The Clinical Impact of Change in the C-Reactive Protein/Albumin Ratio in Gastric Cancer Patients Who Receive Curative Treatment
Toru Aoyama, Yukio Maezawa, Itaru Hashimoto, Kentaro Hara, Keisuke Komori, Kazuki Otani, Keisuke Kazama, Sho Sawazaki, Masakatsu Numata, Shinnosuke Kawahara, Haruhiko Cho, Junya Morita, Kenki Segami, Mie Tanabe, Norio Yukawa, Aya Saito, Yasushi Rino, Takashi Ogata, Takashi Oshima

TL;DR
This study shows that changes in the C-reactive protein/albumin ratio can predict survival outcomes in gastric cancer patients after curative treatment.
Contribution
The study identifies change in CAR as a novel prognostic marker for gastric cancer patients post-surgery.
Findings
Patients with a high-change in CAR had significantly lower 3- and 5-year overall survival rates compared to those with low-change in CAR.
Change in CAR was a significant prognostic factor for both overall survival and recurrence-free survival in gastric cancer patients.
The study found no significant differences in clinicopathological parameters like age, sex, T factor, or N factor between the high- and low-change CAR groups.
Abstract
Recently, change in the C-reactive protein/albumin ratio (CAR) has become a promising prognostic marker in some malignancies. The aim of the present study was to evaluate the clinical impact of change in the CAR in gastric cancer patients who received curative resection. The present study included 458 patients who underwent curative treatment for gastric cancer between 2013 and 2017. The prognosis and clinicopathological parameters were compared between patients who showed a high-change in CAR and those who showed a low-change in CAR. The OS stratified by each clinical factor was compared using a log-rank test, and a significant difference was observed using a 0.05 change in CAR. When the patient background factors were compared between the high-change (change in CAR ≥ 0.05) and low-change (change in CAR < 0.05) groups, the median age, sex ratio, T factor, and N factor were similar.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
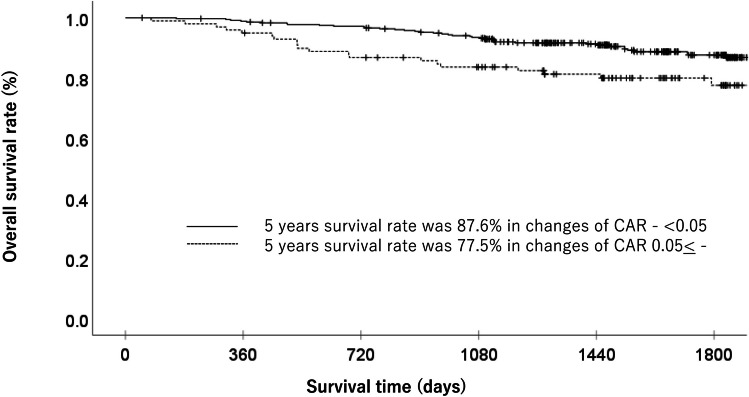 Figure 1
Figure 1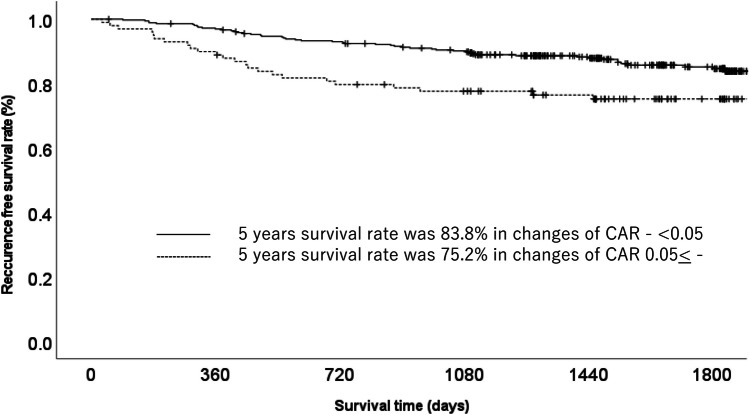 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Biomarkers in Disease Prognosis · Gastric Cancer Management and Outcomes · Cancer, Lipids, and Metabolism
Introduction
Gastric cancer is the fourth most common cancer and the second leading cause of cancer-related death in the world [1, 2]. The prognosis of gastric cancer is gradually improving with the improvement of minimally invasive surgery, perioperative care, and perioperative adjuvant treatment [3–5]. However, almost half of patients experience recurrence even after curative treatment [6, 7]. It is necessary to identify the prognostic factors and/or predictors of perioperative adjuvant treatment.
