Risk of Chronic Obstructive Pulmonary Disease and Receipt of a Breathing Test in 26 States and the District of Columbia, 2017–2018
Kathleen B. Watson, Janet B. Croft, Anne G. Wheaton, Yong Liu, Antonello Punturieri, Lisa Postow, Susan A. Carlson, Kurt J. Greenlund

TL;DR
This study found that many adults without COPD show symptoms indicating higher COPD risk, but only about 40% of them had a breathing test.
Contribution
The study provides new insights into COPD risk levels and testing rates among adults in 26 U.S. states and the District of Columbia.
Findings
Over 15% of adults without COPD were at higher COPD risk based on symptoms, age, and smoking.
More than 40% of high-risk adults reported receiving a breathing test.
Common COPD symptoms like cough and shortness of breath were reported by over 10% of adults.
Abstract
We estimated the prevalence of respiratory symptoms, chronic obstructive pulmonary disease (COPD) risk level, and receipt of a breathing test among adults without reported COPD in 26 states and the District of Columbia by using 2017–2018 Behavioral Risk Factor Surveillance System data. Among adults without reported COPD, the 3 respiratory symptoms indicating COPD (chronic cough, phlegm or mucus production, shortness of breath) were common (each >10%). About 15.0% were at higher COPD risk (based on the number of symptoms, age, and smoking status); 41.4% of adults at higher risk reported receipt of a breathing test. Patient–provider recognition and communication of risk symptoms, appropriate screening, and follow-up are important for early diagnosis and treatment.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure
Figure| Characteristic | Prevalence of a reported COPD diagnosis | Prevalence of respiratory symptoms among adults without a reported COPD diagnosis | ||
|---|---|---|---|---|
| Chronic cough | Sputum production | Shortness of breath | ||
|
| ||||
| Crude | 7.4 (7.2–7.7) | 13.7 (13.2–14.1) | 12.1 (11.7–12.5) | 19.0 (18.5–19.5) |
| Age-adjusted | 6.5 (6.3–6.8) | 13.4 (13.0–13.9) | 12.0 (11.6–12.5) | 18.3 (17.8–18.8) |
|
| ||||
|
| ||||
| Male | 5.9 (5.6–6.3) | 13.2 (12.6–13.9) | 13.1 (12.5–13.8) | 14.8 (14.1–15.5) |
| Female | 7.1 (6.7–7.5) | 13.6 (12.9–14.2) | 11.1 (10.5–11.7) | 21.7 (20.9–22.5) |
|
| ||||
| 18–39 | 2.9 (2.6–3.3) | 12.2 (11.4–13.0) | 11.9 (11.2–12.7) | 14.4 (13.6–15.3) |
| ≥40 | 10.0 (9.6–10.3) | 14.5 (14.0–15.1) | 12.3 (11.8–12.7) | 21.8 (21.2–22.4) |
|
| ||||
| Hispanic | 4.7 (3.8–5.8) | 13.3 (11.6–15.1) | 11.7 (10.2–13.5) | 18.9 (17.0–20.9) |
| Non-Hispanic Black | 6.8 (6.0–7.7) | 16.0 (14.8–17.4) | 14.4 (13.2–15.7) | 24.5 (23.1–26.1) |
| Non-Hispanic White | 6.9 (6.6–7.2) | 13.2 (12.7–13.7) | 12.2 (11.7–12.7) | 17.6 (17.0–18.2) |
| Non-Hispanic Other | 5.6 (4.8–6.7) | 13.5 (10.9–16.6) | 10.0 (8.3–11.9) | 14.6 (12.2–17.4) |
|
| ||||
| High school or less | 8.8 (8.3–9.3) | 16.2 (15.5–17.0) | 15.1 (14.3–15.9) | 22.7 (21.9–23.6) |
| Some college | 6.5 (6.0–6.9) | 13.8 (12.9–14.8) | 12.4 (11.6–13.2) | 19.1 (18.1–20.2) |
| College graduate | 3.2 (2.9–3.6) | 8.9 (8.4–9.5) | 7.4 (6.8–7.9) | 10.9 (10.4–11.5) |
|
| ||||
