Guideline‐directed medical therapy assessment in heart failure patients undergoing percutaneous mitral valve repair
Karl‐Patrik Kresoja, Marianna Adamo, Karl‐Phillipp Rommel, Lukas Stolz, Nicole Karam, Cristina Giannini, Bruno Melica, Ralph Stephan von Bardeleben, Christian Butter, Patrick Horn, Fabien Praz, Daniel Kalbacher, Christos Iliadis, Holger Thiele, Jörg Hausleiter, Marco Metra

TL;DR
This study introduces a scoring system to assess how well heart failure patients are following recommended medical treatments before a specific heart valve repair procedure.
Contribution
A novel GDMT score is proposed and validated to evaluate medical therapy optimization in heart failure patients undergoing M-TEER.
Findings
The GDMT score is associated with lower all-cause mortality in heart failure patients.
Each point increase in the GDMT score reduces mortality risk by 10%.
The score considers three medication classes and is easy to use in clinical settings.
Abstract
Achieving optimized guideline‐directed medical therapy (GDMT) is recommended prior to transcatheter mitral valve edge‐to‐edge repair (M‐TEER) for secondary mitral regurgitation (SMR). We aimed to propose and validate an easy‐to‐use score for assessing the quality of GDMT in patients with heart failure with reduced ejection fraction (HFrEF) undergoing M‐TEER. Among the 1641 EuroSMR patients enrolled in the EuroSMR Registry who underwent M‐TEER, a total of 1072 patients [median age 74, interquartile range (IQR) 67–79 years, 29% female] had complete data on GDMT and a left ventricular ejection fraction ≤ 40% and were included in the current study. We proposed a GDMT score that considers the dosage levels of three medication classes (angiotensin‐converting enzyme inhibitors/angiotensin receptor blockers/angiotensin receptor‐neprilysin inhibitors, beta‐blockers, and mineralocorticoid…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
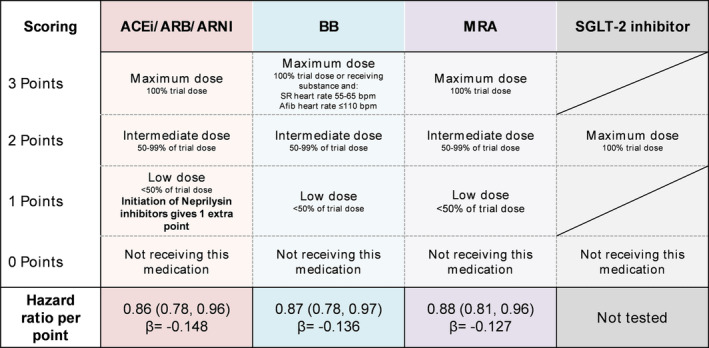 Figure 1
Figure 1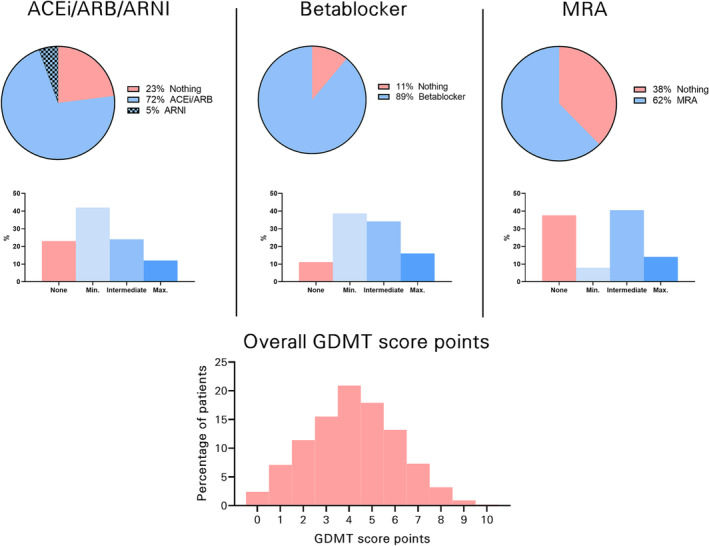 Figure 2
Figure 2| Overall cohort | GDMT score ≤ 4 | GDMT score > 4 |
| |
|---|---|---|---|---|
|
|
|
| ||
| Age, years | 74 (67–79) | 75 (69–80) | 73 (64–78) | <0.001 |
| Female sex, % | 307 (29) | 181 (30) | 126 (28) | 0.50 |
| NYHA class III/IV, % | 939 (87) | 536 (87) | 403 (87) | 0.67 |
| BMI, kg/m2 | 26 (23–30)/1067 | 26 (23–29)/611 | 27 (24–32)/456 | <0.001 |
| EuroSCORE II, % | 9.6 (5.0–23.0)/376 | 9.2 (5.0–22)/235 | 11 (5–24)/141 | 0.76 |
| Estimated glomerular filtration rate, mL/min/1.73 m2 | 47 (33–64)/1001 | 45 (30–60)/565 | 49 (36–67)/436 | <0.001 |
| NT‐proBNP, pg/mL | 3344 (1658–7291)/660 | 3500 (1786–7420)/379 | 3100 (1547–6698)/281 | 0.11 |
| Mean arterial blood pressure, mmHg | 87 (77–97)/1003 | 87 (77–100)/606 | 85 (77–95)/397 | 0.004 |
| Ischaemic heart disease, % | 576 (57)/1009 | 349 (60)/586 | 227 (54)/423 | 0.071 |
