An Unusual Presentation of Erythema Multiforme Following the Administration of Pfizer-BioNTech COVID-19 mRNA Vaccine in a Pediatric Patient
Yara Alghamdi, Fahad Abdulghani, Hassan F Huwait, Magdy Abdulghani, Sahal J Samarkandy

TL;DR
A 14-year-old girl developed erythema multiforme after receiving the Pfizer-BioNTech COVID-19 vaccine, a rare but reported side effect.
Contribution
This case adds to the limited reports linking the BNT162b2 vaccine to erythema multiforme in pediatric patients.
Findings
Erythema multiforme was observed in a previously healthy 14-year-old girl after the first dose of the BNT162b2 vaccine.
This case is among 14 reported cases of new-onset erythema multiforme following the BNT162b2 vaccine.
Erythema multiforme is a rare but documented cutaneous reaction to the Pfizer-BioNTech vaccine.
Abstract
Coronavirus disease 2019 (COVID-19) caused a global calamity that forced emergency use authorization to Pfizer-BioNTech COVID-19 (BNT162b2) vaccine. It is efficacious in preventing symptomatic severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection in seronegative recipients. The safety profile is still unclear; however, commonly reported symptoms post-vaccination are fatigue, headache, muscle pain, chills, and injection-site pain. COVID-19 disease elicits, to some extent, cutaneous side effects like urticaria, morbilliform rash, and chilblain-like eruption. Vaccination against COVID-19 was reported to induce similar dermatologic manifestations, such as urticarial rash, delayed large-local reaction, local injection-site reaction, and morbilliform eruption. Erythema multiforme (EM) is a rare manifestation post-vaccination, and only a few reports implicate it as a culprit…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1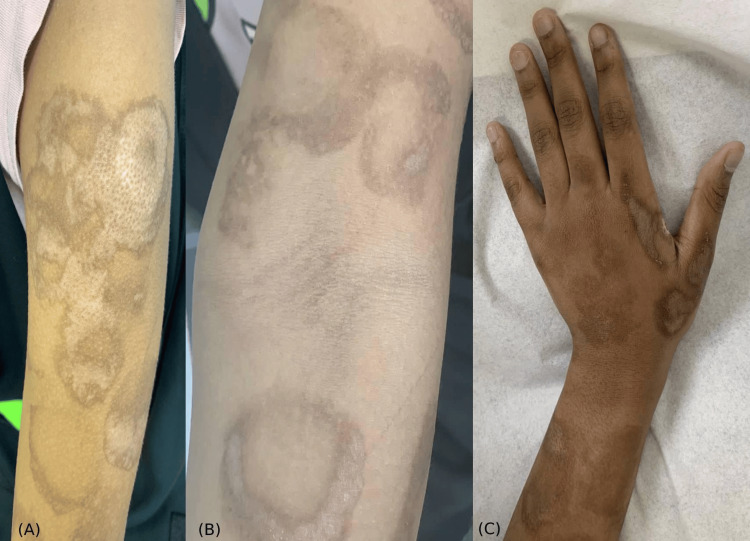 Figure 2
Figure 2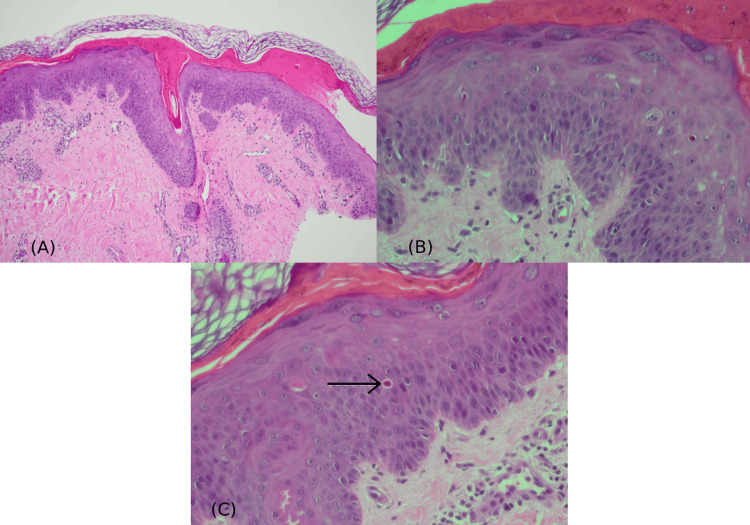 Figure 3
Figure 3| Sources | Age | Gender | Dose | Anatomical distribution | Mucosal involvement | Temporal eruption | Histopathology report | Previous HSV1 infection |
| New-onset EM2 after BNT162b23 Vaccine | ||||||||
| Borg et al. [ | 38 | Male | First dose | Arm, elbow, and sole | Yes | 2 days post-vaccination | Perivascular lymphocytic and histiocytic infiltrate in the upper dermis. Apoptotic keratinocytes throughout epidermis. | No |
| Kim et al. [ | 78 | Female | First dose | Generalized | Yes | 10 days after vaccination | Necrotic keratinocytes and subepidermal bullae with lymphocytic and eosinophilic infiltrate in DEJ4. | No |
| Sechi et al. [ | 76 | Female | First dose | Acral distribution | - | 4 days after vaccination | Vacuolar interface dermatitis with inflammatory lymphohistiocytic infiltrate in dermis. Mild epidermal spongiosis. | No |
| Bonino et al. [ | 91 | Female | Second dose | Neck, trunk, back, and extremities | No | 6 days after vaccination | Perivascular lymphocytic infiltrate in DEJ4. Dyskeratotic keratinocytes in the basal layer. Satellite lymphocytes. | No |
| Wunderlich and Dirschka [ | 61 | Female | Second dose | Acral distribution | Yes | 2 days after vaccination | Necrotic keratinocytes in epidermis obscuring DEJ4. Papillary edema. Perivascular inflammatory infiltrate, and eosinophilia. | No |