To date, several prognostic factors and predictors have been evaluated in gastric cancer. Recently, the nutrition status and systemic inflammation status have been shown to affect short- and long-term oncological outcomes [8]. Among them, the C-reactive protein/albumin ratio (CAR) is a promising prognostic factor. The CAR is identified as a non-specific marker of systemic inflammation. Some studies have shown that GC patients with a high CAR have a significantly poorer prognosis than those with a low CAR [9–11]. On the other hand, inflammation and nutritional status fluctuate dramatically. Thus, the CAR is variable at the diagnosis, as well as before and after gastrectomy. However, the optimal timing of the evaluation of the CAR is not well defined. In addition, one-point measurement of the CAR might not be reproducible. Considering these factors, we hypothesize that measurement of the change in CAR during treatment would have a greater clinical impact in gastric cancer treatment than the measurement of the CAR at a single point. To confirm our hypothesis, we evaluated the clinical impact of change in the CAR in gastric cancer patients who received curative treatment.
Patients and Methods
Patients
Patients were selected based on the medical records of consecutive patients who underwent curative resection for gastric cancer at Kanagawa Cancer Center from 2013 to 2017. The inclusion criteria were as follows: (i) histologically proven adenocarcinoma, (ii) clinical stage I–III disease as evaluated according to the 15th Edition of the General Rules for Gastric Cancer published by the Japanese Gastric Cancer Association [12], (iii) curative gastrectomy as a primary treatment for gastric cancer, (iv) complete (R0) resection of gastric cancer with radical lymph node dissection, and (v) ≥ 16 harvested lymph nodes. We excluded the patients who underwent R1 or R2 resection and those who did not measure CAR during perioperative periods.
Surgical Procedure and Adjuvant Treatment
All patients underwent gastrectomy with nodal dissection. D1+ nodal dissection was performed for those with clinical stage IA disease, and D2 dissection was performed for those with clinical stage ≥ IB disease. Patients diagnosed with pathological II or III disease received S-1-based adjuvant chemotherapy within 6 weeks after surgery [13–15].
Measurement of the CAR
The CAR was calculated as the serum CRP level (mg/dl) divided by the serum albumin level (g/dl) measured 1 week before surgery and 1 month after surgery. The change in CAR was defined as follows: Change in CAR = CAR at 1 month after surgery − CAR at 1 week before surgery.
Follow-up
Patients were followed-up at outpatient clinics. Hematological tests and physical examinations were performed at least every 3 months for 5 years. The carcinoembryonic antigen and CA19 9 tumor marker levels were also checked at least every 3 months for 5 years. Patients underwent a computed tomography examination every 6–12 months until 5 years after surgery.
Evaluations and Statistical Analyses
The significance of differences in the change in CAR and clinicopathological parameters was determined using the chi-squared test. The Kaplan–Meier method was used to calculate the overall survival and recurrence-free survival curves. Univariate and multivariate survival analyses were performed using a Cox proportional hazards model. We used stepwise methods for multivariate analysis in the present study. P values of < 0.05 were considered to indicate statistical significance. The SPSS software program (v27.0 J Win; IBM, Armonk, NY, USA) was used for all statistical analyses. This study was approved by the IRB of Kanagawa Cancer Center.
Results
Patients
We investigated 458 gastric cancer patients in the present study. Among them, 307 patients were male, and 322 patients were > 65 years of age. Sixty-seven patients had postoperative complications. The median CRP value before treatment was 0.07 (range: 0.01–1.54), the median albumin value was 4.1 (range: 2.3–5.1), and the median CAR was 0.01 (range: 0.002–1.543). The median CRP value after treatment was 0.1 (range: 0.01–16.43), the median albumin value was 4. (range: 1.4–4.9), and the median CAR value was 0.025 (range: 0.002–5.476).
