Bilateral Metastatic Gynecomastia from Small-Cell Lung Tumors in a Man: A Report of a Rare Case
Karima El Houari, Sophie Vandewalle

TL;DR
A man with a history of smoking developed painful gynecomastia, which was found to be metastases from a rare type of lung cancer.
Contribution
This report adds to the limited literature on breast metastases from small-cell lung cancer in men.
Findings
Bilateral gynecomastia was diagnosed as metastases from a small-cell lung tumor.
The case emphasizes the rarity of breast metastases from this cancer type in men.
Abstract
A case of a man with the recent onset of painful bilateral firm gynecomastia is reported. Mammography confirmed increased breast density. Biopsy characterized both masses as metastases of a small-cell lung tumor. This case highlights the atypical presentation and complements the literature regarding the rarity of breast metastases from small-cell lung cancer in men. Teaching point: Bilateral gynecomastia in a man with a long history of cigarette smoking should be considered with caution.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
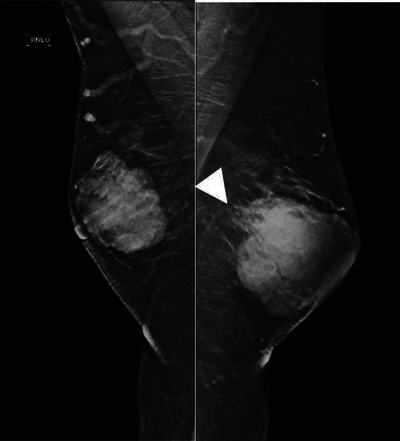 Figure 1
Figure 1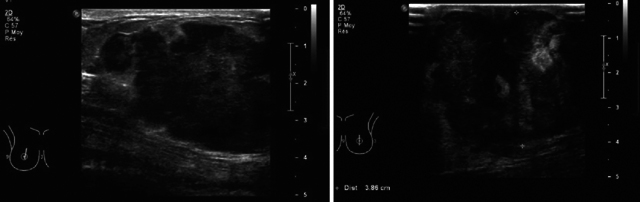 Figure 2
Figure 2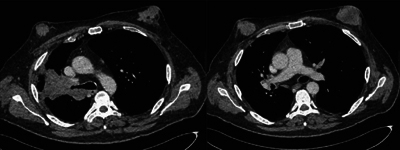 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMale Breast Health Studies · Cancer Diagnosis and Treatment
Introduction
Breast metastases from small-cell lung cancer (SLCS) are exceptional in men (0.2%–1.3%) [1, 2]. Differentiating between a primary small-cell breast tumor and breast metastases of a small-cell lung tumor is a diagnostic challenge given their common morphological characteristics [1, 3]. This rare case complements the existing scarce literature and highlights the atypical presentation of small-cell lung tumors in males [4].
Case Report
We report the case of a 53-year-old man referred for the exploration of bilateral, painful, and firm breast development, which appeared within 1 month. The patient was known for alcohol abuse and was a long-time smoker. There was no personal or family history of breast cancer. A clinical examination confirmed bilateral gynecomastia with induration.
A mammogram revealed the presence of a macro-lobulated retro-nipple opacity bilaterally (Figure 1), measuring 52 × 38 × 50 mm on the right and 50 × 50 × 40 mm on the left, and with blurred posterior contour (white arrow). Both masses were classified as BIRADS 4 (Figure 1).
Mammogram with external oblique view of the right breast and the left breast demonstrating an increase in breast density with a macrolobulated shape bilaterally, with blurred posterior contours (white arrowhead) and retronipple topography. No contact with the pectoral muscle.
Ultrasound confirmed the presence of an irregular marginated lobulated hypoechogenic and vascularized masses in both breasts (right Figure 2a; left Figure 2b). Bilateral axillary lymphadenopathy with cortical thickening was also present.
(a) Ultrasound right breast longitudinally. (b) Ultrasound the left breast. Ultrasound confirmed the presence of an irregular marginated lobulated hypoechogenic and vascularized masses in both breasts.
Microbiopsies of the breast masses and cytopuncture of axillary lymphadenopathy revealed breast metastases of a small-cell tumor.