| de Las Vecillas et al. [ | 47 | Female | Second dose | Generalized | No | 1 day after vaccination | Interstitial perivascular dermatitis. Lymphohistiocytic and eosinophilic infiltrate. Intraepidermal and subcorneal spongiotic vesicles. | No |
| Scharf et al. [ | 27 | Female | First dose | Acral distribution (also observed on the patient's melanocytic nevi) | - | 3 days after vaccination | No histology was obtained. Diagnosis of Nevocentric EM2 was made on clinical grounds. | No |
| Charfi et al. [ | 51 | Female | First dose | Acral distribution | - | 5 days after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No |
| 55 | Male | Second dose (EM2 also appeared after first dose) | Upper and lower extremities | - | 6 days after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No | |
| Katayama and Ota [ | 60 | Female | Second dose | Elbows | No | 3 days after vaccination | Keratinocytes apoptosis, with basal vacuolar change, spongiosis with lymphocytes, and perivascular lymphohistiocytic infiltrate. | No |
| Petruzzi et al. [ | 55 | Female | First dose (EM2 also flared after second dose) | Oral, genital, knees, and acral involvement | Yes | 1 day after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No |
| 49 | Female | Second dose | Oral (tongue, gingiva, buccal mucosa, mouth floor, and soft palate) | Yes | 1 day after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No | |
| 20 | Female | First dose | Oral and genital involvement | Yes | 18 days after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No | |
| 15 | Male | First dose | Generalized | Yes | 7 days after vaccination | No histology was obtained. Diagnosis of EM2 was made on clinical grounds. | No | |
| EM flare-up after BNT162b2 Vaccine | ||||||||
| Livery et al. [ | 58 | Female | First dose (similar eruption has occurred 24 hours after second dose vaccination with BNT162b23) | Acral distribution (bilateral palms and soles) | No | 12 hours after vaccination | - | Yes (Herpes labialis) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDrug-Induced Adverse Reactions · Heparin-Induced Thrombocytopenia and Thrombosis · Intramuscular injections and effects
Introduction
Pfizer-BioNTech mRNA COVID-19 (BNT162b2) has undergone authorization to be administered to the public to prevent Coronavirus disease 2019 (COVID-19) [1]. It is administered to persons older than 12 years for the prevention of symptomatic severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) infection. It is an mRNA vaccine encoding SARS-CoV-2 spike-protein in lipid nanoparticles. Frequently reported side effects are miscellaneous and related to the immune system's reaction to vaccine components, like fatigue and muscular pain. The phenomenon of cutaneous eruption is of a peculiar manner. COVID-19 disease itself elicits dermatologic eruptions like urticaria, morbilliform rash, and chilblain-like reactions [1]. Nevertheless, vaccination against COVID-19 induces similar cutaneous manifestations, specifically, urticarial rash, delayed large-local reaction, local injection-site reaction, morbilliform eruption, erythromelalgia, and cosmetic-filler reaction [1]. Erythema multiforme (EM) is a rare dermatologic manifestation post-vaccination, and only 15 papers reported its eruption following the BNT162b2 vaccine [2-12]. Herein, a healthy adolescent female developed atypical EM after first-dose vaccination with BNT162b2.
