Improving Post-Injury Follow-up Survey Response: Incorporating Automated Modalities
Hannah Scheuer, Kelsey M. Conrick, Brianna Mills, Esther Solano, Saman Arbabi, Eileen M. Bulger, Danae Dotolo, Christopher St. Vil, Monica S. Vavilala, Ali Rowhani-Rahbar, Megan Moore

TL;DR
This study shows that using automated methods like email and text can improve response rates for post-injury follow-up surveys in trauma patients.
Contribution
The study introduces a low-cost, automated approach to improve follow-up survey response rates in trauma care systems.
Findings
Response rates increased by 17.9 percentage points after implementing automated modalities.
Email and text became the primary response modalities in the second protocol.
Automated methods show promise for expanding longitudinal data in trauma registries.
Abstract
Incorporating post-discharge data into trauma registries would allow for better research on patient outcomes, including disparities in outcomes. This pilot study tested a follow-up data collection process to be incorporated into existing trauma care systems, prioritizing low-cost automated response modalities. This investigation was part of a larger study that consisted of two protocols with two distinct cohorts of participants who experienced traumatic injury. Participants in both protocols were asked to provide phone, email, text, and mail contact information to complete follow-up surveys assessing patient-reported outcomes six months after injury. To increase follow-up response rates between protocol 1 and protocol 2, the study team modified the contact procedures for the protocol 2 cohort. Frequency distributions were utilized to report the frequency of follow-up response…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
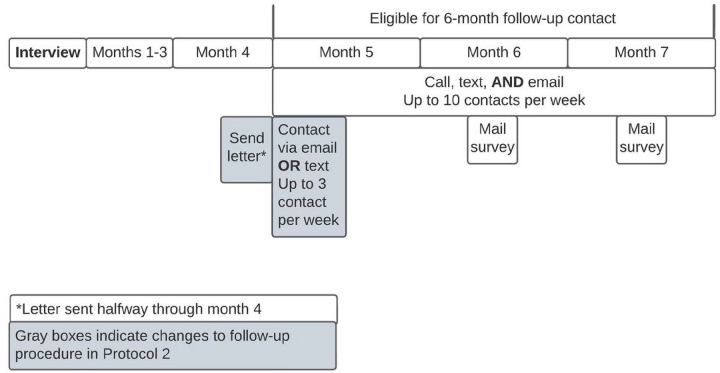 Figure 1
Figure 1- —National Institute on Minority Health and Health Resources of the National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraffic and Road Safety · Injury Epidemiology and Prevention · Trauma and Emergency Care Studies
Background
Trauma patient follow-up in the United States (US) has challenged researchers and trauma care teams for decades.^1^ Data from US trauma patients’ medical records are abstracted into local, state, and national trauma registries to guide intervention and prevention efforts, direct quality improvement, track patient health trajectories and outcomes, and examine the ways in which provider and systemic factors may contribute to disparities in outcomes.^2,3^ However, current gaps in this system limit researchers’ ability to identify groups at highest risk for disparities in functional recovery. Prior research has established the need for a data collection system to collect long-term follow-up data from patients after injury.^4–6^ Despite this critical need, and the successful implementation of follow-up procedures in many other countries,^7,8^ post-discharge follow-up in the US has remained a considerable challenge. Moreover, significant disparities exist in trauma care follow-up, with persons of color and those with higher poverty and lower education levels consistently presenting lower follow-up rates.^9^ Given these gaps in data collection, there is a significant need for a feasible, cost-effective, and culturally resonant follow-up data collection process to be incorporated into existing trauma care systems.
The COVID-19 pandemic has presented additional challenges to reaching patients after discharge. With pandemic-related restrictions on in-person contact and post-discharge follow-up, data collection has been and continues to be adapted to virtual modalities including text and email. Prior research with hard-to-reach trauma populations, including patients with increased environmental instability and/or co-occurring mental health and substance use disorders, has consisted of persistent and intensive follow-up outreach efforts, with limited success.^10^ These efforts are not sustainable long-term or feasible in the context of the COVID-19 pandemic, and there is a need for follow-up methods that reduce the burden on research and hospital staff. National trauma care experts have expressed an interest and need to find a feasible, cost-effective, and low-burden method to follow-up with trauma patients.^4^ Moreover, trauma registry experts have noted that due to limited resources, calling patients individually is not feasible for long-term follow-up, and an automated system is needed.^4^
The current study assessed post-injury survey response rates across different outreach modalities including mail, telephone, text, and email to determine feasibility of collecting patient-reported follow-up data from trauma patients 6 months after hospital admission, as well as most efficient data collection modalities.