| Diabetes, % | 363 (35)/1025 | 191 (32)/595 | 172 (40)/430 | 0.010 |
| Arterial hypertension, % | 702 (70)/1006 | 392 (67)/584 | 310 (74)/422 | 0.031 |
| Previous myocardial infarction, % | 355 (33)/1063 | 210 (35)/609 | 145 (32)/454 | 0.39 |
| Previous percutaneous coronary intervention, % | 391 (47)/839 | 250 (49)/515 | 141 (44)/324 | 0.18 |
| Previous coronary artery bypass grafting, % | 224 (22)/1017 | 124 (21)/592 | 100 (24)/425 | 0.36 |
| Previous stroke, % | 104 (10) | 60 (10) | 44 (10)/457 | 1.00 |
| Chronic obstructive pulmonary disease, % | 175 (16)/1067 | 109 (18)/612 | 66 (15)/455 | 0.16 |
| Atrial fibrillation, % | 630 (59)/1068 | 363 (60)/610 | 267 (58) | 0.71 |
| Mitral regurgitation severity | 0.068 | |||
| II | 64 (5) | 44 (7) | 20 (4) | |
| III | 1008 (95) | 570 (93) | 438 (96) | |
| Mitral valve effective regurgitant orifice area, cm2 | 0.29 (0.2–0.39)/812 | 0.30 (0.20–0.40)/456 | 0.27 (0.20–0.38)/356 | 0.077 |
| Mitral valve biplane vena contracta, mm | 6.9 (5.5–8.0)/647 | 7 (5.7–8.1)/356 | 6.5 (5.4–7.6)/291 | 0.001 |
| Concomitant severe TR, % | 190 (18)/1039 | 126 (21)/591 | 64 (14)/448 | 0.004 |
| Left ventricular end‐diastolic volume, mL | 193 (150–240)/984 | 148 (188–234)/549 | 203 (152–253)/435 | 0.004 |
| Left ventricular ejection fraction, % | 30 (24–35) | 30 (24–35) | 29 (23–34) | 0.030 |
| Tricuspid annulus plane systolic excursion, mm | 16 (14–19)/850 | 16 (13–19)/475 | 17 (14–19)/375 | 0.78 |
| Estimated systolic pulmonary artery pressure, mmHg | 48 (38–58)/900 | 47 (38–58)/520 | 48 (39–58)/380 | 0.48 |
- —University Medical Center Mainz of the Johannes Gutenberg University Mainz
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEntrepreneurship Studies and Influences
Background and aims
Secondary mitral regurgitation (SMR) is frequent among patients with heart failure with reduced ejection fraction (HFrEF) and is associated with a dismal prognosis.1, 2 In current guidelines, transcatheter mitral valve edge‐to‐edge repair (M‐TEER) has been recommended as a therapeutic option for eligible patients.3, 4, 5 These guidelines emphasize the importance of optimization of guideline‐directed medical therapy (GDMT) for HFrEF before referring patients to M‐TEER.5, 6 However, real‐word data often show the underuse of GDMT.1, 7 Recent evidence highlighted that optimal GDMT is only achieved when maximum trial doses of substances are prescribed, which is often not the case in clinical practice. Thus, both initiation and titration to target doses administered in randomized controlled clinical trials are related to a better outcome for patients with heart failure.7, 8, 9, 10 Yet, given the large number of substances that are recommended and available for GDMT, it is challenging to provide an objective measure of GDMT that allows for monitoring of therapy intensity and to allow for comparison in scientific studies.