| Large central metro | 5.0 (4.5–5.5) | 12.4 (11.5–13.4) | 10.4 (9.5–11.4) | 17.0 (15.9–18.1) |
| Large fringe metro | 5.7 (5.2–6.3) | 12.9 (11.9–13.9) | 12.4 (11.4–13.4) | 17.3 (16.2–18.3) |
| Medium metro | 7.4 (6.8–8.1) | 13.5 (12.6–14.4) | 12.0 (11.3–12.8) | 18.5 (17.5–19.6) |
| Small metro | 7.8 (7.2–8.4) | 14.8 (13.4–16.4) | 13.2 (12.1–14.4) | 20.2 (18.7–21.8) |
| Micropolitan | 8.0 (7.5–8.7) | 14.6 (13.6–15.6) | 13.5 (12.6–14.5) | 20.1 (19.2–21.1) |
| Rural (noncore) | 8.4 (7.7–9.2) | 15.7 (13.9–17.8) | 15.0 (13.2–17.1) | 20.9 (19.8–22.2) |
|
| ||||
|
| ||||
| Former or current smoker | 11.2 (10.7–11.7) | 17.8 (17.0–18.6) | 17.1 (16.3–17.9) | 24.2 (23.3–25.2) |
| Never smoked | 3.1 (2.8–3.4) | 10.9 (10.3–11.5) | 9.0 (8.5–9.5) | 14.9 (14.3–15.5) |
|
| ||||
| Current asthma | 24.6 (23.2–26.1) | 25.3 (23.1–27.6) | 23.2 (21.0–25.6) | 46.9 (44.3–49.5) |
| Former history only | 11.8 (9.6–14.3) | 14.9 (13.0–16.9) | 15.2 (13.2–17.5) | 21.1 (19.0–23.5) |
| Never | 4.3 (4.1–4.5) | 12.3 (11.8–12.8) | 10.9 (10.4–11.3) | 15.7 (15.2–16.2) |
|
| ||||
| No | 2.3 (2.1–2.6) | 11.3 (10.8–11.8) | 10.0 (9.5–10.5) | 14.1 (13.6–14.6) |
| Yes | 15.7 (15.0–16.5) | 19.6 (18.5–20.7) | 18.3 (17.2–19.4) | 30.9 (29.6–32.2) |
| Subgroup | Combined no. of risk factors and symptoms | |||||
|---|---|---|---|---|---|---|
| Not at higher COPD risk (n = 115,344) | At higher COPD risk (n = 27,514) | |||||
| 0 | 1 | 2 | 3 | 4 | 5 | |
|
| ||||||
| Crude | 20.0 (19.5–20.6) | 37.6 (37.0–38.3) | 26.0 (25.5–26.5) | 10.7 (10.3–11.1) | 4.2 (4.0–4.4) | 1.5 (1.3–1.6) |
| Age-adjusted | 23.3 (22.7–23.8) | 37.5 (36.8–38.1) | 24.2 (23.7–24.7) | 9.8 (9.5–10.2) | 3.9 (3.7–4.1) | 1.3 (1.2–1.4) |
|
| ||||||
| Aged <40 y, never smoker | 78.3 (77.1–79.5) | 14.7 (13.7–15.8) | 5.3 (4.7–6.0) | 1.7 (1.4–2.1) | — | — |
| Aged ≥40 y, never smoker | — | 73.0 (72.0–73.9) | 17.8 (17.1–18.5) | 7.0 (6.4–7.7) | 2.2 (2.0–2.5) | — |
| Aged <40 y, current or former smoker | — | 64.2 (62.2–66.1) | 20.7 (19.1–22.5) | 10.0 (8.9–11.3) | 5.0 (4.1–6.0) | — |
| Aged ≥40 y, current or former smoker | — | —d | 59.3 (58.2–60.3) | 24.6 (23.7–25.6) | 10.5 (9.9–11.2) | 5.5 (5.1–6.0) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Obstructive Pulmonary Disease (COPD) Research · Respiratory Support and Mechanisms · Injury Epidemiology and Prevention
Objective
Chronic obstructive pulmonary disease (COPD) is a group of progressive airflow obstruction conditions with limited reversibility. In 2021, 14.2 million US adults reported physician-diagnosed COPD (1); many more adults with lung obstruction are unaware they have COPD (2). Adults at higher risk may not be aware of relevant risk factors and may not recognize symptoms as possibly related to COPD (3). When left untreated, COPD can advance faster to more severe stages of the disease (4); thus, early identification of COPD can improve health and reduce disability and death. Although screening asymptomatic adults is not recommended (5), the Global Initiative for Chronic Obstructive Lung Disease (GOLD) suggests adults with risk factors or symptoms (at higher COPD risk) be directed to subsequent testing for airflow obstruction (6). Estimates of adults at higher COPD risk who received a breathing test (spirometry) are limited. We examined COPD prevalence and, among adults without reported COPD, the prevalence of respiratory symptoms, COPD risk factors, and receipt of breathing test stratified by COPD risk group.
