A randomized phase III double-blind placebo-controlled trial of first line chemotherapy and trastuzumab with or without bevacizumab for patients with HER2/neu-positive metastatic breast cancer: a trial of the ECOG-ACRIN Cancer Research Group (E1105)
Jessica Mezzanotte-Sharpe, Anne ONeill, Ingrid A. Mayer, Carlos L. Arteaga, Ximing J Yang, Lynne I. Wagner, David Cella, Neal J. Meropol, R. Katherine Alpaugh, Thomas J. Saphner, Robert E. Swaney, Karen L Hoelzer, William J. Gradishar, Vandana G. Abramson, P. Kothai Sundaram

TL;DR
This study tested whether adding bevacizumab to standard treatment improves outcomes for HER2-positive metastatic breast cancer patients, but found no significant benefit.
Contribution
The trial evaluated the efficacy of bevacizumab in combination with chemotherapy and trastuzumab for HER2-positive metastatic breast cancer.
Findings
Median progression-free survival was 11.1 months with placebo and 13.8 months with bevacizumab.
Median survival was 49.1 months with placebo and 63 months with bevacizumab.
Toxicities like hypertension and neutropenia were more common with bevacizumab.
Abstract
In 2008, bevacizumab received accelerated Food and Drug Administration (FDA) approval for use in human epidermal growth factor receptor 2 (HER2)-negative metastatic breast cancer (MBC). Based on the preclinical and preliminary clinical activity of the trastuzumab and bevacizumab combination, ECOG-ACRIN E1105 trial was developed to determine if the addition of bevacizumab to a chemotherapy and trastuzumab combination for first-line therapy would improve progression-free survival (PFS) in patients with HER2-positive MBC. 96 patients were randomized to receive standard first-line chemotherapy and trastuzumab with or without bevacizumab between November 2007 and October 2009, and 93 began protocol therapy. Induction therapy was given for 24 weeks, followed by maintenance trastuzumab with or without bevacizumab. 60% (56/93) began carboplatin and 74% (69/93) completed 6 cycles of induction…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
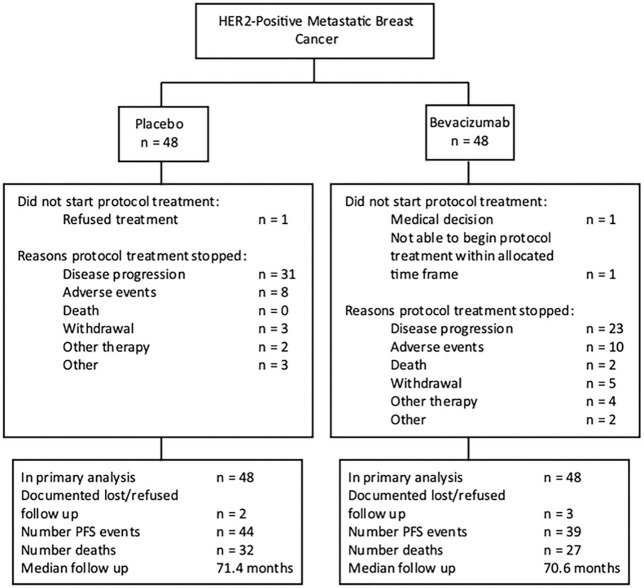 Figure 1
Figure 1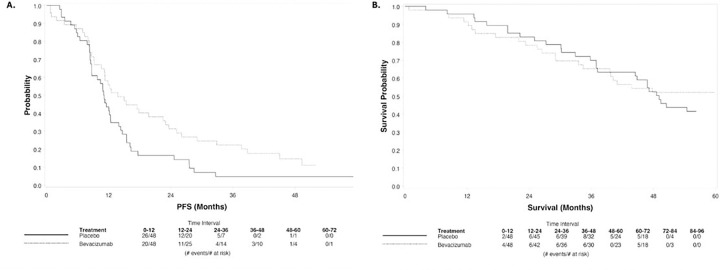 Figure 2
Figure 2- —ECOG-ACRIN Cancer Research Group
- —National Cancer Institute of the National Institutes of Health
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHER2/EGFR in Cancer Research · Cancer Treatment and Pharmacology · Breast Cancer Treatment Studies
Introduction
In 2008, bevacizumab received accelerated Food and Drug Administration (FDA) approval for use in human epidermal growth factor receptor 2 (HER2)-negative metastatic breast cancer (MBC). This was based off the E2100 study, which showed a combination of paclitaxel plus bevacizumab significantly prolonged progression-free survival (PFS) in treatment-naïve patients with MBC (1). By 2011, however, the FDA withdrew its approval for bevacizumab due to the lack of evidence of OS benefit and concern for unacceptable toxicity (2).