Survival Analysis
The OS stratified by each clinical factor was compared using a log-rank test, and a significant difference was observed using a change in CAR of 0.05 (Table 1). When the patient background factors were compared between the high-change (change in CAR ≥ 0.05) and low-change (change in CAR < 0.05) groups, the median age, sex ratio, T factor, and N factor were similar. Each clinicopathological factor was categorized as shown in Table 2 and analyzed for its prognostic significance. The univariate and multivariate analyses for OS showed that pathological N factor, vascular invasion, and change in CAR were significant prognostic factors. The change in CAR was therefore selected for the final multivariate analysis model. In the low-change group, the OS rates at 3 and 5 years after surgery were 94.1% and 87.6%, respectively, while those in the high-change group were 83.6 and 77.5%, which amounted to a significant difference. The OS curves are shown in Fig. 1. The univariate and multivariate analyses of factors associated with RFS showed that the change in CAR was a significant prognostic factor. The change in CAR was selected as a significant prognostic factor for the final multivariate analysis model (Table 3). In the low-change group, the RFS rates at 3 and 5 years after surgery 90.1% and 85.1%, respectively, while those in the high-change group were 77.6 and 75.2%. The RFS curves are shown in Fig. 2. Table 1. Patient characteristicsCharacteristicsNo. of patients (%)1 year OS rate (%)3-year OS rate (%)5-year OS rate (%)p valueAge (years)0.047 < 65136 (29.7%)99.397.091.2 ≥ 65322 (70.3%)97.589.383.0Gender0.059 Man307 (67.0%)98.090.483.2 Woman151 (37.0%)98.093.990.0Pathological type0.512 Intestinal216 (47.2%)98.193.086.4 Diffuse242 (52.8%)97.990.284.7UICC T status < 0.001 T1285 (62.2%)98.996.192.4 T2 to T3173 (37.8%)96.584.773.8Lymph node metastasis < 0.001 Negative332 (72.5%)98.596.091.9 Positive126 (27.5%)96.879.767.8Lymphatic invasion < 0.001 Negative316 (69.0%)98.194.991.3 Positive142 (31.0%)97.984.972.1Vascular invasion < 0.001 Negative260 (56.8%)99.297.793.7 Positive198 (43.2%)96.484.174.4Change of CAR0.008 < 0.05359 (78.4%)98.994.187.6 0.05 ≤99 (21.6%)94.983.677.5Postoperative complications0.653 Yes67 (14.6%)97.089.383.0 No391 (85.4%)98.292.085.9OS Overall survival, UICC Union for International Cancer Control, CAR C-reactive protein albumin ratioTable 2Uni and multivariate Cox proportional hazard analysis of clinicopathological factors for overall survivalFactorsNoUnivariate analysisMultivariate analysisOR95% CI**p valueOR95% CI**p valueAge (years)0.051 < 651361.000 65 ≦3221.9200.997–3.698Gender0.063 Woman1511.000 Man3071.7940.969–3.321Pathological type Intestinal2161.0000.512 Diffuse2421.1880.710–1.986UICC T status < 0.001 T12851.000 T2–T41733.9322.277–6.793Lymph node metastasis < 0.001 < 0.001 Negative3321.0001.000 Positive1264.5302.691–7.6252.9581.705–5.132Change of CAR0.0090.046 < 0.053591.0001.000 0.05 ≤ 992.0541.198–3.5231.7331.009–2.978Lymphatic invasion < 0.001 Negative3161.000 Positive1423.6132.147–6.079Vascular invasion < 0.001 < 0.001 Negative2601.0001.000 Positive1984.9072.690–8.9483.2421.714–6.129Postoperative complications0.653 No3911.000 Yes671.1690.592–2.308UICC Union for International Cancer ControlFig. 1Overall survival in gastric cancer patients with high change in CAR (≥ 0.05) and low change in CAR (< 0.05)Table 3. Uni and multivariate Cox proportional hazards analysis of clinicopathological factors for recurrence free survivalFactorsNoUnivariate analysisMultivariate analysisOR95% CI**p valueOR95% CI**p valueAge (years)0.059 < 651361.000 65≦3221.7250.979–3.041Gender0.347 Woman1511.000 Man3071.2750.769–2.113Pathological type0.377 Intestinal2161.000 Diffuse2421.2300.777–1.949UICC T status < 0.001 T1–T22851.000 T3–T41733.3262.071–5.341Lymph node metastasis < 0.001 < 0.001 Negative3321.0001.000 Positive1264.5232.847–7.1852.5551.491–4.378Change of CAR0.0080.020 < 0.053591.0001.000 0.05 ≤ 991.9421.193–3.1591.7921.098–2.927Lymphatic invasion < 0.0010.021 Negative3161.0001.000 Positive1423.8072.392–6.0601.9031.101–3.291Vascular invasion < 0.0010.023 Negative2601.0001.000 Positive1983.6152.194–5.9561.9091.092–3.336Postoperative complications0.264 Yes3911.000 No671.3940.779–2.494Fig. 2Recurrence-free survival in gastric cancer patients with high change in CAR (≥ 0.05) and low change in CAR (< 0.05)
Postoperative Course of the Low-Change and High-Change Groups