Case presentation
A healthy 14-year-old female developed localized unilateral cutaneous eruption throughout the left upper extremity that manifested after the administration of the BNT162b2 vaccine. Approximately one-hour post-vaccination, a localized fluid-filled bullous formed at the injection site. The next day, the bullous confluent into pruritic dusky-red two-zoned incomplete-ring targetoid scaly plaques (Figures 1-2). There was no face, ocular, mucosal, or systemic manifestation. New medications, previous history of similar lesions, signs of herpes-simplex-virus (HSV) infection, and prodromal symptoms were all denied. Referral for dermatological assessment was done 20 days post-eruption, and demonstrated ill-defined two-zoned scales with dusky-red incomplete-ring plaques over the left extremity, favoring the extensor surface (Figures 1-2). Histopathology showed a regenerative epidermis with scattered dyskeratotic keratinocytes (Figure 3). From a clinical and histopathological aspect, atypical EM secondary to the BNT162b2 vaccine was established. Usual management was offered with betamethasone-valerate 0.1% cream and fusidic-acid 2% cream to counteract any secondary bacterial infection. At the follow-up examination, EM-eruption had improved. Presentation of acute localized EM within the first four hours post-vaccination will hinder the patient from receiving the second dose of BNT162b2 and other mRNA vaccines.
(A) Acute localized cutaneous eruption after the BNT162b2 vaccination over the left upper extremity. The eruption materialized firstly on the injection site, deltoid area, and disseminated downward through the arm and hand favoring the extensor surface. (B) Scale formation on the ill-defined incomplete ring-shaped dusky-tanned two-zoned targetoid plaque. (C) Two-zoned dusky purpuric center surrounded by a pale targetoid plaque over the extensor surface of the left arm.
(A) Poorly defined morphed targetoid plaques with signs of PIH over the left deltoid area. (B) Incomplete ring-formation of targetoid lichenoid plaques with signs of PIH, xerosis, and excoriation on the anterior aspect of the arm. (C) Targetoid plaques taking the shape of incomplete rings with signs of post-inflammatory hyperpigmentation on the dorsal aspect of the hand.PIH: post-inflammatory hyperpigmentation
(A) Hematoxylin and eosin (H&E)-stained section shows orthokeratotic hyperkeratosis, overlying a layer of necrotic epidermis (x100 magnification). (B and C) The underlying epidermis is regenerative with predominantly scattered supra-basal dyskeratotic keratinocytes (arrow) (H&E; x40 magnification, features suggestive of EM pattern).EM: erythema multiforme
Discussion
EM is a self-limited immune-mediated reaction with unknown pathogenesis. The most frequent trigger is HSV [13]. It has been linked to SARS-CoV-2 infection as typical acral eruption in young persons, and widespread atypical manifestation in adults [4]. EM is a rare dermatologic manifestation post-vaccination, and only 15 papers reported on its eruption following the BNT162b2 vaccine [2-12].
One hypothesis that explains the abrupt onset of EM is pre-sensitization. Post-vaccination adverse events are generally attributed to the immune system's reaction to the vaccine’s components like egg protein, gelatin, and polyethylene-glycol (PEG). Those ingredients are necessary to stabilize vaccines during transportation, prevent bacterial contamination, and improve the drug’s water solubility; the latter is achieved by PEG [14]. BNT162b2 vaccine does not contain any food or drug components; however, it is formulated with PEG to stabilize lipid nanoparticles containing active SARS-CoV-2 mRNA-protein [14]. PEG is found in numerous medications and injectable steroids. Although safe, reports have shown that 70% of patients receiving PEG therapies will develop anti-PEG IgG [14,15]. Thus, reaction to PEG-formulated products (i.e. vaccines) indicates previous sensitization.