Methods
Design
This study was part of a larger prospective cohort study conducted at a level-1 trauma center in the Pacific Northwest. Interviews were conducted with n = 245 racially and ethnically diverse trauma patients to develop a culturally resonant data collection system for equity-related measures. Six months after enrollment, study participants were contacted to complete the PROMIS-29,^11^ a follow-up health-related quality of life survey measure. To test the feasibility of an automated system, researchers used Twilio, a low-cost (0.007) module within the Research Electronic Data Capture (REDCap) survey platform^[12](#R12),[13](#R13)^ that automatically sends text messages or emails at specified intervals. All participants were given a 10 gift card upon completion of the interview. Study procedures were approved by the University Institutional Review Board (IRB). The STROBE guidelines were used to ensure proper reporting of methods, results, and discussion.
Eligibility
Potentially eligible patients were identified via electronic medical record review. Inclusion criteria were: 18 years or older, admitted for at least 24 hours with a physical injury (preliminary ICD-10 codes S00-T88 or V00-Y99), and had the ability to consent and interview in English or Spanish. Patients were excluded if they had a burn injury, were under law enforcement supervision, were under care for a secondary complication to a prior injury sustained more than 2 weeks prior to screening, or were unable to consent to participate in research as judged by nursing staff (e.g., those with cognitive impairments).
Recruitment and Procedure
We used a purposive sampling strategy to ensure a racially and ethnically diverse sample. The recruitment process was modified because of changes to study site procedures due to the COVID-19 pandemic (Table 1). Protocol 1. Patients in protocol 1 were enrolled from 6/24/19 to 3/6/2020. These patients were approached by the bedside, provided with the purpose of the study, consented, and completed a 25–40-minute audio-recorded interview (SDC). Participants (N = 136) were asked to provide their phone, email, and mailing address, as well as additional contact information for two friends or relatives, their work, and their health clinic. Six months later, patients were contacted up to 10 times per week via multiple simultaneous outreach methods including phone, text, e-mail, and mail. They were asked to participate in a 10-minute interview during which they completed the PROMIS-29, a short form assessment containing one pain intensity question and four items from seven domains: depression, anxiety, physical function, pain interference, fatigue, sleep disturbance, and ability to participate in social roles and activities.^11^ Participants were eligible to complete the follow-up survey from 5–7 months after initial interview. In an effort to yield high follow-up response rates,^10^ research staff prioritized contacting patients for follow-up in as many ways possible and engaged in phone, text message, and email outreach concurrently (Fig. 1). Paper surveys with return postage were sent to participants who had not responded during second week of months 6 and 7 after interview. Protocol 2. Due to restrictions on in-person contact stemming from the COVID-19 pandemic, recruitment for protocol 2 patients was conducted remotely from 4/15/2020–8/30/2020. Potentially eligible patients were called while they were admitted to the hospital and offered the option to participate in the interview then or be contacted again post-discharge. Potentially eligible patients who had already been discharged from the hospital were contacted by phone up to 10 times in the two weeks after discharge. Once they had consented to participation and completed the interview, participants were asked to provide the same contact information as protocol 1 participants.
To increase follow-up survey response rates and further test the feasibility of low-cost automated contact options (i.e., text and email sent through Twilio), the study team implemented a new 6-month follow-up contact procedure during the COVID-19 pandemic (Fig. 1). Prior research demonstrates that sending a letter before asking participants to complete follow-up surveys increased telephone survey response rate by 11%.^14^ In line with this evidence, the investigative team sent a letter by mail to participants (N = 109) two weeks prior to them being eligible for 6-month follow-up; participants were eligible to complete the survey 5–7 months after initial interview. Additionally, in line with prior literature demonstrating increased response rates when offering only one response modality at a time,^15^ participants were only offered one modality (either text or email) for the first 1–2 weeks of eligibility (Fig. 1). Paper surveys with return postage were sent to participants who had not responded during second week of months 6 and 7 after interview.
Data Analysis
Once participants completed the follow-up survey, research staff recorded the modality by which the participant responded. Descriptive statistics were used to summarize participant demographics, report the frequency of follow-up response by modality, and overall response rates.
Results
A total of 178 individuals out of 245 eligible participants responded to the 6-month follow-up survey: 88 using protocol 1 and 90 using protocol 2 (Table 2). Overall response rate was 64.7% for protocol 1 and 82.6% for protocol 2. Most (n = 124; 69.6%) self-identified as persons of color.
Overall, after implementing new follow-up contact procedures, the response rate by any modality increased by 17.9 percentage points from protocol 1 (64.7%) to protocol 2 (82.6%). In protocol 1, the primary response modality was by phone (72.7%), and email and text only made up a combined 12.5% of responses. In contrast, the combination of email (47.8%) and text (14.4%) made up more than half of the responses during use of protocol 2 (62.2%), with phone accounting for only 35.6%. Mail responses also decreased between the two phases (14.8–2.2%).
The 90 participants from protocol 2 who responded to the 6-month follow-up survey were asked if they had received the letter indicating they would be soon contacted to complete the follow-up. Among these, 53.3% (n = 48) indicated they recalled receiving the letter. These individuals were additionally asked how receiving the letter influenced their willingness to respond to the survey; 47.9% (n = 23) indicated the letter made them more likely to respond, 47.9% (n = 23) indicated the letter did not influence their likelihood of responding, and 4.2% (n = 2) indicated the letter made them less likely to respond.
