Pulmonary sclerosing pneumocytoma mimicking a low-grade primary malignancy: A case report
Tomohide Ando, Tomonari Oki, Shuhei Iizuka, Yoshiro Otsuki, Toru Nakamura

TL;DR
A rare benign lung tumor called pulmonary sclerosing pneumocytoma can mimic low-grade cancer due to its fast growth rate, making diagnosis challenging.
Contribution
This case report highlights the rare occurrence of a short volume doubling time in pulmonary sclerosing pneumocytoma, resembling low-grade malignancies.
Findings
PSPs can grow rapidly with a volume doubling time of 249 days, similar to low-grade malignancies.
Histopathological analysis confirmed the diagnosis of PSP despite the rapid growth pattern.
Diagnostic testing beyond growth rate is essential for accurate identification of PSPs.
Abstract
Pulmonary sclerosing pneumocytoma (PSP) is a rare benign tumor classified as a pulmonary adenoma. It presents as a solitary pulmonary nodule without any specific findings, often posing a diagnostic challenge. We herein present a case of a PSP with a short volume doubling time (VDT) comparable to low-grade pulmonary malignancies. A 27-year-old female presented to the emergency department with a fever that had persisted for the past two days. An incidental finding on chest screening computed tomography (CT) revealed a 9 mm pulmonary nodule with a round shape and smooth margin, suggestive of a benign etiology. Follow-up CT one year later revealed an enlarged nodule exhibiting a VDT of 249 days. A thoracoscopic lingulectomy was performed, and the histopathological examination revealed papillary and diffuse proliferation of epithelial-like cells. The epithelial cells were positive for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
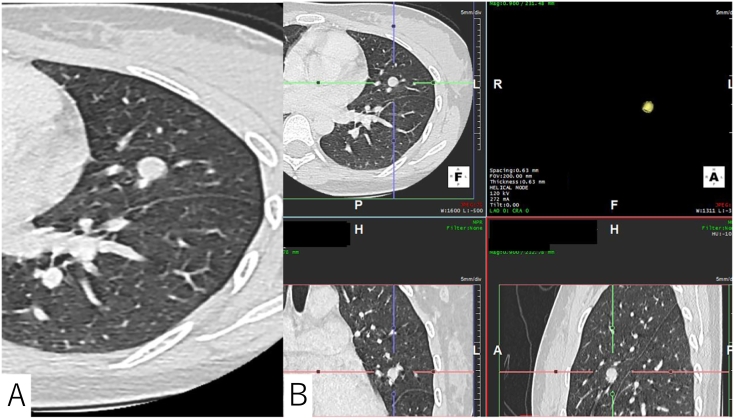 Figure 1
Figure 1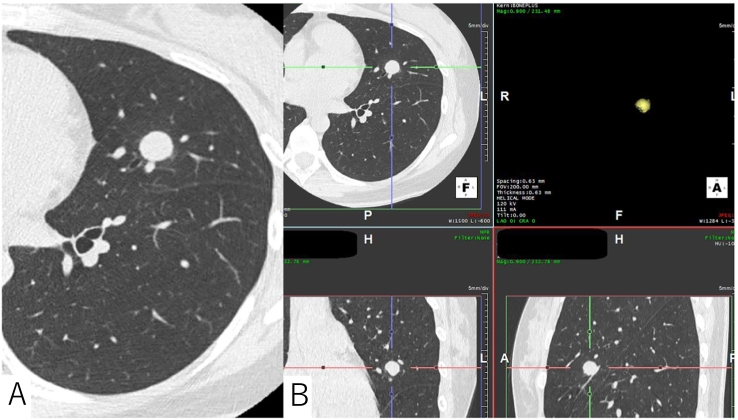 Figure 2
Figure 2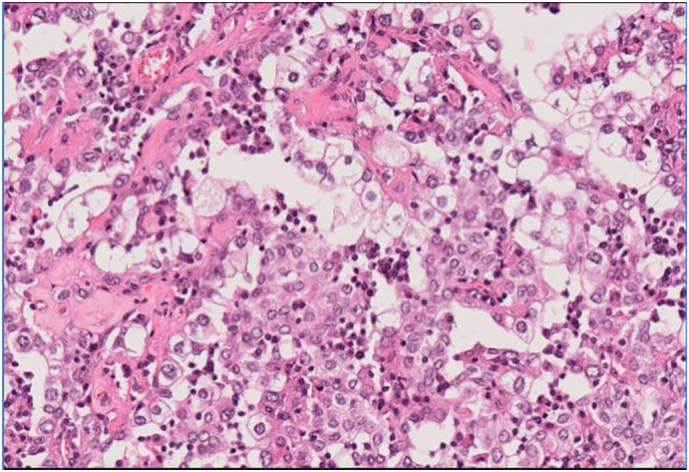 Figure 3
Figure 3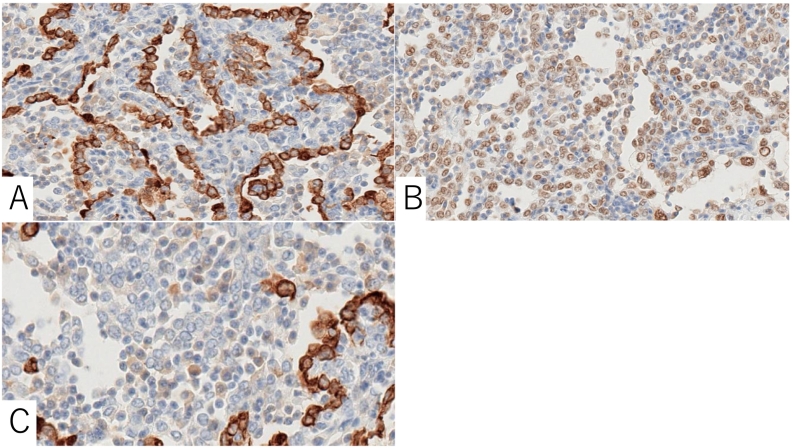 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedical Imaging and Pathology Studies · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · MXene and MAX Phase Materials
Introduction
1
Pulmonary sclerosing pneumocytoma (PSP) is a rare benign tumor of the lung previously known as sclerosing hemangioma and classified as a pulmonary adenoma [1,2]. It presents as a solitary pulmonary nodule without any specific findings, often posing a diagnostic challenge. While its radiological characteristics have been discussed in the literature, there have been limited reports addressing the volume doubling time (VDT) thus far. In this report, we present a case of a PSP with a VDT comparable to malignancies such as carcinoid tumors. This work has been reported in line with the SCARE criteria [3].
Case presentation
2
A 27-year-old woman, who had never smoked, presented with a fever persisting for the past two days. The patient had no relevant past medical history or family history. A physical examination revealed left costovertebral angle tenderness and a urinalysis revealed the presence of pyuria. There were no other indications suggestive of an obvious fever source. The diagnosis was pyelonephritis, and intravenous ceftriaxone was administered. An incidental finding on screening chest computed tomography (CT) revealed a 9 mm pulmonary nodule with a round shape and smooth margin in the left upper lobe (Fig. 1A). She reported no weight loss, hemoptysis, or shortness of