When the postoperative course of the two groups was compared, there were some differences in the incidence of postoperative surgical complications and the incidence of other-cause deaths. The incidence of postoperative complications was 32.3% (32/99) in the high-change group and 9.7% (35/359) in the low-change group. The incidence of surgical complications in the high-change group was significantly higher than that in the low-change group (p = 0.009). The incidence of other causes of death was in the high-change and low-change groups was 10.1% (10/99) and 3.6% (13/359), respectively, which amounted to a significant difference (p < 0.001). Furthermore, there was a significant difference between the two groups in the site of first relapse at lymph node metastasis (Table 4). Table 4. Patterns of recurrence between the patients with C-reactive protein albumin ratio < 0.05 and those with C-reactive protein albumin ratio 0.05 ≤ Recurrence siteAll cases (n = 458)C-reactive protein albumin ratiop value < 0.05 (n = 359)0.05 ≤ (n = 99)Number%Number%Number%Peritoneal173.7143.933.00.685Hematological163.5113.155.10.341Lymph node132.851.488.1< 0.001Local site40.841.1000.291
Discussion
The aim of the present study was to clarify the clinical impact of change in CAR in gastric cancer patients who received curative treatment. The major finding is that a change in CAR is a significant risk factor in gastric cancer patients. In addition, a higher change in CAR is related to postoperative complications and lymph node recurrence. Therefore, a change in CAR is a promising prognostic factor for gastric cancer patients.
In the present study, the high-change CAR (≥ 0.05) group had a significantly poorer prognosis in comparison to the low-change CAR (< 0.05) group (hazard ratio: 1.733, 95% confidence interval: 1.009–2.978, p = 0.0049). Moreover, the 5-year OS rates of the high-change CAR group and low-change CAR group were 77.5% and 87.6%, respectively. Although limited studies have evaluated the clinical impact in malignancies, similar results were observed in previous studies. Oshima et al. evaluated the changes and prognostic impact of inflammatory nutritional factors during neoadjuvant chemoradiation therapy in 49 patients with resectable pancreatic cancer [16]. They found that high change in CAR (≥ 0.077) after chemoradiation therapy were significantly associated with shorter OS. The median OS was 23.1 months in patients with a high change in CAR and 64.1 months in those with a low change in CAR. In addition, change in CAR after chemoradiation therapy were a prognostic factor (hazard ratio: 5.1842, p = 0.0036). Moreover, Ikoma et al. evaluated the clinical impact of change in CAR in 97 gastric cancer patients who received immune checkpoint inhibitor therapy [17]. They found that patients with low change in CAR (≤ 0.01) during immune checkpoint inhibitor therapy had better survival than those with high change in CAR (> 0.01). The median OS was 9.4 months in the patients with low change in CAR and 4.5 months in those with high change in CAR; the difference was statistically significant (p = 0.002). In addition, the univariate and multivariate analyses showed that low change in CAR was a prognostic factor (HR 0.59; 95% CI 0.37–0.93; p = 0.002). Considering our results and previous reports, the change in CAR during cancer treatment might be a promising prognostic factor.
Recently, the change in CAR during treatment might be not only a promising prognostic factor but also a promising nutritional assessment tool for nutritional intervention. To date, there have been various nutritional/anti-inflammatory treatment studies for malignancy patients during cancer treatment [18, 19]. However, limited studies have shown only positive results, and there are no definitive nutritional/anti-inflammatory treatments. One possible reason is the difficulty of setting an endpoint. Although previous studies, including our studies, focused on body weight or lean body mass, the effect of nutritional/anti-inflammation treatment during cancer treatment on weight and muscle was much smaller than expected, and the difference may not have been detectable. On the other hand, the change in CAR might indicate small change in nutritional/anti-inflammatory treatment during cancer treatment. For example, Silva et al. conducted a clinical trial to evaluate the systemic inflammatory response to eicosapentaenoic acid (EPA) in 29 colorectal cancer patients [20]. The patients who were assigned to the supplemental group received 2 g of fish oil containing 600 mg of EPA and docosahexaenoic acid (DHA). When the change in CAR between baseline and 9 weeks after chemotherapy was compared, the patients who received EPA showed a clinically relevant decrease in their C-reactive protein/albumin ratio (p = 0.005).
They found that low doses of fish oil supplementation can positively modulate the nutritional status and C-reactive protein/albumin ratio. Considering these factors, change in the CAR might become promising predictive markers of nutritional/anti-inflammatory treatment during cancer treatment.
