Abiraterone-Induced Secondary Hypertension: Two Wrongs Don’t Make a Right
Achilleas Betsikos, Eleni Paschou, Virginia Geladari, Stauroula Magaliou, Nikolaos Sabanis

TL;DR
Abiraterone, a prostate cancer drug, can cause severe hypertension and other issues even with prednisolone use.
Contribution
Reports a case of abiraterone-induced mineralocorticoid excess despite prednisolone.
Findings
Abiraterone caused secondary hypertension and hypokalemia.
Metabolic alkalosis and elevated ACTH levels were observed.
Prednisolone failed to prevent the mineralocorticoid excess.
Abstract
Abiraterone, an inhibitor of both 17α-hydroxylase and 17,20-lyase, is considered a novel, state-of-the-art, life-prolonging therapy in the urologists’ arsenal when treating prostate cancer. Despite its efficacy, it is linked with an increased risk of cardiovascular adverse effects. Herein, we report a case in which the administration of abiraterone resulted in a full-blown syndrome of apparent mineralocorticoid excess despite the concomitant administration of prednisolone; that is, secondary hypertension, hypokalemia, metabolic alkalosis, as well as elevated levels of adrenocorticotropic hormone (ACTH).
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
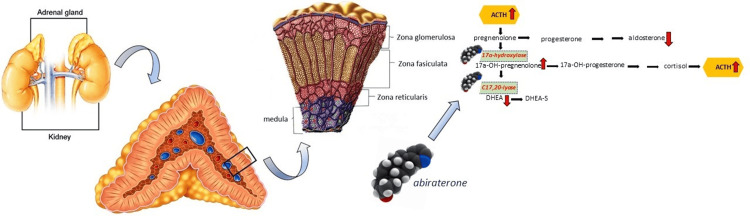 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsProstate Cancer Treatment and Research · Sexual Differentiation and Disorders · Adrenal and Paraganglionic Tumors