breath. A three-dimensional CT scan obtained at a 0.63 mm thickness with volume rendering showed that the nodule volume was 425 mm^3^ (Fig. 1B). Volume rendering was obtained on Aquarius iNtuition 3D workstation (TeraRecon Inc., San Mateo, CA). Based on its radiological features, a benign pulmonary nodule was suspected and a radiographic follow-up was planned. One year later, the nodule enlarged to a maximum diameter of 14 mm (Fig. 2A) with an estimated volume of 1050 mm^3^ (Fig. 2B). No other pulmonary lesions or lymphadenopathies were observed. Due to the health insurance limitations, positron emission tomography was not accessible. A rapid growth pattern, with an estimated VDT of 249 days calculated using the Schwartz formula, prompted us to consider a malignancy [4]. Transbronchial biopsy was considered non-diagnostic because of the absence of a bronchial connection to the lesion, based on the thin-section CT. A surgical resection was planned for both diagnostic therapeutic purposes. The patient underwent a thoracoscopic lingulectomy successfully and was discharged uneventfully on the fifth postoperative day.Fig. 1A: A chest CT showing a 9 mm pulmonary nodule with a round shape and smooth margin in the left upper lobe.B: The volume of the nodule was estimated to be 425 mm3 based on the three-dimensional CT volume rendering reconstruction.Fig. 1. Fig. 2A: The nodule enlarged to a maximum size of 14 mm one year later.B: The nodule enlarged to a volume of 1050 mm^3^.Fig. 2
A histopathological examination revealed that the tumor was composed of a mixture of papillary, sclerotic, and solid patterns. The papillary area showed cores of fibrovascular sclerotic stroma and epithelioid cells lined by cuboidal epithelium. The solid area exhibited sheets of round to oval cells with pale eosinophilic cytoplasm (Fig. 3). Additionally, there was chronic infiltration of inflammatory cells, predominantly lymphocytes and plasma cells (Fig. 3). Immunohistochemical staining showed that the epithelial cells tested positive for cytokeratin (CKAE1/AE3) and thyroid transcription factor 1 (TTF1) (Fig. 4A and B), while the stromal cells were positive for TTF1 but negative for CKAE1/AE3 (Fig. 4C). No mitotic activity was not observed. Those results were consistent with a diagnosis of a PSP. She is currently disease free at 2 months since surgery.Fig. 3. Histopathological examination showing papillary and diffuse proliferation of epithelial-like cells, accompanied by increased numbers of round, relatively large cells in the tissue stroma.Fig. 3. Fig. 4A: The epithelial cells were positive for CKAE1/AE3.B: The epithelial cells were positive for TTF1.C: The stromal cells were positive only for TTF1.Fig. 4
Discussion
3
PSPs typically present as incidental pulmonary nodules with no specific findings, and are often misdiagnosed as malignancies. The diagnostic dilemma with PSPs arises from their rarity and the lack of specific radiological findings, with correct diagnostic rates reported at a maximum of 30.3 % even in large case series [5]. A hamartoma was considered as a potential differential diagnosis due to its well-defined appearance in the present case, but it was excluded based solely on its rapid growth, which indicated potential malignancy. The possibility of a metastatic tumor was also ruled out due to its isolated occurrence, which is an atypical presentation for a metastatic lesion.