Vaccine-induced EM is highly infrequent. Nonetheless, it has been implicated before in literature with diphtheria-pertussis-tetanus, measles-mumps-rubella, and human papillomavirus vaccines [2]. Su et al. [16] have collected data from 1999 to 2017 and concluded the median time of EM onset post-vaccination is six days; while adverse events occurred within two weeks. The temporal association of the BNT162b2 vaccine and EM eruption in this report is unusual compared with the data from Su et al. [16] as it appeared within 24 hours.
EM is secondary to the BNT162b2 vaccine, although rare, but scarce reports exist [2-12]. The body of evidence from the literature reported 14 new cases, and one report described a flare of pre-existing EM [2-12]. The manifestation was highly variable from aspects of age, gender, dose-inflicted eruption, local or systemic manifestation, and anatomical involvement (Table 1). All reports described eruption in adults [2-12], there was only one adolescent report of EM [12]. The only consistent factor that supported EM diagnosis is the clinical and histopathological correlation. Almost all eruptions have manifested within two weeks, mostly in females (80%), after first-dose administration (66.66%), and resolved with topical corticosteroid.
Conclusions
EM pathogenesis, theoretically, involves a stimulus triggering a delayed hypersensitivity reaction. This stimulus could be PEG, and previous sensitization could explain the rapid manifestation in this report. EM secondary to the BNT162b2 vaccine is unusual. Nonetheless, the clinical picture along with histopathological correlation is suggestive of EM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical and pathologic correlation of cutaneous COVID-19 vaccine reactions including V-REPP: a registry-based study J Am Acad Dermatol Mc Mahon DE Kovarik CL Damsky W 1131218620223451707910.1016/j.jaad.2021.09.002PMC 8431833 · doi ↗ · pubmed ↗
- 2Generalized erythema multiforme-like skin rash following the first dose of COVID-19 vaccine (Pfizer-Bio N Tech)J Eur Acad Dermatol Venereol Kim MJ Kim JW Kim MS Choi SY Na JI 036202210.1111/jdv.17757 PMC 865661934661942 · doi ↗ · pubmed ↗
- 3Abrupt onset of Sweet syndrome, pityriasis rubra pilaris, pityriasis lichenoides et varioliformis acuta and erythema multiforme: unravelling a possible common trigger, the COVID-19 vaccine Clin Exp Dermatol Sechi A Pierobon E Pezzolo E 4374404720223461731710.1111/ced.14970 PMC 8652785 · doi ↗ · pubmed ↗
- 4Atypical erythema multiforme related to BNT 162b 2 (Pfizer-Bio N Tech) COVID-19 vaccine Int J Dermatol Buján Bonino C Moreiras Arias N López-Pardo Rico M Pita da Veiga Seijo G Rosón López E Suárez Peñaranda JM Sánchez-Aguilar Rojas D 07602021 http://10.1111/ijd.15894.10.1111/ijd.15894 PMC 865298634473839 · doi ↗ · pubmed ↗
- 5Erythema multiforme following COVID-19 vaccination (BNT 162b 2) [Article in German]Hautarzt Wunderlich K Dirschka T 68707320223467643810.1007/s 00105-021-04911-4PMC 8530369 · doi ↗ · pubmed ↗
- 6Viral-like reaction or hypersensitivity? Erythema multiforme minor reaction and moderate eosinophilia after the Pfizer-Bio N Tech BNT 162b 2 (m RNA-based) SARS-Co V-2 vaccine J Investig Allergol Clin Immunol de Las Vecillas L López J Morchón E Rodriguez F Drake M Martino M 777832202110.18176/jiaci.075734588156 · doi ↗ · pubmed ↗
- 7Nevocentric erythema multiforme after SARS-COV-2 vaccine J Eur Acad Dermatol Venereol Scharf C Di Brizzi EV Pellerone S Liguori M Giorgio CM Argenziano G 0236202210.1111/jdv.17688 PMC 865751434547145 · doi ↗ · pubmed ↗
- 8Pfizer-Bio N Tech SARS-Co V-2 m RNA vaccine-associated erythema multiforme J Eur Acad Dermatol Venereol Borg L Mercieca L Mintoff D Micallef D Pisani D Betts A Scerri L 0436202210.1111/jdv.1768234547125 · doi ↗ · pubmed ↗