Leclercia adecarboxylata in a Patient With Newly Diagnosed Chronic Lymphocytic Leukemia
Nivedha Balaji, Aarushi Kalra, Aleksandra Ignatowicz, Tanya Aggarwal, Sonu Gupta

TL;DR
This paper reports a case of Leclercia adecarboxylata infection in a man with leukemia, highlighting its misdiagnosis and low virulence.
Contribution
The novelty lies in documenting a rare clinical case of L. adecarboxylata bacteremia in an immunocompromised patient.
Findings
L. adecarboxylata was identified in a 53-year-old immunocompromised male with chronic lymphocytic leukemia.
The infection was successfully managed with antibiotics and did not result in severe complications.
The case emphasizes the importance of accurate identification to avoid misdiagnosis as Escherichia coli.
Abstract
Leclercia adecarboxylata is a Gram-negative bacillus commonly seen in immunocompromised individuals and often misdiagnosed as Escherichia coli. L. adecarboxylata is an opportunistic pathogen found in aquatic environments. It is a nonfatal infection that has low virulence and endorses susceptibility to many common antibiotics. We report a case of a 53-year-old immunocompromised male who was managed for L. adecarboxylata bacteremia.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
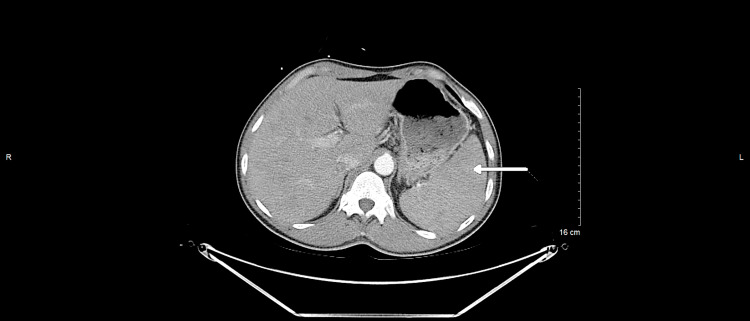 Figure 1
Figure 1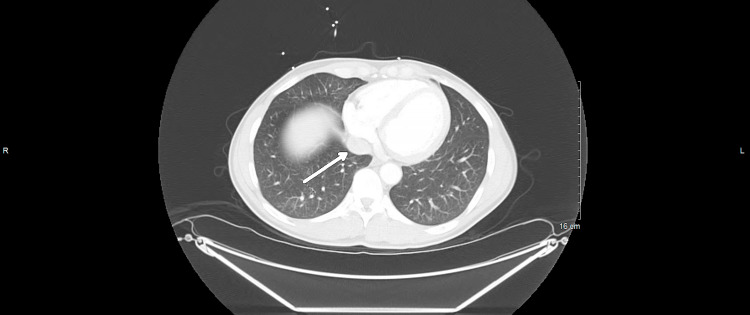 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEnterobacteriaceae and Cronobacter Research · Mycobacterium research and diagnosis · Antibiotic Resistance in Bacteria
Introduction
Leclercia adecarboxylata is a motile Gram-negative bacillus in the Enterobacteriaceae family known as an opportunistic aquatic organism. It most commonly presents as an acquired infection in the immunocompromised [1, 2]. Due to similar biochemical features, there have been times this microorganism has been misdiagnosed as Escherichia coli [3]. However, in the last few years, reported cases of L. adecarboxylata have increased in frequency, which may have come from recent outbreaks of product contamination [4]. Bacteremia of this microorganism has been seen in those patients who have skin tears such as burn wounds and cellulitis [5]. Per studies, this low-virulence bacterium has shown high susceptibilities to common antibiotics. In rare cases, sometimes its susceptibility has been limited to first-generation cephalosporin or Trimethoprim (TMP)-Sulfamethoxazole (SMX) due to the resistance of a few strains [6]. In this case report, we discuss the emergence of L. adecarboxylata bacteremia in a newly diagnosed immunocompromised patient.
Case presentation
Our case involves a 53-year-old male with no significant medical history who presented to the emergency department with a 5-day history of shortness of breath, malaise, chills, pleuritic chest pain, and productive cough with brown-colored sputum. He endorsed a 20-pound weight loss over a 3-month period and the presence of bilateral inguinal lymphadenopathy of 4-5 weeks duration. Vitals were significant for the temperature of 37.8°C. Laboratory studies were significant for white blood cell (WBC) 42.4 K/μL (5-10 K/μL) with predominant lymphocytosis and procalcitonin 0.40 μg/L (<0.1 μg/L). Physical examination was notable for an ill-appearing male with bilateral inguinal lymphadenopathy without tenderness to palpation. His cardiopulmonary and abdominal exams were unremarkable. Computed tomography (CT) scan of the chest, abdomen, and pelvis shown in Figures 1-2 revealed bilateral ground glass opacities, mediastinal, bilateral hilar, and bilateral axillary adenopathy with mild splenomegaly.
Computed tomography (CT) scan of the chest, abdomen, and pelvis depicting mild splenomegaly.White arrow shows the mild splenomegaly.
Computed tomography (CT) scan of the chest, abdomen, and pelvis depicting mediastinal lymphadenopathy.White arrow shows the mediastinal lymphadenopathy.
Blood cultures were obtained, and then the patient was started on ampicillin-sulbactam 3 g every 6 hours and azithromycin 500 mg every 24 hours for treatment of community-acquired pneumonia as the CT scan noted bilateral ground glass opacities. Blood cultures grew Enterobacter species L. adecarboxylata and Staphylococcus epidermidis. L. adecarboxylata was pan-sensitive. S. epidermidis was deemed a contamination rather than a true infection because it only grew in one bottle. Infectious diseases department was consulted who then initiated amoxicillin 875 mg every 12 hours for an additional 10 days after the patient had completed a 5-day course of ampicillin-sulbactam and azithromycin. With further investigation, the patient reported swimming in a nearby lake several days prior to admission. This is important as the lake may be the source of this patient's infection with L. adecarboxylata.