To date, the radiographic features of PSPs have mainly been explored based on the morphological findings and metabolic activity, with limited research on their proliferative capacity [5,6]. The CT findings in the present case revealed a solitary, round-shaped nodule with a smooth margin that remained unchanged after a one-year follow-up, consistent with that of a PSP. Because positron emission tomography was not available, we focused on the VDT to speculate on its growth rate.
A rapid growth rate indicated by a VDT of 249 days raised suspicion of a malignancy. Except for the rapid enlargement, the radiological findings remained typical of a PSP. The epidemiological profile, especially among middle-aged Asian women, further substantiated the diagnosis [[7], [8], [9]].
The volume doubling time refers to the time required for a tumor to double in volume and is used to differentiate it between benign and malignancy [10]. While a long median doubling time of 965 days indicates a slow-growing nature and indolent behavior of a PSP, a short VDT of 374 days may also represent its biological diversity in the literature [[11], [12], [13], [14]]. The shortest VDT of 249 days in the present case seemed comparable to that of a low-grade malignancy such as a carcinoid tumor [[15], [16], [17]]. As a result, we misdiagnosed this case as a malignancy based solely on the short VDT. A histopathological examination in the present case revealed a typical finding compatible with a PSP, showing no mitotic activity. The pathogenesis of such a rapid growth remains unclear. Some PSPs may manifest with malignant characteristics, including metastases and even a potential fatality, despite their benign nature, demonstrating a broad spectrum of their biological features [18,19]. The report suggesting that regional lymph node metastases do not impact prognosis contributes not only to diagnostic but also to therapeutic challenges [20]. Besides its rarity and the lack of specific radiological findings, this biological diversity may lead to diagnostic confusion of a PSP.
Conclusion
4
PSPs may exhibit rapid growth, demonstrating a short VDT similar to that of low-grade pulmonary malignancies. The present case illustrated the diagnostic challenge of PSPs based solely on the growth rate and also underscored the importance of a comprehensive diagnostic workup for this rare entity.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical Approval was not required because the manuscript was not a research study and we only have the patient consent for writing and other forms of publication.
Funding
Not applicable.
Author contribution
AT wrote this paper. YO reviewed the pathological findings. All authors read and approved the final manuscript.
Guarantor
Toru Nakamura.
Research registration number
Not applicable.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Conflict of interest statement
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Travis W.D.Brambilla E.Nicholson A.G.Yatabe Y.Austin J.H.M.Beasley M.B.The 2015 World Health Organization classification of lung tumors: impact of genetic, clinical and radiologic advances since the 2004 classification J. Thorac. Oncol.102015124312602629100810.1097/JTO.0000000000000630 · doi ↗ · pubmed ↗
- 2Liebow A.A.Hubbell D.S.Sclerosing hemangioma (histiocytoma, xanthoma) of the lung Cancer 9195653751328470110.1002/1097-0142(195601/02)9:1<53::aid-cncr 2820090104>3.0.co;2-u · doi ↗ · pubmed ↗
- 3Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg.1092023113611403701395310.1097/JS 9.0000000000000373 PMC 10389401 · doi ↗ · pubmed ↗
- 4Schwartz M.A biomathematical approach to clinical tumor growth Cancer 141961127212941390970910.1002/1097-0142(196111/12)14:6<1272::aid-cncr 2820140618>3.0.co;2-h · doi ↗ · pubmed ↗
- 5Shin S.Y.Kim M.Y.Oh S.Y.Lee H.J.Hong S.A.Jang S.J.Kim S.S.Pulmonary sclerosing pneumocytoma of the lung: CT characteristics in a large series of a tertiary referral center Medicine (Baltimore)942015 e 49810.1097/MD.0000000000000498 PMC 460296925634202 · doi ↗ · pubmed ↗
- 6Xu J.Dong Y.Yin G.Jiang W.Yang Z.Xu W.Zhu L.(18) F-FDG PET/CT imaging: a supplementary understanding of pulmonary sclerosing pneumocytoma Thoracic Cancer 102019155215603113199210.1111/1759-7714.13100 PMC 6610286 · doi ↗ · pubmed ↗
- 7Kuo K.T.Hsu W.H.Wu Y.C.Huang M.H.Li W.Y.Sclerosing hemangioma of the lung: an analysis of 44 cases J. Chin. Med. Assoc.662003333812728972 · pubmed ↗
- 8Manickam R.Mechineni A.Pulmonary sclerosing pneumocytoma: an essential differential diagnosis for a lung nodule Cureus 142022 e 2108110.7759/cureus.21081 PMC 882694535165545 · doi ↗ · pubmed ↗