So far, there is no uniform framework on how to grade the quality of GDMT for HFrEF patients. We therefore aimed to provide a simple scoring framework to assess the quality of GDMT in HFrEF patients in general, validate it in a cohort of HFrEF patients with SMR undergoing M‐TEER, and assess its association with all‐cause mortality.
Methods
Study population
This analysis included patients with SMR who underwent M‐TEER at 11 European centres from the EuroSMR Registry. The EuroSMR design has been published before.11, 12 The management of GDMT was left to local physicians. All patients gave their informed consent. The study complied with the Declaration of Helsinki and was performed with the approval of local ethical committees. Patients with a left ventricular ejection fraction (LVEF) > 40% and patients in whom GDMT information was incomplete at baseline were excluded.
Guideline‐directed medical therapy score
As shown in Figure 1, GDMT medications were stratified into four classes: (i) angiotensin‐converting enzyme inhibitors (ACE‐Is), angiotensin receptor blockers (ARBs), or angiotensin receptor‐neprilysin inhibitors (ARNIs); (ii) beta‐blockers (BBs); (iii) mineralocorticoid receptor antagonists (MRAs); and (iv) sodium‐glucose cotransporter‐2 (SGLT‐2) inhibitors. A scoring system was proposed where patients could receive 0–3 points for each category according to the dosage levels [0 for not receiving the substance, 1 for minimum dosage (<50% of recommended trial dose), 2 for intermediate dosage (50–99% of recommended trial dose), and 3 for maximum dosage (100% of recommended trial dose); 1 extra point was given for ARNI initiation, and there were exceptions for BBs and MRAs] (Figure 1). Of note, SGLT‐2 inhibitors were not tested in the present study due to a lack of availability in the study period.
Framework for a scoring system for guideline‐directed medical therapy (GDMT). Proposed scoring scheme for a score to quantitatively assess the quality and quantity of GDMT. Patients can receive points from each domain and can receive a maximum of up to 12 points in total, indicating maximum GDMT. Further, the association of the domains with all‐cause mortality is displayed. Of note, sodium‐glucose cotransporter‐2 (SGLT‐2) inhibitors were not validated for the proposed score. Trial doses were defined according to the guidelines of the European Society of Cardiology Guidelines for heart failure. 6 ACE‐I, angiotensin‐converting enzyme inhibitor; Afib, atrial fibrillation; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor‐neprilysin inhibitor; BB, beta‐blocker; MRA, mineralocorticoid receptor antagonist; SR, sinus rhythm.
Statistical analysis and matching
Data are provided as the median and corresponding interquartile range (IQR) or the mean with standard deviation. Continuous variables were compared with the Mann–Whitney U test or the Kruskal–Wallis test, where appropriate. Categorical variables were compared using Fisher's exact test.
Cox regression analyses were performed to test the prognostic relevance of the baseline GDMT score with regard to all‐cause mortality.
A two‐sided significance level of α 0.05 was defined as appropriate to indicate statistical significance. Statistical analyses were performed using the SPSS software (IBM Corp. released 2017, Version 25.0, Armonk, NY, USA).
Results
Of 1641 patients undergoing M‐TEER between 2008 and 2021, 482 were excluded due to an LVEF > 40% and 87 due to missing data on the quality or quantity of GDMT. This resulted in a final cohort of 1072 patients, which exhibited characteristics similar to previous M‐TEER cohorts, including increased perioperative risk, impaired renal function, and significant SMR and left ventricular dilatation (Table 1).
The GDMT score was calculated as illustrated in Figure 1, and the distribution and intensity of GDMT according to the scoring system are displayed in Figure 2. The median GDMT score was 4 (IQR 3–5) points, indicating low GDMT intensity before M‐TEER. Only 12 patients (1.1%) achieved a GDMT score of 9 points, which is required to reach trial GDMT dosages in all three domains.