To introduce change in CAR as a parameter in daily clinical practice, it is necessary to set the optimal cutoff value. In the present study, we set the cutoff value of change in CAR at 0.05 according to the 1-, 3-, and 5-year survival rates. Several values of the change in CAR have been described in previous studies. Oshima et al. set the cutoff value of change in CAR at 0.077, and Ikoma et al. set it at 0.01. These differences might be due to the following reasons. First, the number of patients and patient background factors were different. Our study (n = 458) evaluated resectable gastric cancer, Ikoma et al. evaluated unresectable gastric cancer (n = 97), and Oshima et al. evaluated pancreatic cancer (n = 49). Second, the methods used to evaluate change in CAR were different. Our study evaluated the cutoff value of change in CAR according to the survival rate, while other studies evaluated the cutoff value of change in CAR according to a receiver operating characteristic curve. These differences might have affected the cutoff value. Further studies are needed to establish the optimal evaluation method and optimal cutoff value of change in CAR.
The present study was associated with some limitations. First, this was a retrospective study with a small sample size from a single institution. Therefore, our study might have a selection bias. Second, there might be time bias in the present study. Our study included data from 2012 to 2017. During this period, perioperative care and perioperative adjuvant treatment were improved. Third, in the present study, the incidence of other-cause death was significantly higher in the high-change group than in the low-change group. However, the reason for this issue is unclear. Considering these factors, our results need to be validated in another large cohort.
In conclusion, change in CAR during treatment is a significant risk factor and in gastric cancer patients and is therefore a promising prognostic factor. In addition, the changes of inflammation status during perioperative periods might be a promising prognostic factor for gastrointestinal cancer patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2020;71:209–249. 10.3322/caac.21660. PMID: 33538338. 10.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68: 394–424. 10.3322/caac.21492. PMID: 30207593. 10.3322/caac.2149230207593 · doi ↗ · pubmed ↗
- 3Aoyama T, Yoshikawa T. Adjuvant therapy for locally advanced gastric cancer. Surg Today. 2017;47:1295–1302. 10.1007/s 00595-017-1493-y. PMID: 28251375.10.1007/s 00595-017-1493-y 28251375 · doi ↗ · pubmed ↗
- 4Yoshikawa T, Rino Y, Yukawa N, Oshima T, Tsuburaya A, Masuda M. Neoadjuvant chemotherapy for gastric cancer in Japan: a standing position by comparing with adjuvant chemotherapy. Surg Today. 2014;44:11–21. 10.1007/s 00595-013-0529-1. PMID: 23508452.10.1007/s 00595-013-0529-123508452 · doi ↗ · pubmed ↗
- 5Kanda M, Kodera Y, Sakamoto J. Updated evidence on adjuvant treatments for gastric cancer. Expert Rev Gastroenterol Hepatol. 2015;9:1549–60. 10.1586/17474124.2015.1094373. PMID: 26414453.10.1586/17474124.2015.109437326414453 · doi ↗ · pubmed ↗
- 6Pentheroudakis G, ESMO Guidelines Committee. Recent e Updates to the ESMO Clinical Practice Guidelines on hepatocellular carcinoma, cancer of the pancreas, soft tissue and visceral sarcomas, cancer of the prostate and gastric cancer. Ann Oncol. 2019;30:1395–1397. 10.1093/annonc/mdz 180. PMID: 31168599.10.1093/annonc/mdz 18031168599 · doi ↗ · pubmed ↗
- 7Muro K, Van Cutsem E, Narita Y, Pentheroudakis G, Baba E, Li J, Ryu MH, Zamaniah WIW, Yong WP, Yeh KH, Kato K, Lu Z, Cho BC, Nor IM, Ng M, Chen LT, Nakajima TE, Shitara K, Kawakami H, Tsushima T, Yoshino T, Lordick F, Martinelli E, Smyth EC, Arnold D, Minami H, Tabernero J, Douillard JY. Pan-Asian adapted ESMO Clinical Practice Guidelines for the management of patients with metastatic gastric cancer: a JSMO-ESMO initiative endorsed by CSCO, KSMO, MOS, SSO and TOS. Ann Oncol. 2019;30:19–33. 10.10 · doi ↗ · pubmed ↗
- 8Aoyama T. Perioperative body composition changes in the multimodal treatment of gastrointestinal cancer. Surg Today. 50:217–222, 2020. 10.1007/s 00595-019-01815-8. PMID: 31028458.10.1007/s 00595-019-01815-831028458 · doi ↗ · pubmed ↗