Modified Technique to Fabricate a Definitive Closed Bulb Hollow Obturator for Maxillectomy in a Patient Following COVID-Associated Mucormycosis: A Case Report
Alcina Fernandes, Grazina Fernandes, Kennedy Mascarenhas, Meena Aras, Vidya Chitre

TL;DR
A new method was developed to create a lighter and more stable obturator prosthesis for a patient who had maxillectomy due to mucormycosis.
Contribution
A novel flasking technique and modified impression method were introduced to improve prosthesis design.
Findings
The flasking technique reduced the prosthesis weight, enhancing stability and retention.
The modified impression technique effectively captured palatal deformities.
The prosthesis provided an effective oro-nasal seal for the patient.
Abstract
Immunocompromised people developed mucormycosis as a result of the COVID-19 outbreak. Antifungal medications, surgical excision of infected tissues, and therapy of underlying metabolic problems are available forms of treatment. Usually, surgery entails completely excising the affected area. The patient is at risk for nasal twang, nasal cavity leaks, and impaired masticatory function because of these anomalies. The obturator prosthesis may form an oro-nasal seal in such problems. Additionally, lowering the prosthesis weight contributes to improved stability and retention. This case report explains a novel flasking technique to lessen the prosthesis weight and a modified impression technique to capture the palatal deformity.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