Quality and quantity of guideline‐directed medical therapy (GDMT) in the EuroSMR cohort. The pie charts represent the fraction of patients receiving the medication at all, and the bar charts below show the corresponding intensity of medication with reference to the recommended study trial dose. ACE‐I, angiotensin‐converting enzyme inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin receptor‐neprilysin inhibitor; MRA, mineralocorticoid receptor antagonist.
During a median follow‐up of 604 (IQR 342–1105) days, the primary outcome of all‐cause mortality occurred in 412 patients (38.4%). All score categories were associated with the primary outcome (Figure 1; P < 0.05 for all). The standardized beta values between the three score categories were comparable, indicating a reasonable fit of the point scoring system (ACE‐I/ARB/ARNI, β = −0.15; BB, β = −0.14; and MRA, β = −0.13). The overall GDMT score was also associated with the primary outcome [hazard ratio (HR) 0.90, 95% confidence interval (CI) 0.86–0.95 for each increase in one GDMT score point]. The GDMT score remained associated with the primary outcome after adjustment for estimated glomerular filtration rate (HR_adj_ 0.92, 95% CI 0.87–0.96) and the EuroSCORE II (HR_adj_ 0.91, 95% CI 0.83–0.99).
Conclusions
This study introduces a simple scoring system to assess the quality of GDMT in HFrEF patients in general and was validated in an HFrEF population with SMR undergoing M‐TEER. The purpose of this scoring system is not to predict prognosis but rather to provide a framework to grade the quality of GDMT, to allow for easy monitoring of GDMT adherence, on the one hand, and for comparability in the setting of clinical trials, on the other hand.
While the rate of administration of the different GDMT classes was comparable with randomized trials,4 GDMT intensity was low in this patient population, with almost no patients receiving maximum GDMT. With recent evidence showing that GDMT dosing and up‐titration is a crucial prognostic factor for HFrEF patients,9 the need for a tool to assess GDMT becomes evident.8 Interestingly, the self‐perception of physicians is in dire contrast to clinical reality, where most cardiologists believe their patients to be on optimal GDMT.13 The reasons for non‐up‐titration are manifold, but one important aspect might be the lack of perception of non‐optimized GDMT; a scoring system that automatically provides feedback on non‐optimal GDMT adherence might help to further sharpen physicians' attention in the clinical setting and raise awareness about GDMT intensification.8
Among objective criteria, impaired renal function and hypotension are often cited as common reasons for suboptimal dosing of GDMT. In line with this, renal function was a significant predictor of outcomes in patients treated conservatively in the COAPT study but not in those undergoing M‐TEER,14 suggesting that at least parts of the adverse effects of renal impairment can be alleviated by M‐TEER. Even in the absence of maximum GDMT, M‐TEER might provide clinical benefits by improving haemodynamics, especially with regard to forward flow and systemic perfusion, allowing for further intensification of GDMT, which has been associated with lower mortality.11, 15 Importantly, for some patients, M‐TEER might allow subsequent GDMT up‐titration. A scoring system in this setting might also be important for future randomized trials to allow for objective comparison and changes in GDMT adherence consequently to interventions that affect haemodynamics like M‐TEER.
The study's strengths include its large sample size, multicentre design, and use of real‐world data. However, the study only included patients undergoing M‐TEER, which may limit generalizability to other patient populations. Additionally, the availability of certain medications, such as ARNIs and SGLT‐2 inhibitors, varied during the study period and could therefore not be validated in the GDMT score. Yet, given the ease and safety of SGLT‐2 inhibitor initiation, directly at the GDMT recommended dose and without relevant adverse effects on renal function and haemodynamics, we believe this to be a justifiable limitation of the study.16 Lastly, reasons for suboptimal up‐titration of GDMT were not available and could not reasonably be assessed given the retrospective nature of the study.
In conclusion, this study provides a way to score GDMT intensity in patients with HFrEF and SMR undergoing M‐TEER. This scoring framework might be used in future clinical trials by heart teams to assess the quality of GDMT in this patient population. Lastly, the study highlights the need for further research to improve the use of GDMT in these patients.