During this time period, the interest in the use of bevacizumab in HER2-positive breast cancer was also high due to studies demonstrating association between HER2 amplification and increased vascular endothelial growth factor (VEGF) in breast cancer (3–5). Additionally, a phase II trial at the time showed combining bevacizumab with trastuzumab in the treatment of HER2-positive MBC was both clinically feasible and active in the absence of chemotherapy (6). Based on the preclinical and preliminary clinical activity of the trastuzumab and bevacizumab combination, E1105 was developed to determine if the addition of bevacizumab to first-line chemotherapy and trastuzumab would improve PFS in patients with HER2-positive MBC.
Materials and Methods
Participants
Patients ≥ 18 years with histologically confirmed HER2-positive MBC, ECOG performance status of 0 or 1, adequate hematological, neurological, cardiac and end-organ function, and no prior systemic therapies were considered for enrollment (7). Prior taxane and trastuzumab were allowed if given > 12 months prior to recurrence. The study was coordinated by the ECOG-ACRIN Cancer Research Group (ECOG-ACRIN), in collaboration with Radiation Therapy Oncology Group (RTOG), North Central Cancer Treatment Group (NCCTG), Cancer and Leukemia Group B (CALGB), Southwest Oncology Group (SWOG), National Surgical Adjuvant Breast and Bowel Project (NSABP), Cancer Trials Support Unit (CTSU). Written informed consent was obtained from all patients before enrolment.
Treatment
Patients were randomized to receive standard first-line induction chemotherapy (paclitaxel 90 mg/m2 IV weekly x3 every 4 weeks [6 cycles] or paclitaxel 80 mg/m2 IV weekly x3 every 4 weeks + carboplatin AUC 2 IV weekly x3 every 4 weeks [6 cycles]) with trastuzumab (2 mg/kg IV weekly [after initial loading dose of 4 mg/kg] for 6 cycles) and placebo (PLAC) or bevacizumab (BEV) (10mg/kg IV every 2 weeks for 24 weeks [6 cycles]), followed by maintenance trastuzumab (6 mg/kg IV every 3 weeks) and BEV or PLAC (15 mg/kg IV every 3 weeks) until disease progression, severe adverse event, pregnancy, withdrawal, or death. Participants were allowed to discontinue chemotherapy and proceed to maintenance therapy. If trastuzumab or bevacizumab was discontinued, chemotherapy could continue. A schematic of the trial is provided in Fig. 1.
Assessments
Tumor (Computer tomography/ bone scan) and cardiac (echocardiogram or MUGA) assessments were performed at baseline, every 3 months, and 3 months post treatment. Tumor assessments continued until first progression. Complete blood counts were assessed prior to every cycle. Quality of life (QOL) assessments (FACIT-Fatigue Subscale, FACT/NCCN Breast Symptom Index, FACT/GOG-Ntx, FACT-G item GP5) were completed at baseline, end of cycles 3 and 6 induction, cycle 5 maintenance, 12 months post-randomization, and annually to 60 months post-randomization.
Statistical Considerations and Endpoints
Progression-free survival (PFS) was the primary endpoint and was defined as time from randomization to first disease progression via RECIST 1.0, new second breast primaries, or to death from any cause. Blinded treatment assignments were made in permuted blocks in a 1:1 fashion to PLAC or BEV. Randomization was stratified by prior adjuvant trastuzumab use, prior taxane use, disease-free interval (≤ 24 months, > 24 months), and planned carboplatin (yes, no). The accrual goal was 416 patients where 301 PFS events provided 86% power to detect a 30% reduction in the failure hazard rate. The trial was monitored by the ECOG-ACRIN DSMC, including a prespecified cardiac stopping rule for high rates of clinical CHF in BEV.
