Parinaud Syndrome in a Patient With Microangiopathic Lesions in the Bilateral Gangliocapsular Region and Left Thalamus
Renu Magdum, Priyanka S Aher

TL;DR
A 62-year-old man with vision and walking issues was found to have Parinaud syndrome caused by brain lesions linked to high blood pressure.
Contribution
This case highlights microangiopathy as a novel cause of Parinaud syndrome beyond typical midbrain involvement.
Findings
MRI showed lesions in the thalamic and gangliocapsular regions, not the typical midbrain.
Symptoms aligned with Parinaud syndrome despite atypical lesion location.
Hypertension was likely the underlying cause of the microangiopathy.
Abstract
Parinaud syndrome, which most commonly involves the dorsal midbrain, has classical features of upward gaze paralysis, convergence-retraction nystagmus, and pupillary light near dissociation. A 62-year-old male presented to the Eye department with diminution of vision and symptoms of dry eye with associated difficulty in walking. Examination revealed nystagmus while performing convergence test. An MRI revealed lesions in the thalamic and gangliocapsular regions. Microangiopathies involving the thalamus and gangliocapsular region can lead to Parinaud syndrome. In our case, microangiopathies were most probably hypertensive.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1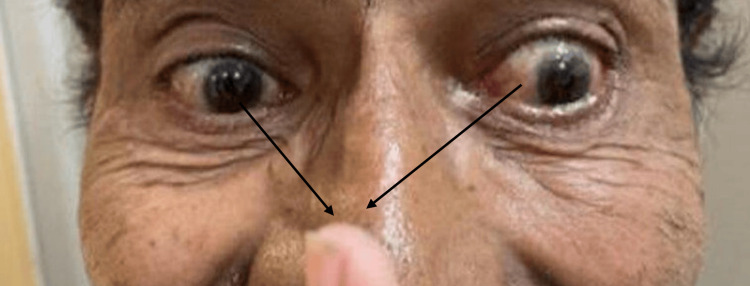 Figure 2
Figure 2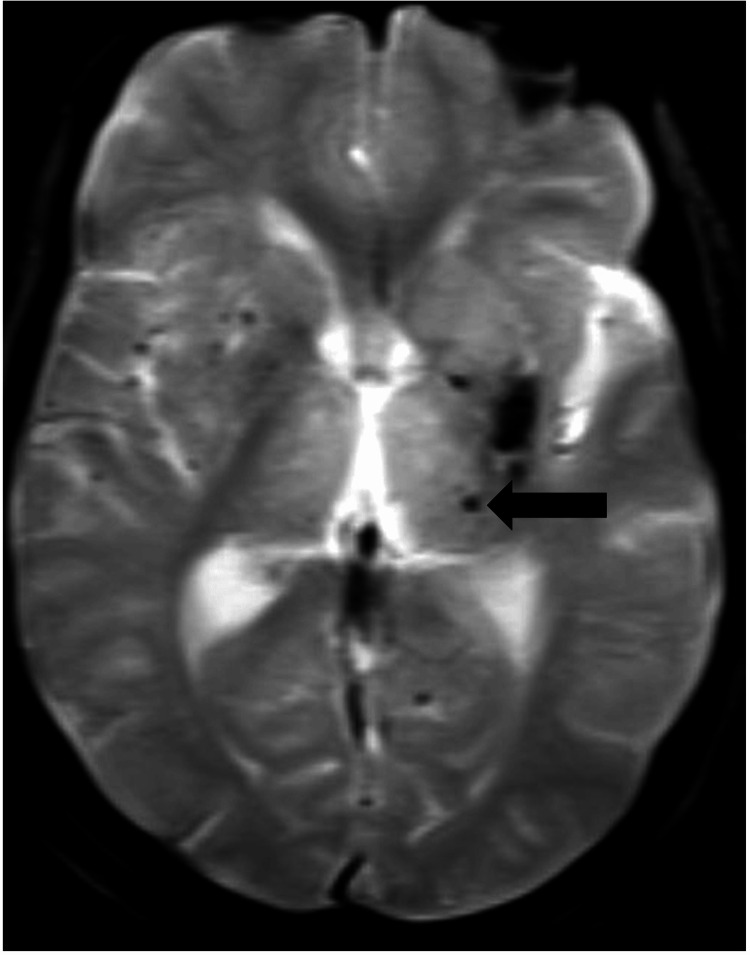 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVestibular and auditory disorders · Ophthalmology and Eye Disorders · Glaucoma and retinal disorders