Infant Barlow’s Disease in Association with Atrial Septal Defect
Isaac Azevedo Silva, Larissa Ales Leite Matos, Carolina Sant’Anna, Ulisses Alexandre Croti

TL;DR
A seven-year-old girl with rare heart conditions underwent surgery to repair her mitral valve and atrial septal defect.
Contribution
A case report of mitral valve regurgitation and Barlow’s disease in association with an atrial septal defect, highlighting the rarity and treatment approach.
Findings
Echocardiography confirmed Barlow’s disease and an ostium secundum atrial septal defect.
The patient underwent successful mitral valvuloplasty and patch atrioseptoplasty.
Mitral valve repair is emphasized as the preferred treatment for such rare conditions.
Abstract
Clinical data: Female, seven years old, referred to our service complaining about congestive heart failure symptoms due to mitral valve regurgitation and atrial septal defect. Technical description: Echocardiographic findings compatible with Barlow’s disease and atrial septal defect, ostium secundum type. Operation: She was submitted to mitral valvuloplasty with chordal shortening and prosthetic posterior ring (Gregori-Braile®) along with patch atrioseptoplasty. Comments: Mitral valve regurgitation is a rare congenital heart disease and Barlow’s disease is probably rarer. Mitral valve repair is the treatment of choice.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2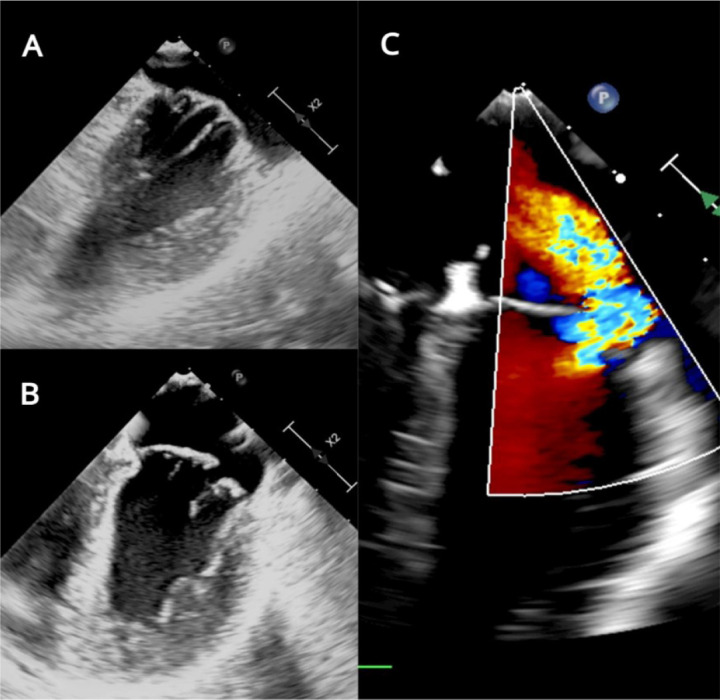 Figure 3
Figure 3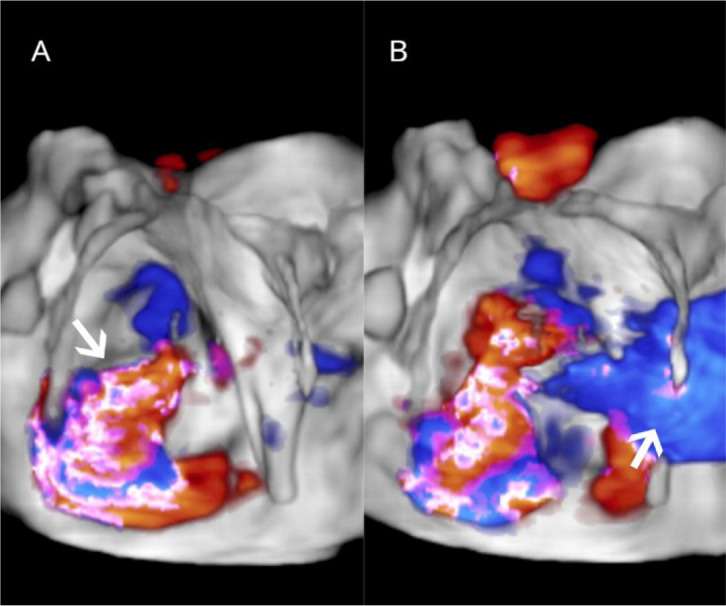 Figure 4
Figure 4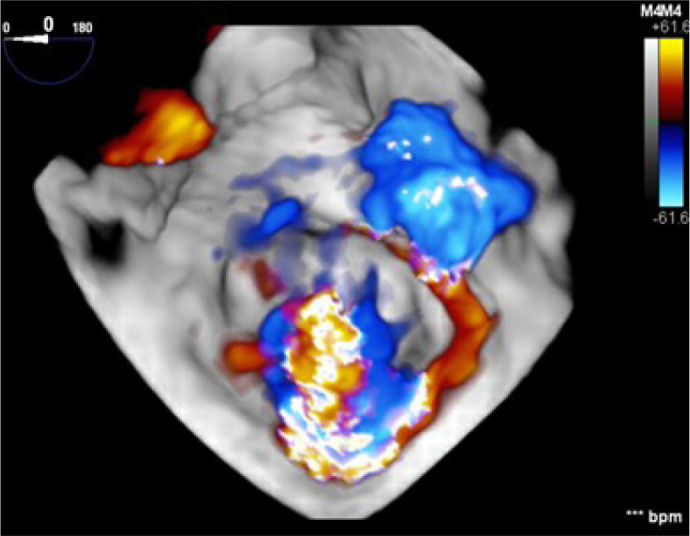 Figure 5
Figure 5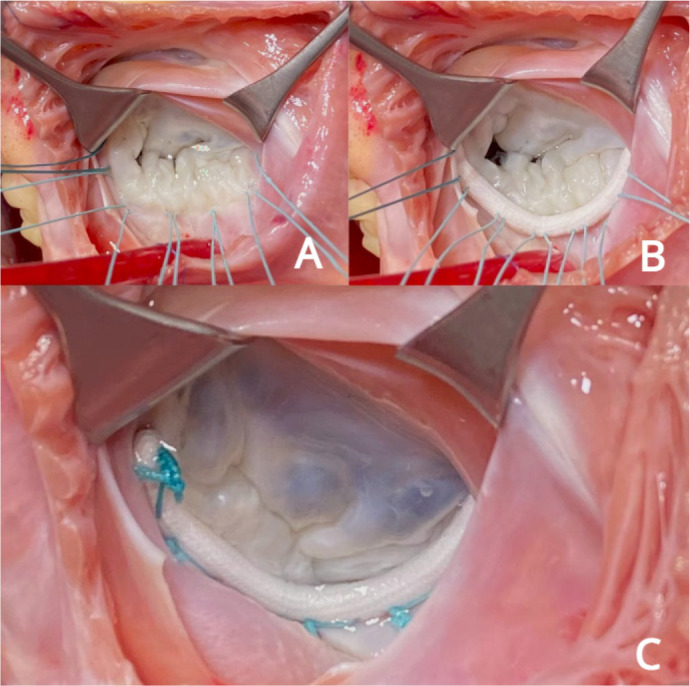 Figure 6
Figure 6| Abbreviations, Acronyms & Symbols | |
|---|---|
| ASD | = Atrial septal defect |
| BD | = Barlow’s disease |
| MV | = Mitral valve |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Cardiac Arrhythmias and Treatments · Pericarditis and Cardiac Tamponade
CASE PRESENTATION
Clinical Data
**: **
Female, seven years old, weighting 23.9 kg, height 1.25 m, with a history of long-term exertional dyspnea, referred to our hospital due to progressive worsening of symptoms. She was diagnosed at seven years old with atrial septal defect (ASD) and mitral valve (MV) prolapse and regurgitation, and since then, she has been on medical therapy.