Methods
We used data from the 2017–2018 Behavioral Risk Factor Surveillance System (BRFSS) (7). Twenty-six states and the District of Columbia administered an optional respiratory health module with questions about 3 respiratory symptoms (chronic cough, phlegm or mucus production, shortness of breath) and receipt of a breathing test. Combined landline and cellular telephone response rates ranged from 35.1% to 64.1% (median, 46.5%). The age-adjusted prevalence of COPD was estimated overall and by subgroup. Among adults without reported COPD, we estimated the age-adjusted prevalence of reported symptoms; the combined number of risk factors and symptoms; the risk for COPD (at higher risk vs not at higher risk); and receipt of a breathing test overall and by subgroup. The 2 risk factors considered were being aged 40 years or older and being a former or current smoker. We determined risk status by using GOLD’s “Could It Be COPD?” questionnaire (8), which asks about the number of risk factors and COPD-related symptoms. We defined higher COPD risk as having 3 or more symptoms or risk factors (combined). We used t tests to assess pairwise differences in the prevalence of COPD and COPD risk group by selected characteristics. Prevalence ratios (PRs), estimated from age-adjusted multiple logistic regression models, described the association between risk groups and receiving a breathing test. We used SAS-callable SUDAAN version 11.0.1 (RTI International) to conduct all analyses.
Results
Information on COPD diagnosis, respiratory symptoms, and receipt of breathing test was reported by 158,741 (82.8%) respondents in 26 states and the District of Columbia. COPD prevalence was highest among women, adults aged 40 years or older, former or current smokers, and adults with current asthma (Table 1). COPD prevalence was higher among non-Hispanic Black and non-Hispanic White adults than among Hispanic adults and increased with decreasing levels of education and urbanicity (Table 1).
Among adults without reported COPD, 13.4% (age-adjusted) reported chronic cough, 12.0% reported sputum production, and 18.3% reported shortness of breath (Table 1). Prevalence of reporting each symptom was highest among adults who were aged 40 years or older, were non-Hispanic Black, had a high school diploma or less, were living in rural areas, were former or current smokers, and had current asthma. Among adults without reported COPD, the prevalence of each symptom was higher among those reporting a breathing test (from 18.3% [sputum production] to 30.9% [chronic cough]) than among those reporting no breathing test (from 10.0% [sputum production] to 14.1% [chronic cough]) (Table 1). The prevalence of having a breathing test was higher among adults with COPD (68.1%; 95% CI, 65.0%–71.1%) than without (24.3%; 95% CI 23.8%–24.9%).