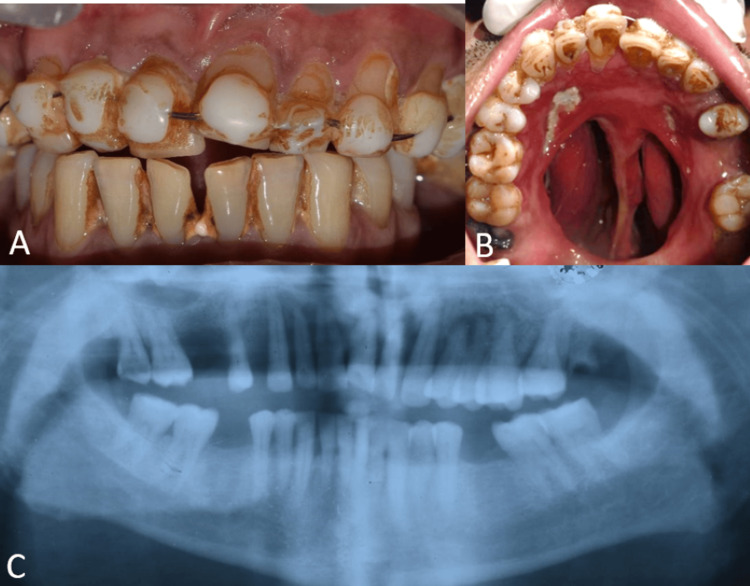 Figure 1
Figure 1 Figure 2
Figure 2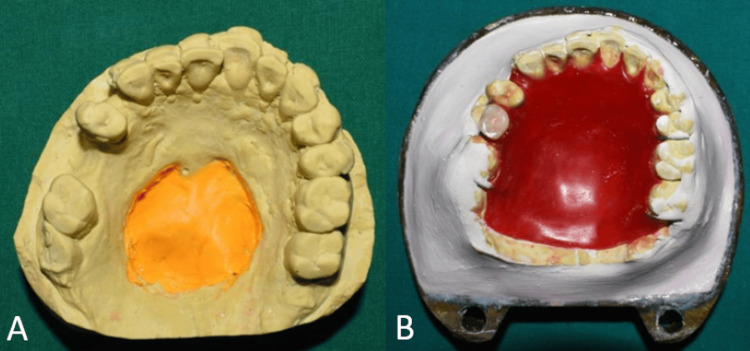 Figure 3
Figure 3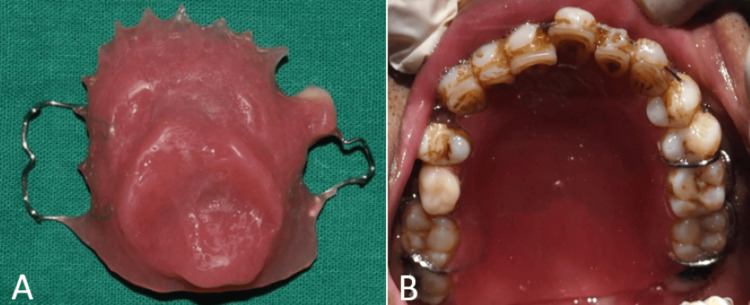 Figure 4
Figure 4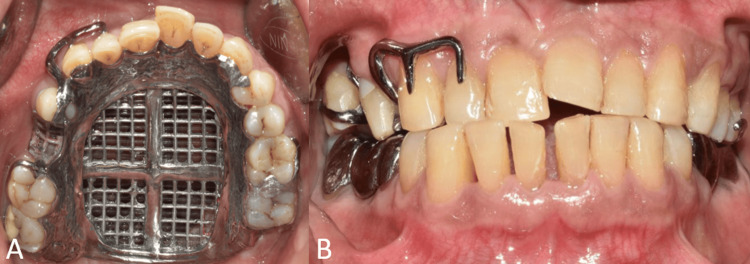 Figure 5
Figure 5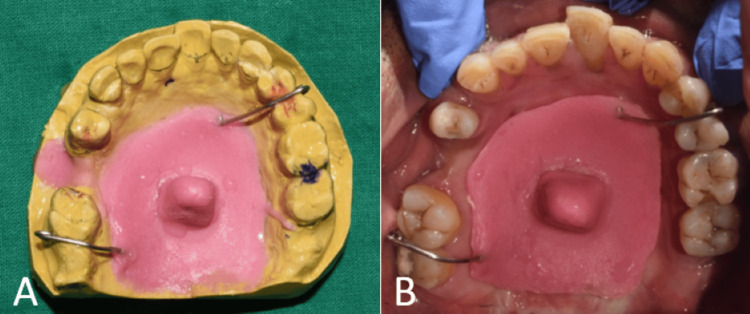 Figure 6
Figure 6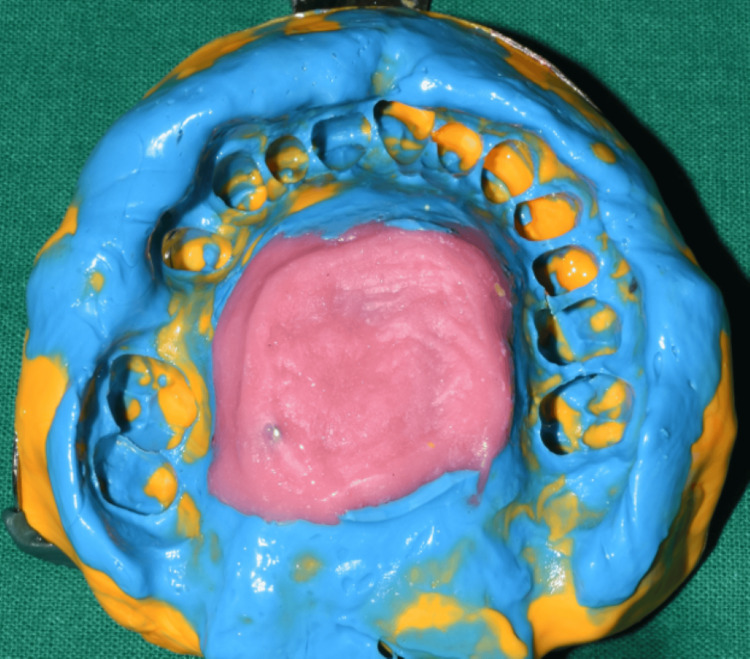 Figure 7
Figure 7 Figure 8
Figure 8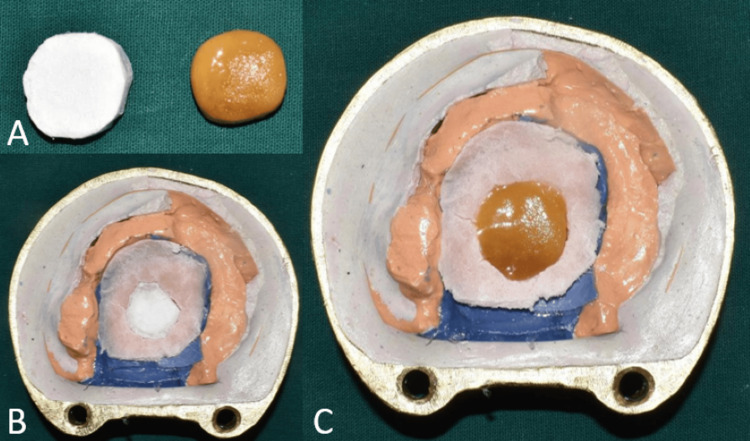 Figure 9
Figure 9 Figure 10
Figure 10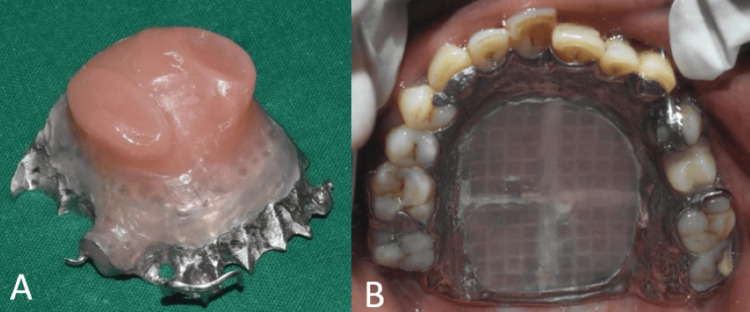 Figure 11
Figure 11Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEar Surgery and Otitis Media · Sinusitis and nasal conditions · Dental Research and COVID-19
Introduction
There was a spike in the number of cases of mucormycosis, or "Black Fungus," that were either directly or indirectly linked to COVID-19 during the second wave of coronavirus disease, or COVID-19, infection caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) virus in the year 2021 worldwide. The standard prosthetic treatment of defects plays a significant role in developing function for the patient [1,2].
Rehabilitating a maxillary defect frequently requires the use of a maxillary obturator. Keeping the nasal and oral cavities apart to allow for appropriate deglutition and articulation, supporting the orbital contents to prevent enophthalmos and diplopia, supporting the soft tissue to restore the midfacial contour, and attaining a satisfactory esthetic result are the goals of rehabilitation for patients who have had a total or partial maxillectomy [3,4].
The present article describes the prosthetic rehabilitation of a postsurgical defect due to mucormycosis.
Case presentation
A 47-year-old male patient was referred to the Department of Prosthodontics for prosthetic rehabilitation. The patient gave a history of uncontrolled diabetes with COVID-19 infection which resulted in chronic invasive fungal rhinosinusitis with mucormycosis. He underwent diagnostic nasal endoscopy (DNE) and hard palate sequestral excision under local anesthesia. As a result, the hard palate was removed, resulting in an Aramany Class III maxillary deformity (Figure 1). Upon clinical examination, the remaining teeth and the anterior hard palate were found to be movable. A lightweight hollow closed bulb maxillary obturator was therefore suggested as part of the patient's treatment plan to help with speech, deglutition, and mastication.
Intraoral and OPG view showing the maxillary defect(A) Frontal view on maximum intercuspation; (B) occlusal view of the maxillary arch showing the defect in the palate; (C) OPG showing the maxillary defect.OPG: Orthopantomogram
Procedure
Primary impression was made with irreversible hydrocolloid (Vignette chromatic, Dentsply India Pvt Ltd, Bengaluru, India) by blocking the palatal defect with gauze (Figure 2).