Conflict of interest
K.‐P.K. has been a consultant to Edwards Lifesciences. M.A. has been a consultant to Abbott Structural Heart and Medtronic. K.‐P.R. reports no conflict of interest. L.S. has received speaker honoraria from Edwards Lifesciences. N.K. has received consultant fees from Abbott Structural Heart, Edwards Lifesciences, and Medtronic. C.G. has received consultant honoraria from Medtronic. B.M. has received a consulting fee and honoraria for lectures from Abbott and from Edwards. R.S.v.B. is a consultant to Abbott, Edwards, Jenscare, Medtronic, NeoChord, Philips, and Siemens. C.B. reports no conflict of interest. P.H. has received travel support and an educational grant from Abbott Medical GmbH and Edwards Lifesciences and an unrestricted research grant from Edwards Lifesciences. F.P. has received travel expenses from Abbott Vascular, Polares Medical, and Edwards Lifesciences. D.K. has received personal fees from Abbott Medical, Edwards Lifesciences, and Pi‐Cardia Ltd. C.I. has received travel and consultant honoraria from Abbott and Edwards Lifesciences. H.T. reports no conflict of interest. J.H. has been a consultant to Edwards Lifesciences. M.M. has received the following personal fees of minimal amounts since January 2021: from Amgen, LivaNova, and Vifor pharma as a member of Executive or Data Monitoring Committees of sponsored clinical trials; and from AstraZeneca, Bayer, Boehringer Ingelheim, Edwards Lifesciences, and Roche Diagnostics for participation to advisory boards and/or speeches at sponsored meetings. P.L. has been a consultant to Abbott Structural Heart, Edwards Lifesciences, and Medtronic.
Funding
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chioncel O , Lainscak M , Seferovic PM , Anker SD , Crespo‐Leiro MG , Harjola V‐P , et al. Epidemiology and one‐year outcomes in patients with chronic heart failure and preserved, mid‐range and reduced ejection fraction: An analysis of the ESC Heart Failure Long‐Term Registry. Eur J Heart Fail 2017;19:1574‐1585. doi:10.1002/ejhf.813 28386917 · doi ↗ · pubmed ↗
- 2Pagnesi M , Adamo M , Sama IE , Anker SD , Cleland JG , Dickstein K , et al. Impact of mitral regurgitation in patients with worsening heart failure: Insights from BIOSTAT‐CHF. Eur J Heart Fail 2021;23:1750‐1758. doi:10.1002/ejhf.2276 34164895 PMC 9290728 · doi ↗ · pubmed ↗
- 3Adamo M , Fiorelli F , Melica B , D'Ortona R , Lupi L , Giannini C , et al. COAPT‐like profile predicts long‐term outcomes in patients with secondary mitral regurgitation undergoing Mitra Clip implantation. JACC Cardiovasc Interv 2021;14:15‐25. doi:10.1016/j.jcin.2020.09.050 33309313 · doi ↗ · pubmed ↗
- 4Stone GW , Abraham WT , Lindenfeld J , Kar S , Grayburn PA , Lim DS , et al. Five‐year follow‐up after transcatheter repair of secondary mitral regurgitation. N Engl J Med 2023;388:2037‐2048. doi:10.1056/NEJ Moa 2300213. Published online ahead of print 5 March 36876756 · doi ↗ · pubmed ↗
- 5Vahanian A , Beyersdorf F , Praz F , Milojevic M , Baldus S , Bauersachs J , et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J 2022;43:561‐632. doi:10.1093/eurheartj/ehab 395 34453165 · doi ↗ · pubmed ↗
- 6Mc Donagh TA , Metra M , Adamo M , Gardner RS , Baumbach A , Böhm M , et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2022;24:4‐131. doi:10.1002/ejhf.2333 35083827 · doi ↗ · pubmed ↗
- 7Greene SJ , Butler J , Albert NM , De Vore AD , Sharma PP , Duffy CI , et al. Medical therapy for heart failure with reduced ejection fraction: The CHAMP‐HF registry. J Am Coll Cardiol 2018;72:351‐366. doi:10.1016/j.jacc.2018.04.070 30025570 · doi ↗ · pubmed ↗
- 8Packer M , Metra M . Guideline‐directed medical therapy for heart failure does not exist: A non‐judgmental framework for describing the level of adherence to evidence‐based drug treatments for patients with a reduced ejection fraction. Eur J Heart Fail 2020;22:1759‐1767. doi:10.1002/ejhf.1857 32432391 PMC 7687274 · doi ↗ · pubmed ↗