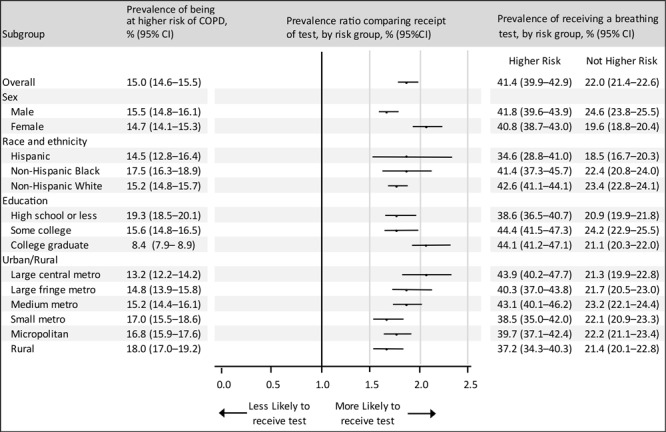
Among adults without reported COPD, 23.3% (age-adjusted) reported no symptoms or risk factors, 61.7% reported 1 or 2 symptoms or risk factors, and 15.0% reported 3 or more symptoms and risk factors (at higher COPD risk) (Table 2). Among adults at higher COPD risk, 41.4% reported receiving a breathing test. Overall, adults at higher COPD risk were nearly twice as likely (PR = 1.9; 95% CI,1.8–2.0) to report receiving a test compared with adults not at higher COPD risk (Figure). Women at higher COPD risk (PR = 2.1; 95% CI, 1.9–2.2) were more likely than men at higher COPD risk (PR = 1.7; 95% CI, 1.6–1.8) to report receiving a test; we observed no other subgroup differences.
Prevalence of adults at higher COPD risk and prevalence ratios of receipt of a breathing test, by risk status, among adults without a reported COPD diagnosis, by subgroup, Behavioral Risk Factor Surveillance System, 26 states and the District of Columbia, 2017–2018. Estimates were adjusted for age with the inclusion of age group as a covariate in the logistic model (unweighted n = 142,858; 813 responses excluded due to missing data on smoking status); prevalence ratios compare the age-adjusted prevalence of receipt of a breathing test among adults at higher COPD risk versus adults not at higher risk. Higher COPD risk was defined as 3 or more symptoms or risk factors from the GOLD’s “Could It Be COPD?” questionnaire (8). Error bars indicate 95% CIs. “Other” non-Hispanic not included due to heterogeneity of this group. Abbreviations: COPD, chronic obstructive pulmonary disease; GOLD, Global Initiative for Chronic Obstructive Lung Disease.
Discussion
Among adults without reported COPD, shortness of breath was the most reported symptom (19.0%), followed by chronic cough (13.7%) and sputum production (12.1%). Based on respiratory symptoms, age, and smoking status, 15.0% of adults were at higher COPD risk. Adults at higher COPD risk were twice as likely as adults not at higher COPD risk to report receiving a breathing test, although only 4 in 10 adults at higher COPD risk reported receiving a breathing test.
Studies have consistently shown that COPD symptoms are present in the US population, although prevalence estimates have varied across studies, likely because of differences in study populations and symptom measures (9–11). Reported estimates for wheezing, shortness of breath, and coughing were between 10% and 20% and were dependent on the sample and measure used (9–11). Studies estimating the prevalence of adults at higher COPD risk and how this prevalence is associated with receiving a breathing test are sparser. One study found that 5.1% of adults were at higher COPD risk (12), but their definition of risk differed from ours: their study did not include adults who had symptoms but no smoking history (an estimated 10.9% in our study). Another study reported a similar prevalence for receiving a breathing test (26%), regardless of symptoms or diagnosis (9). Although we found no studies reporting the relationship between risk status and receipt of breathing tests, findings consistently show respiratory symptoms to be present in adults with and without diagnosed COPD.