Primary impression and cast(A) Occlusal view of the maxillary arch showing the defect in the palate blocked with gauze; (B) primary impression of the maxillary arch; (C) primary cast of the maxillary arch
Impressions were poured and undercuts were blocked with putty silicone impression material (Zhermack Elite HD+, Zhermack SpA, Badia Polesine, Italy) (Figure 3). The interim obturator was fabricated incorporating a long-span Adams clasp on teeth no. 26 and 27 with an interproximal loop [5] for extra retention due to mobile teeth (Figure 4A). Conventional methods were used for dewaxing and investing. The interim obturator was delivered after finishing and polishing (Figure 4B).
Lab procedures(A) Primary cast showing blocked undercuts; (B) investing for fabrication of interim obturator.
Interim obturator (A) Intaglio surface of the interim obturator; (B) occlusal view of the maxillary arch showing the interim obturator.
For six months, the patient had weekly follow-ups. Once the patient's hard palate and teeth were less mobile, a definitive hollow bulb obturator was scheduled. The diagnostic cast was surveyed and the cast metal framework was designed with the following components: embrasure clasps on teeth no. 26 and 27; occlusal rest on teeth no. 15 and 17, cingulum rest on 13 and 23, modified complete palatal type of major connector extended till palatal surfaces of teeth. Distal surfaces of teeth no. 14, 17, and 27 were also prepared to act as a guiding plane.
Mouth preparation was done, and the mesio-occlusal rest seats were prepared on teeth no. 17, 24, and 27. The disto-occlusal rest seats were prepared on teeth no. 15 and 26. The canine rest seats were prepared on 13 and 23. Impression with polyvinyl siloxane (Elite HD+, Zhermack SpA, Badia Polesine, Italy) poured and cast metal framework was fabricated by conventional procedure. Cast metal framework in situ (Figure 5).
Intraoral view showing metal framework trial(A) Occlusal view showing metal framework trial; (B) frontal view showing metal framework trial.
A modified impression technique was used to capture the palatal defect, custom impression trays were fabricated using autopolymerizing acrylic resin (DPI-RR Cold CureTM, Dental Product of India, India) and adjusted to accommodate the palatal deformity by incorporating clasps for increased stability as shown in Figure 6.
Modified impression technique(A) Primary cast showing custom acrylic tray for making the final impression; (B) intraoral view showing the custom acrylic tray.
To make the impression, a stock tray covered in putty silicone impression material (Elite HD+, Zhermack SpA, Badia Polesine, Italy) was placed over a custom acrylic tray. Wash impression was made using light body polyvinylsiloxane (Elite HD+, Zhermack SpA, Badia Polesine, Italy). The final impression was adapted on the diagnostic cast and the cast was poured by using an altered cast technique (Figures 7, 8).
Final impression using the modified impression technique
Altered cast
Investing and dewaxing was done. For fabrication of hollow closed bulb obturator thermocol (polystyrene sheet) was used as a spacer as it is inert and conforms to the shape of the defect without much deformation. Trial closure was done with thermocol filled in the defect area (Figure 9). Thermocol was replaced by jaggery (cane sugar) similar in shape and size as it is highly soluble, easy to retrieve, and moldable [6].
Fabrication of hollow obturator(A) Image showing thermocol and jaggery of similar sizes; (B) trial closure was done with thermocol placed in the defect; (C) thermocol was replaced by jaggery to fabricate the hollow obturator.
After acrylisation, a small hole of 2 mm diameter was made into the denture area for removal of jaggery. A syringe with warm water was used to flush out the jaggery from the defect area (Figure 10). Autopolymersing resin was used to pack the hole and the definitive prosthesis was finished and polished (Figure 11). The patient was given post-insertion instructions and educated regarding hygiene maintenance.
Procedure for removal of jaggery(A) A 2 mm hole made on the intaglio surface of the obturator; (B) a syringe used to flush out jaggery; (C) after removal of jaggery.
Final prosthesis(A) Intaglio surface of the obturator; (B) occlusal view showing the final prosthesis.
