARS-CoV-2). A chest radiograph taken after the fifth BNT162b2 revealed infiltrative shadows on the lower field of both lungs (Figures 1A, 1B). Chest computed tomography (CT) revealed bilateral ground-glass opacities (GGOs), with thickened interlobular septal walls and traction bronchiectasis (Figures 1C, 1D).
Chest radiograph and high-resolution CT of the chestBefore the fifth BNT162b2 mRNA vaccination, a chest radiograph showed no abnormalities (A). After vaccination, infiltrative shadows (black arrows) were detected in the lower field of both lungs (B). Chest computed tomography revealed bilateral ground-glass opacities (black arrows), thickened interlobular septal walls, and traction bronchiectasis (white arrows) (C, D).
Bronchoscopy was performed, and bronchoalveolar lavage (BAL) fluid from the right B5 showed lymphocyte and eosinophil proliferation (55% and 10%, respectively) and an increased CD4/CD8 ratio (6.6); bacterial cultures were negative. The transbronchial lung biopsy (TBLB) of the right B8a revealed strong fibrous growth from the alveolar wall into the alveoli, along with reactive type II alveolar epithelial growth and bronchial epithelialization. These findings were consistent with organizing pneumonia with fibrosis (Figure 2).
Histopathological findings obtained by transbronchial lung biopsyStrong fibrous growth from the alveolar wall into the alveoli (black arrows), reactive type 2 alveolar epithelial growth, and bronchial epithelialization were observed. (A) Hematoxylin-Eosin stain: ×100. (B) Periodic Acid-Schiff-Alcian Blue staining: ×100.
Based on the patient's clinical history, radiological features, laboratory data, and histopathological findings, a diagnosis of DI-ILD caused by the BNT162b2 mRNA vaccination was made. After bronchoscopy, the patient received 500 mg of methylprednisolone for three days, followed by prednisolone (PSL) at 30 mg/day. Following treatment initiation, the patient's symptoms subsided, and levels of both KL-6 and SP-D decreased. The patient was discharged from the hospital on Day 23; however, a follow-up CT scan seven weeks after her first visit showed persistent bilateral GGOs with fibrosis and traction bronchiectasis; therefore, long-term oxygen therapy was continued.
Discussion
Here, we diagnosed COVID-19 mRNA vaccine-related DI-ILD in a patient, showing no other cause of the sudden-onset ILD other than a recent COVID-19 mRNA vaccination.
BNT162b2 mRNA is encapsulated within lipid nanoparticles. When the mRNA reaches the target cell, it is taken up, and the encoded SARS-CoV-2 spike protein is expressed. The spike protein is then presented on the cell surface, where it is detected by dendritic cells, which in turn trigger cellular and humoral immune responses [5]. However, it is suggested that fragments of antigens and/or associated peptides may be released into the circulation and that the lipid nanoparticles may have proinflammatory effects [6]. Such immune responses may be associated with DI-ILD. According to a survey by the Japanese Ministry of Health, Labour, and Welfare (as of March 12, 2023), an estimated 294,416,519 doses of BNT162b2 have been administered. The total number of cases of interstitial pneumonia was 81 (0.000028%); therefore, sequelae are extremely rare. However, we do not know how many of these cases were DI-ILD.
We searched for recent reports of COVID-19 mRNA vaccine-related DI-ILD [7-14]. The characteristics of these patients include the appearance of respiratory symptoms soon after vaccination, onset of disease during the first or second vaccination period, high levels of KL-6 and SP-D (range 214-4084 U/mL and 73.1-675.5 ng/mL, respectively), an organizing pneumonia pattern on chest CT, a high percentage of lymphocytes in BAL fluid, and high responsiveness to steroids. In the current case, interstitial pneumonia appeared only after the fifth vaccination, and the response to steroids was poor. The latter was likely because the patient visited our outpatient clinic one month after the onset of the disease. In addition, lung fibrosis likely progressed during this time, causing irreversible changes to the lung structures.
Among the known case reports, TBLB was performed in two cases [12,14]. In all of these cases, polypoidal organization and fibrosis were observed in the alveolar space, and the fibrosis was relatively uniform at early time points. The pathological picture was different from that of cryptogenic organizing pneumonia due to strong inflammatory cell infiltration coupled with atypical alveolar epithelial cells. DI-ILD caused by the BNT162b2 mRNA vaccine is suspected to be a manifestation of organizing pneumonia with severe inflammation.
Conclusions
COVID-19 mRNA vaccine-related DI-ILD is extremely rare, and there is insufficient information to prove a causal relationship. It is important to note that the benefits of the COVID-19 vaccination outweigh the risks, as the vaccines are highly effective at preventing severe disease and hospitalization. We highly recommend that individuals get vaccinated; however, it should be noted that DI-ILD can occur after COVID-19 mRNA vaccination, as in this case. Further studies on COVID-19 mRNA vaccine-related DI-ILD are required.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Safety and Efficacy of the BNT 162b 2 m RNA Covid-19 Vaccine N Engl J Med Polack FP Thomas SJ Kitchin N 2603261538320203330124610.1056/NEJ Moa 2034577 PMC 7745181 · doi ↗ · pubmed ↗
- 2Adverse reactions to the first and second doses of Pfizer-Bio N Tech COVID-19 vaccine among healthcare workers J Infect Chemother Maruyama A Sawa T Teramukai S Katoh N 9349422820223536153610.1016/j.jiac.2022.03.015PMC 8947941 · doi ↗ · pubmed ↗
- 3COVID-19 vaccine-associated anaphylaxis: A statement of the World Allergy Organization Anaphylaxis Committee World Allergy Organ J Turner PJ Ansotegui IJ Campbell DE 1005171420213355882510.1016/j.waojou.2021.100517 PMC 7857113 · doi ↗ · pubmed ↗
- 4Adverse events following COVID-19 m RNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia Immun Inflamm Dis Yasmin F Najeeb H Naeem U 011202310.1002/iid 3.807PMC 1002242136988252 · doi ↗ · pubmed ↗
- 5BNT 162b 2 m RNA COVID-19 Vaccine: First Approval Drugs Lamb YN 4955018120213368363710.1007/s 40265-021-01480-7PMC 7938284 · doi ↗ · pubmed ↗
- 6Adverse effects of COVID-19 m RNA vaccines: the spike hypothesis Trends Mol Med Trougakos IP Terpos E Alexopoulos H 5425542820223553798710.1016/j.molmed.2022.04.007PMC 9021367 · doi ↗ · pubmed ↗
- 7COVID-19 vaccine-related interstitial lung disease: a case study Thorax Park JY Kim JH Lee IJ 1021047720223436283810.1136/thoraxjnl-2021-217609 · doi ↗ · pubmed ↗
- 8COVID-19 vaccine induced interstitial lung disease J Infect Chemother Yoshifuji A Ishioka K Masuzawa Y 95982820223458001010.1016/j.jiac.2021.09.010PMC 8450284 · doi ↗ · pubmed ↗