Discussion
The current study is an innovative test of the feasibility of collecting follow-up data from racially and ethnically diverse patients in the US who have experienced injury via cost-efficient and low-burden automated modalities including text and e-mail. Findings from this investigation reveal that the implementation of a follow-up outreach procedure that included sending a letter two weeks prior to requests for follow-up completion and reducing the number of options for initial contact was associated with an increase in response rate. Furthermore, implementation of this purposeful modification in outreach procedure changed the most common response modality from phone, a higher cost and higher administrator burden modality, to a combination of email and text message, which may be automated and therefore more cost-efficient alternatives. Taken together, our results suggest that follow-up data can feasibly be collected from trauma patients by implementing an automated and cost-efficient data collection process.
This investigation identifies several areas for future research. First, this investigation is US centric and does not consider successful post-discharge follow-up procedures that have been implemented in other countries.^7,8^ Future research should be informed by lessons learned from successful post-discharge follow-up efforts implemented in other countries. While this study did not assess patient preference for follow-up outreach modality, recent evidence suggests that patients who speak a language other than English may have specific preferences for non-phone outreach.^16^ Assessing patient preference should be a priority in future studies. Furthermore, recent concerns have been raised regarding cybersecurity specifically with Twilio and REDCap.^17^ Although the current investigation does not have the means to address these concerns, cybersecurity remains a critical issue and must be addressed in future research.
While this study offers important insights into follow-up with hard-to-reach trauma populations, limitations must be noted. Results from this investigation could be impacted by selection bias. Due to COVID-19, recruitment procedures were solely remote for some of the participants. With remote recruitment, these participants had to answer the phone in order to be enrolled in the study, whereas protocol 1 participants were approached and enrolled by the bedside. This difference in recruitment strategies could suggest fundamental differences between cohorts. There were also several changes made between the two protocols and investigators cannot be sure whether improvement in response rate is due to one change or a combination of the changes. Additionally, future research should include a detailed cost analysis to ensure that costs of implementing this follow-up protocol are sustainable. Finally, all study participants were recruited from one level-1 trauma center located in the northwest. Further research is needed to ensure findings are generalizable on a national scale.
Recent scholarship has established expert consensus on outcome measures for data collection from trauma patients.^6^ However, there is a demonstrated and significant need for the implementation of a feasible and cost-effective follow-up data collection process to be incorporated within existing trauma care systems. Trauma registry experts have identified that this system should prioritize automated data collection processes to increase willingness of trauma centers to implement procedures for long-term follow-up with trauma patients.^4^ This investigation provides evidence that the implementation of a cost-efficient and automated data collection process may be both feasible and effective for following up with US trauma patients and ultimately expanding the national trauma registry to include data crucial for promoting long-term positive outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aaland M, Marose K, Zhu T. The lost to trauma patient follow-up: a system or patient problem. J Trauma Acute Care Surg. 2012;73(6):1507–11.23147179 10.1097/TA.0b 013e 31826 fc 928 · doi ↗ · pubmed ↗
- 2Moore M, Conrick KM, Fuentes M, Research on Injury Disparities: A Scoping Review. Health Equity. 2019;3(1):504–11.31637361 10.1089/heq.2019.0044 PMC 6798805 · doi ↗ · pubmed ↗
- 3Surgeons A Co. National Trauma Data Bank. Accessed February 7 2022.
- 4Conrick K, Mills B, Mohamed K Improving Data Collection and Abstraction to Assess Health Equity in Trauma Care. Journal of Medical Systems. In Press.10.1007/s 10916-022-01804-435260929 · doi ↗ · pubmed ↗
- 5Graves J, Moore M, Vavilala M, Gonzalez C. 164 Health equity and injury: building community, research, and advocacy partnerships to address the national research and policy agenda. Inj Prev. 2017;23(Suppl 1):A 62–62.
- 6Herrera-Escobar JP, Price MA, Reidy E, Core Outcome Measures for Research in Traumatic Injury Survivors: The NTRAP Modified Delphi Consensus Study. J Trauma Acute Care Surg. 2022;92(5):916–23.35081596 10.1097/TA.0000000000003546 · doi ↗ · pubmed ↗
- 7Gabbe BJ, Sutherland AM, Hart MJ, Cameron PA. Population-Based Capture of Long-Term Functional and Quality of Life Outcomes After Major Trauma: The Experiences of the Victorian State Trauma Registry. In. Vol 69. The Journal of Trauma. 2010:532–536.10.1097/TA.0b 013e 3181 e 5125 b 20838122 · doi ↗ · pubmed ↗
- 8van der Vliet QMJ, Bhashyam AR, Hietbrink F, Houwert RM, Öner FC, Leenen LPH. Routine incorporation of longer-term patient-reported outcomes into a Dutch trauma registry. In. Vol 28. Qual Life Res. 2019:2731–2739.31098797 10.1007/s 11136-019-02211-y PMC 6761083 · doi ↗ · pubmed ↗