Discussion
Mucormycosis is one of the rare opportunistic fungal infections presenting in different clinical forms. In 40% of individuals with mucormycosis, diabetes was shown to be the most prevalent predisposing condition. When the entire maxillary arch is affected, the lesion has an erosive character [7]. To prevent any recurrence, such patients typically have a very comprehensive bilateral maxillectomy. Patients' acceptance of one more intrusive treatment and inadequate bone are cited as reasons for the difficulty of surgical rehabilitation. Prosthetic rehabilitation using immediate, interim, and definitive obturators begins right after surgery if the defect is not surgically repaired. It preserves the midfacial contour by lifting and supporting soft tissues, promoting proper deglutition and speech articulation [8].
The classification of defects may lead to different framework designs for obturators. To limit dislodging functional forces, the prosthesis design should incorporate a robust primary connector for cross-arch stabilization as well as stabilizing and retaining components [9,10].
Many methods have been detailed for creating open and closed bulb hollow obturators, which reduce weight in the prosthesis such as putty, salt, and soap. To prevent fluid collection, the open hollow bulb obturator has to be cleaned frequently or have vent holes placed. It mostly accumulates fluids, mucus, and food [11]. Conversely, closed bulb obturators do not accumulate fluid since they extend sufficiently into the defect [12].
In this case report a novel technique for creating a closed hollow bulb obturator prosthesis has been detailed, which uses thermocol to regulate the hollow bulb's thickness and a jaggery spacer as methods used prior require multiple processing steps and are difficult to retrieve. Jaggery is a non-centrifugal cane sugar that is completely soluble in water. The benefits of using this technique include simplicity in manufacturing as the thermocol and jaggery can be shaped as needed, shorter time spent in the lab, the economy of scale, rigidity, and simplicity in retrieval [6].
Conclusions
In terms of the patient's need for both esthetics and function, the single-piece fully hollow design used in this report proved to be an excellent rehabilitation technique and allowed us to maintain the prosthesis weight as low as feasible. A modified impression technique was used to record the palatal defect. The approach demonstrates how to create a patient-centered, cost-effective method using widely available materials.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1COVID-19 and mucormycosis of orofacial region: a scoping review Cureus Banerjee A Das M Verma P Chatterjee A Ramalingam K Srivastava KC 015202310.7759/cureus.37984 PMC 1020234437223184 · doi ↗ · pubmed ↗
- 2Maxillofacial Prosthetics: Multidisciplinary Practice Chalian VA Drane JB Standish SM 133148 Baltimore The Williams and Wilkins Co.1971 https://www.sciepub.com/reference/76289
- 3Sectional prosthesis for total maxillectomy patients: a clinical report J Prosthet Dent Wang RR 241244781997929763810.1016/s 0022-3913(97)70020-9 · doi ↗ · pubmed ↗
- 4Definitive obturator fabrication for partial maxillectomy patient Case Rep Dent Singh M Limbu IK Parajuli PK Singh RK 6513210202020203225745310.1155/2020/6513210 PMC 7115166 · doi ↗ · pubmed ↗
- 5Long span adam’s clasp with interproximal arrow head: david’s modification J MAR Dent Sci Oral Rehabil Athisayamd 442023 https://www.medicalandresearch.com/current_issue/1288
- 6A simple and innovative technique of fabrication of a definitive closed hollow bulb obturator Int J Curr Res Farooqui R Aras MA Chitre V 87118713112020 https://doi.org/10.24941/ijcr.37334.12.2019
- 7Obturator prostheses for hemimaxillectomy patients J Oral Rehabil Keyf F 8218292820011158082010.1046/j.1365-2842.2001.00754.x · doi ↗ · pubmed ↗
- 8Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the mycoses Study Group Education and Research Consortium Lancet Infect Dis Cornely OA Alastruey-Izquierdo A Arenz D 02119201910.1016/S 1473-3099(19)30312-3PMC 855957331699664 · doi ↗ · pubmed ↗