On admission, the patient was New York Heart Association class II for congestive heart failure.
TECHNICAL DESCRIPTION
Chest Radiography
Chest radiography shows increased pulmonary vascular markings, no pulmonary edema, and mild cardiomegaly with cardiothoracic ratio of 0.55 (Figure 1).
Fig. 1. Chest radiography with prominent pulmonary vascular markings and mild cardiomegaly.
Electrocardiography
Sinus rhythm (S QRS 106°), PR interval of 155 ms, QRS of 78 ms, QTc of 432 ms, heart rate of 88 bpm, and left atrial enlargement.
Transesophageal Echocardiography
Situs solitus in levocardia, usual venoatrial, atrioventricular, and ventriculoarterial connections.
Presence of ostium secundum ASD of 14 mm with left to right shunt (Figure 2). Normal biventricular ejection fraction, enlargement of right cardiac chambers and left atrium, and noticeable MV insufficiency (Figures 3C, 4A, 4B).
Fig. 2. Apical four-chamber transesophageal echocardiogram, two-dimensional view. A) Imaging with probe rotated toward right-sided structures, showing dropout in mid-septum between the left atrium and right atrium consistent with ostium secundum atrial septal defect (ASD). B) Addition of color Doppler shows left-to-right shunt through the ASD.
Fig. 3. Transesophageal echocardiogram, two-dimensional view of mitral valve. A) Prolapsed, thickened, and elongated chordae tendineae. B) Failure of coaptation and billowing anterior segments (A2 and A3) and posterior scallops (P2 and P3). C) Addition of color Doppler shows severe mitral regurgitation.
Fig. 4. Three-dimensional echocardiogram image of the mitral valve from the left atrial perspective. Color Doppler demonstrates valve regurgitation (arrow) (A) and left-to-right shunt through the atrial septal defect (arrow) (B).
MV features included annular dilation, leaflet redundancy, with failure of coaptation between A2-A3 and P2-P3, associated with multisegmental prolapsing/billowing MV components, and thickened, elongated chordae tendineae, typical of Barlow’s disease (BD) (Figures 3A, 3B, 5).