The thoraco-abdominal computed tomography (CT) scan confirmed the presence of a large right upper lobar budding tumor, histologically a small-cell bronchial carcinoma (Figure 3).
Thoraco-abdominal CT scan injected into the parenchymal window: left upper lobar mass stenosing the right lobar bronchus and “mass” type breast tissue development, bilaterally.
The treatment proposed was chemotherapy and immunotherapy.
Discussion
SLCS is an aggressive neuroendocrine tumor that exceptionally metastasizes to the breast (0.2%–1.3%) [1, 5]. Pulmonary SLCS is often diagnosed incidentally, given its insidious nature [2, 6]. There are only two cases of bilateral breast metastases from pulmonary SLCS in male patients reported in the literature in 1976 and 2011 [7, 3].
Malignancy must be considered in cases of recent-onset gynecomastia associated with smoking [8]. In addition, it is imperative to distinguish between a primary breast and metastasized pulmonary SLCS because the therapeutic approach and the prognosis are different [3, 9, 10].
Although breast metastatic lesions are more superficial and do not cause skin retraction, a distinction between both entities is impossible [1, 11]. A biopsy is required and the final diagnosis is based on the histological and immunohistochemical analysis, including TTF1 marker, neuroendocrine (NSE, chromogranin A, and synaptophysin), and hormonal receptors [3, 10]. The TTF-1 marker not being specific on its own. [1].
Conclusion
Breast metastases from SLCS are exceptional, especially in male. The distinction between pulmonary and breast small-cell tumors is a diagnostic challenge in imaging. Biopsy and extensive immunohistochemical analyzes are essential for differentiation and therapeutic management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Khoury R, Bucau M, Bizot A, Khalil A. Breast metastasis of a lung carcinoma. BJR case Rep. 2022;8(2):20210142. DOI: 10.1259/bjrcr.20210142.36177253 PMC 9499442 · doi ↗ · pubmed ↗
- 2Bannon M, Marak C, Ashraf A, et al. Unusual presentation of a small cell lung cancer with bilateral breast metastases: Case report and a brief review of the literature. Respir Med Case Rep. 2022;38:101693. DOI: 10.1016/j.rmcr.2022.101693.35799863 PMC 9254160 · doi ↗ · pubmed ↗
- 3Altintoprak F, Baytekin HF, Tasdemir C. Primary small cell carcinoma of the lung presenting with breast and skin metastases. Korean J Intern Med. 2011;26(2):207–209. DOI: 10.3904/kjim.2011.26.2.207.21716912 PMC 3110854 · doi ↗ · pubmed ↗
- 4Mirrielees JA, Kapur JH, Szalkucki LM, et al. Metastasis of primary lung carcinoma to the breast: A systematic review of the literature. J Surg Res. 2014;188(2):419–431. DOI: 10.1016/j.jss.2014.01.024.24560348 · doi ↗ · pubmed ↗
- 5Güldoğan N, İçten GE, Tokat F, et al. Three cases of breast metastases from lung cancer and systematic review of the literature. Eur J Breast Health. 2021;17(2):200–205. DOI: 10.4274/ejbh.galenos.2020.5703.33870122 PMC 8025728 · doi ↗ · pubmed ↗
- 6Economopoulou P, Chrysikopoulou A, Goula K, et al. Breast Metastasis from neuroendocrine carcinoma of the lung: A case report and review of the literature. Case Rep Oncol. 2020;13(3):1281–1284. DOI: 10.1159/000510936.34191931 PMC 7649700 · doi ↗ · pubmed ↗
- 7Giarelli L, Ferlito A. Bilateral Breast metastases from oat‐cell lung carcinoma in a man treated with diethylstilbestrol for prostatic adenocarcinoma. J Am Geriatr Soc. 1976;24(11):511–515. DOI: 10.1111/j.1532-5415.1976.tb 03274.x.184140 · doi ↗ · pubmed ↗
- 8Collins LG, Haines C, Perkel R, Enck RE. Lung cancer: Diagnosis and management. Am Fam Physician. 2007;75(1):56–63.17225705 · pubmed ↗