Secondary endpoints included overall survival (OS), defined as time from randomization date to death from any cause. The Kaplan-Meier method was used to estimate time-to-event distributions. Cox proportional hazards models were used to estimate hazard ratios and test for significance. Toxicities were graded according to CTCAE version 3.0. Cardiac safety profiles included clinical congestive heart failure (symptomatic decline in LVEF to below the lower limit of normal or symptomatic diastolic dysfunction). Baseline characteristics are reported among 95 of 96 with baseline information available, specific treatment information is reported among 93 of 96 patients who began protocol therapy, and best response, PFS and OS are analyzed on an intent-to-treat basis.
Results
Baseline Characteristics
Between November 9, 2007, and October 28, 2009, 96 of 416 patients were enrolled. Due to slow accrual, the trial was closed after October 2009. Table 1 provides a summary of baseline characteristics.
Among the patients who began treatment in the PLAC (n = 47) and BEV (n = 46) arms, 64% (30/47) and 57% (26/46) began the optional carboplatin, and 72% (34/47) and 76% (35/46) completed 6 cycles of induction therapy, respectively. The median number of cycles for maintenance therapy (n = 63) was 8 and 16 for the PLAC and BEV arms. Disease progression (66% [31/47] and 50% [23/46]) and adverse events (15% [7/47] PLAC and 22% [10/46] BEV) were the most common reasons for discontinuing treatment.
Clinical Efficacy and Secondary Endpoints
The best overall response rate (CR + PR) was 54% (26/48) and 61% (29/48) in PLAC and BEV, respectively (Table 2). There was no statistically significant difference in PFS: median PFS was 11.1 and 13.8 months; hazard ratio (HR) (95% Confidence Interval [Cl]) for BEV vs. PLAC: 0.73 (0.43–1.23), p = 0.24 (Fig. 2A). With n = 96 patients and 83 PFS events, the power to detect the original target difference between arms was only 37%. At a median follow-up of 70.7 months, median overall survival was 49.1 and 63 months; (HR [95% Cl]: 1.09 [0.61–1.97], p = 0.75) (Fig. 2B (truncated at 60 months)).
Overall Toxicity and Cardiac Safety
Toxicity incidence, defined as ≥ grade 3 and experienced by ≥ 2 patients, occurred in 47% (22/47) of PLAC and 67% (30/45) of BEV patients (Table 3). The most frequent ≥ grade 3 toxicities across both arms were neutropenia (6.4%, 6.7%) and hypertension (10.6%, 13.3%). Left ventricular systolic dysfunction (0%, 8.9%), fatigue (2.1%, 11.1%), and sensory neuropathy (6.4%, 11.1%) occurred more frequently in the BEV arm. At Cycle 6 Induction, more BEV patients reported fatigue compared to PLAC (FACIT Fatigue Scale: mean scores: 30.2 and 37.0, p = 0.02; FACT-G item GP5 [“I am bothered by sided effects of treatment”]: mean scores: 2.5 and 3.2, p < 0.01). One patient treated with bevacizumab died from treatment-related catheter infection (Table 3). Clinical congestive heart failure occurred in 1 PLAC and 4 BEV patients.
Discussion
During the enrollment of the presented study, new drug approvals such as lapatinib (10), decreased metastatic recurrence with trastuzumab, and excitement regarding other HER2 targeted agents (such as pertuzumab and trastuzumab-emtansine) resulted in low patient accrual and early study closure in 2009. Due to low accrual, the study was underpowered, and no significant difference in clinical outcomes was observed between treatment arms. The safety profiles for bevacizumab and trastuzumab were consistent with prior phase I, II and III trials. Cardiac toxicity is a known side effect of trastuzumab; however, previous studies found the toxicity was reversible, unlike doxorubicin-induced cardiomyopathy (11, 12). We saw few overall cardiac adverse events from bevacizumab in addition to the hallmark hypertension associated with anti-angiogenic drugs (13).The results from this trial corroborated the 2011 FDA decision to remove bevacizumab as a recommended therapeutic option for patients with breast cancer.