Early COPD diagnosis leads to treatment and better quality of life. To increase rates of early diagnosis of COPD, it may be important to improve COPD screening through the use of COPD case-finding tools (6). Our study demonstrated that more than half of adults at higher COPD risk had not received a breathing test, a case-finding tool, and may benefit from discussing respiratory symptoms with their health care providers. Improving understanding about the reasons symptomatic adults may be potentially undiagnosed and untreated, such as the cost of testing or incomplete reporting of symptoms by patients (9), can help guide prevention, early diagnosis, treatment, and management strategies (13). Breathing tests are important in diagnosis and guiding treatment decisions for another reason. Respiratory symptoms are common in former and current smokers without airway obstruction (14), yet this group may not respond to COPD therapeutics (15).
This study has limitations. The self-reported data might be subject to recall and social desirability biases. Data included noninstitutionalized adults in 26 states and the District of Columbia; therefore, findings may not be generalizable to the broader US population. Because of differences in the time frame referenced for the symptom-related questions (eg, past 3 months) and the question for receipt of a breathing test (ever), symptoms may or may not have existed before receipt of the breathing test. The presence of respiratory symptoms and risk factors in the absence of diagnosed COPD cannot be interpreted as undiagnosed COPD (11). Finally, when examining the association between COPD risk and receipt of a breathing test, this study did not account for the presence of other respiratory conditions that might warrant a breathing test. For example, 63.6% of adults with and 18.6% without a history of asthma reported a breathing test.
COPD accounts for most deaths from chronic lower respiratory diseases, a leading cause of US deaths (16). Strategies to improve patient awareness and patient–provider communications and to promote the use of breathing tests among patients who are at higher risk for COPD are needed to support the early screening, diagnosis, and management of COPD and its symptoms.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu Y , Carlson SA , Watson KB , Xu F , Greenlund KJ . Trends in the prevalence of chronic obstructive pulmonary disease among adults aged ≥18 years — United States, 2011–2021. MMWR Morb Mortal Wkly Rep. 2023;72(46):1250–1256. 10.15585/mmwr.mm 7246 a 1 37971940 PMC 10684355 · doi ↗ · pubmed ↗
- 2Martinez CH , Mannino DM , Jaimes FA , Curtis JL , Han MK , Hansel NN , . Undiagnosed obstructive lung disease in the United States. Associated factors and long-term mortality. Ann Am Thorac Soc. 2015;12(12):1788–1795. 10.1513/Annals ATS.201506-388OC 26524488 PMC 4722830 · doi ↗ · pubmed ↗
- 3Calverley PM , Nordyke RJ , Halbert RJ , Isonaka S , Nonikov D . Development of a population-based screening questionnaire for COPD. COPD. 2005;2(2):225–232. 10.1081/COPD-57594 17136949 · doi ↗ · pubmed ↗
- 4Welte T , Vogelmeier C , Papi A . COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. 10.1111/ijcp.12522 25363328 · doi ↗ · pubmed ↗
- 5Mangione CM , Barry MJ , Nicholson WK , Cabana M , Caughey AB , Chelmow D , ; US Preventive Services Task Force. Screening for chronic obstructive pulmonary disease: US Preventive Services Task Force reaffirmation recommendation statement. JAMA. 2022;327(18):1806–1811. 10.1001/jama.2022.5692 35536260 · doi ↗ · pubmed ↗
- 6Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease: 2023 Report. 2023. Accessed January 15, 2024. https://goldcopd.org/2023-gold-report-2
- 7Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System. Survey data & documentation. Last reviewed August 30, 2023. Accessed January 15, 2024. https://www.cdc.gov/brfss/data_documentation/index.htm
- 8Global Initiative for Chronic Obstructive Lung Disease. Patients and advocacy groups. Accessed January 15, 2024. https://goldcopd.org/patients-advocacy-groups