Fig. 5. Three-dimensional image from the left atrial perspective demonstrating features typical of Barlow’s disease with severe mitral regurgitation, annular dilation, leaflet redundancy, and multisegmental prolapsing/billowing mitral valve components.
No abnormalities in other valves. Additional findings were unremarkable.
Operation
After median sternotomy, cardiopulmonary bypass was established with bicaval and ascending aorta cannulation. A single dose of antegrade cold crystalloid cardioplegia, Custodiol-HTK® (GmbH, Bensheim, Germany), was given. Through left atriotomy in interatrial groove, the MV was evaluated confirming echocardiographic findings (Figure 6A).
Fig. 6. Surgical aspect of the mitral valve from atrial view. A) After atriotomy, with ring repair sutures in place (note diffuse thickening of the anterior leaflet with failure of coaptation between A2-A3 and P2-P3). B) Imaging after implantation of a rigid 26 mm posterior ring (Gregori-Braile®). C) Final aspect with ring in place and proper coaptation of the leaflets after testing with saline solution (NaCl 0.9%).
MV repair was performed by chordal shortening and implantation of rigid 26 mm posterior ring (Gregori-Braile®, Braile Biomédica, São José do Rio Preto/São Paulo, Brazil) (Figures 6B, 6C). The ostium secundum ASD was closed with bovine pericardial patch.
Transesophageal echocardiogram was performed after cardiopulmonary bypass weaning, showing minimal MV regurgitation, no residual shunts, and preserved biventricular function.
COMMENT
Congenital MV lesions are a rare and particularly degenerative MV disease. An echocardiographic study detected MV congenital malformations in approximately 0.5% of 13,400 subjects^[1,2]^. There is no clear information about the incidence of BD in infants and children. Indeed, the diagnosis of BD, even in adults, has been raising concerns, as shown by Carpentier’s group^[3]^.
Histologically, normal MV tissue consists of three layers. The atrialis, on the atrial side, is rich in elastic fibers, providing elasticity to the valve. The spongiosa, in the middle, is made of glycosaminoglycans and proteoglycans, supplying flexibility to the valve, absorbing vibrations. And the fibrosa, on the ventricular side, is the thickest part of the leaflet and is rich in collagen fibers, providing tensile strength to the valve^[4]^.
In BD, the organization of the three layers is disrupted. Collagen and elastin fibers are fragmented, and the spongiosa layer expands due to accumulation of proteoglycans, characteristic of myxomatous degeneration, and infiltrates the fibrosa layer^[3]^.
On echocardiography, BD is characterized by a diffuse, leaflet redundancy, with bileaflet prolapse or prolapse of multiple segments. Valve leaflets are also often thickened (> 3 mm) as measured in diastole using the M-mode. Chordae are also frequently thickened and chordal elongation is more common than chordal rupture^[5]^.
MV regurgitation was the classical manifestation of BD, and repair with a prosthetic posterior ring has been proved to allow better outcomes than with complete rings^[6]^.
In this presented case, echocardiographic landmarks of BD were found and confirmed on surgical exploration. A no-resection MV repair was successfully achieved through chordal shortening and prosthetic posterior annulus approach along with ASD closure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mitchell SC Korones SB Berendes HW. Congenital heart disease in 56,109 births. Incidence and natural history Circulation 197143332333210.1161/01.cir.43.3.3235102136 · doi ↗ · pubmed ↗
- 2Banerjee A Kohl T Silverman NH. Echocardiographic evaluation of congenital mitral valve anomalies in children Am J Cardiol 199576171284129110.1016/s 0002-9149(99)80357-97503011 · doi ↗ · pubmed ↗
- 3Fornes P Heudes D Fuzellier JF Tixier D Bruneval P Carpentier A. Correlation between clinical and histologic patterns of degenerative mitral valve insufficiency: a histomorphometric study of 130 excised segments Cardiovasc Pathol 199982819210.1016/s 1054-8807(98)00021-010724505 · doi ↗ · pubmed ↗
- 4Schoen FJ. Evolving concepts of cardiac valve dynamics: the continuum of development, functional structure, pathobiology, and tissue engineering Circulation 2008118181864188010.1161/CIRCULATIONAHA.108.80591118955677 · doi ↗ · pubmed ↗
- 5van Wijngaarden AL Kruithof BPT Vinella T Barge-Schaapveld DQCM Ajmone Marsan N. Characterization of degenerative mitral valve disease: differences between fibroelastic deficiency and barlow's disease J Cardiovasc Dev Dis 2021822310.3390/jcdd 802002333671724 PMC 7926852 · doi ↗ · pubmed ↗
- 6Gregori Jr F Silva SS Moure O Takeda R Façanha L Ribeiro I Surgical treatment of mitral insufficiency in children: ten years of reparative techniques Braz J Cardiovasc Surg 19894320220910.1590/S 0102-76381989000300004 · doi ↗