Since the closure of E1105, other clinical trials have explored the combination of HER2-targeted and antiangiogenic therapies. A phase II single-arm trial of bevacizumab, trastuzumab, and capecitabine showed clinical activity as first-line therapy for patients with HER2-positive MBC, with no unexpected toxicities, and a median time to progression of 14.5 months (95% Cl, 10.5 months to NR) (14). The AVEREL study randomized 424 first-line patients to trastuzumab/docetaxel with or without concomitant bevacizumab (15). Despite a trend favoring bevacizumab PFS (median 13.7 vs. 16.5 months; HR 0.82, log-rank P = 0.078), no difference was observed in overall survival (15). The BETH study randomized 3509 patients with HER2-positive early stage breast cancer to receive standard chemotherapy/trastuzumab with or without bevacizumab for 1 year of adjuvant therapy (16). After 38 months of follow-up, there was no statistically significant difference between treatment arms (92% IDFS rates in both groups). Currently, the majority of recent studies using bevacizumab to treat breast cancer are in the HER2-negative patient population or are in subsets of HER2-positive and -negative patients with specific types of refractory disease (17, 18).
More recently, the major focus on treating refractory HER2-positive MBC lies in developing new HER2-targeted antibody-drug conjugates, combinations of CDK4/6 or PI3K/Akt inhibitors with these agents as well as with endocrine therapies, and combinations of different immunotherapy agents with HER2-targeted therapies (19). Despite the strong pre-clinical rationale for combining HER2-targeted therapies with antiangiogenic drugs, there was no overall benefit, and there was added toxicity of combining bevacizumab with trastuzumab and chemotherapy, aligning with the 2011 FDA decision to remove the recommendation for the use of bevacizumab in all breast cancers. Despite advances in the adjuvant and metastatic setting made over the past decades, approximately 15–20% of patients with early HER2-positive breast cancer still relapse after curative therapy, and HER2-positive MBC remains incurable. Therefore, new therapeutic approaches are still necessary for this disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Miller K, Wang M, Gralow J, Dickler M, Cobleigh M, Perez EA (2007) Paclitaxel plus Bevacizumab versus Paclitaxel Alone for Metastatic Breast Cancer. N Engl J Med 357(26):2666–267618160686 10.1056/NEJ Moa 072113 · doi ↗ · pubmed ↗
- 2Rossari JR, Metzger-Filho O, Paesmans M, Saini KS, Gennari A, de Azambuja E (2012) Bevacizumab and Breast Cancer: A Meta-Analysis of First-Line Phase III Studies and a Critical Reappraisal of Available Evidence. J Oncol 2012:41767323008712 10.1155/2012/417673 PMC 3447373 · doi ↗ · pubmed ↗
- 3Linderholm B, Andersson J, Lindh B, Beckman L, Erlanson M, Edin K (2004) Overexpression of c-erb B-2 is related to a higher expression of vascular endothelial growth factor (VEGF) and constitutes an independent prognostic factor in primary node-positive breast cancer after adjuvant systemic treatment. Eur J Cancer 40(1):33–4214687787 10.1016/s 0959-8049(03)00673-7 · doi ↗ · pubmed ↗
- 4Petit AM, Rak J, Hung MC, Rockwell P, Goldstein N, Fendly B (1997) Neutralizing antibodies against epidermal growth factor and Erb B-2/neu receptor tyrosine kinases down-regulate vascular endothelial growth factor production by tumor cells in vitro and in vivo: angiogenic implications for signal transduction therapy of solid tumors. Am J Pathol 151(6):1523–15309403702 PMC 1858348 · pubmed ↗
- 5Yang W, Klos K, Yang Y, Smith TL, Shi D, Yu D (2002) Erb B 2 overexpression correlates with increased expression of vascular endothelial growth factors A, C, and D in human breast carcinoma. Cancer 94(11):2855–286112115372 10.1002/cncr.10553 · doi ↗ · pubmed ↗
- 6Hurvitz S, Pegram M, Lin L, Chan D, Allen H, Dichmann R (2009) Final Results of a Phase II Trial Evaluating Trastuzumab and Bevacizumab as First Line Treatment of HER 2-Amplified Advanced Breast Cancer. Cancer Res 69(24Supplement):6094
- 7Wolff AC, Hammond MEH, Hicks DG, Dowsett M, Mc Shane LM, Allison KH (2013) Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J Clin Oncol [Internet]. Oct 7 [cited 2023 Jul 25]; 10.1200/JCO.2013.50.9984?role=tab · doi ↗
- 8O’Brien PC, Fleming TR (1979) A multiple testing procedure for clinical trials. Biometrics 35(3):549–556497341 · pubmed ↗