The patient underwent a malignancy workup during the hospitalization due to his presentation with enlarged lymph nodes, elevated WBC count, and due to being infected by L. adecarboxylata which is present commonly in the immunocompromised state. Hematology and Oncology were consulted after the leukemia and lymphoma panel was positive for chronic lymphocytic leukemia (CLL). The patient was then discharged and underwent excisional biopsy of the right inguinal lymph node confirming the diagnosis of CLL. Chemotherapy with acalabrutinib and obinutuzumab was initiated at that time. No further follow-up with infectious diseases was required after completion of antibiotic therapy.
Discussion
In this case presentation, we discuss how L. adecarboxylata was diagnosed in a patient who truly fits the risk factor profile for this infection. As mentioned previously, L. adecarboxylata is an opportunistic pathogen that is widely present in nature, existing in food, water, soil, and freshwater environments, and is commonly seen in polymicrobial infections [4]. It is also seen in the normal gut flora [2]. It is prevalent in people with predisposing risk factors such as wounds/ulcers, catheters, or immunosuppressive diseases such as cancer, renal failure, or cirrhosis [4, 7, 8]. The morphological and microbiological properties of L. adecarboxylata and the Escherichia genus are similar resulting in the misidentification of such infections [7, 8]. After further biochemical testing with DNA hybridization, Leclercia was differentiated from other species in the Enterobacteriaceae family [6].
After the patient stated he was near a body of water prior to hospital arrival and presented with symptoms, sepsis workup labs including respiratory, urine, and blood cultures were collected. His presentation of significant weight loss over the year along with developing lymphadenopathy was concerning for underlying malignancy which prompted further diagnostic testing. The setting where the patient had a biopsy completed during the hospital course showed CLL and blood cultures positive for L. adecarboxylata, which only provided further confirmation that this L. adecarboxylata was not a contaminant.
Sensitivities of Leclercia were sent and came back pan-sensitive. Many previous cases state that this microorganism is of low virulence [5]. Our patient was initially given cefepime and azithromycin which was transitioned to amoxicillin. A study by Stock et al., showed that 101 strains of Leclercia were naturally susceptible to 70 antimicrobial agents such as tetracyclines, aminoglycosides, most of the beta-lactams, fluoroquinolones, chloramphenicol, nitrofurantoin, and azithromycin; however, they were resistant to penicillin G, oxacillin, erythromycin, roxithromycin, clarithromycin, ketolides, lincosamides, streptogramins, linezolid, glycopeptides, rifampicin, fusidic acid, and fosfomycin [6].
This case portrays the emergence of L. adecarboxylata in immunocompromised patients which should not be overlooked. Delay in treatment of L. adecarboxylata can lead to complications such as endocarditis, bacteremia, and spontaneous bacterial peritonitis [4, 9]. It can also cause cutaneous diseases such as cellulitis [9, 10]. Early identification and management with antibiotics proves to improve morbidity and mortality.
Conclusions
In conclusion, this relatively new pathogen has not been studied enough to be considered as a differential on initial presentation for hospitalists, but its recent emergence in immunocompromised patients raises a concern for further evaluation and management. Though susceptible to most antibiotics currently, L. adecarboxylata’s resistance can grow over time and may need further studies to discuss worsening complications if management is not sufficient or delayed. This case highlights the need to keep a broad differential when treating patients who are immunocompromised.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Leclercia adecarboxylata as emerging pathogen in human infections: Clinical features and antimicrobial susceptibility testing Pathogens Zayet S Lang S Garnier P 13991020213483255510.3390/pathogens 10111399 PMC 8619052 · doi ↗ · pubmed ↗
- 2A rare case of multidrug-resistant Leclercia adecarboxylatacatheter-related bloodstream infection and an updated brief literature review Mediterr J Hematol Infect Dis Colangelo C Tiecco G Di Gregorio M 015202310.4084/MJHID.2023.052PMC 1049731137705522 · doi ↗ · pubmed ↗
- 3Leclercia adecarboxylata: a case report and literature review of 74 cases demonstrating its pathogenicity in immunocompromised patients Infect Dis Spiegelhauer MR Andersen PF Frandsen TH Nordestgaard RL Andersen LP 17918851201910.1080/23744235.2018.153683030488747 · doi ↗ · pubmed ↗
- 4Sepsis and Leclercia adecarboxylata QJM Matsuura H Sugiyama S 73373411120182991714510.1093/qjmed/hcy 131 · doi ↗ · pubmed ↗
- 5Leclercia adecarboxylata bacteremia without a focus in a non-immunosuppressed patient Am J Case Rep Shaikhain T Al-Husayni F Al-Fawaz S Alghamdi EM Al-Amri A Alfares M 022202110.12659/AJCR.929537 PMC 801983833782375 · doi ↗ · pubmed ↗
- 6Leclercia adecarboxylata isolation: Case reports and review J Clin Diagn Res Anuradha M 048201410.7860/JCDR/2014/9763.5260 PMC 431625725653951 · doi ↗ · pubmed ↗
- 7First clinical case of VIM-1-producing Leclercia adecarboxylata: A case report and literature review Med i Microecol Shuhoumi MAA Mhrooqi AA Rashdi AA Kumar R Jabri AA Al Kalbani A Al Jardani A 100075152023
- 8A case of Leclercia adecarboxylata endocarditis in a 62-year-old man ID Cases Malik K Davie R Withers A Faisal M Lawal F 024202110.1016/j.idcr.2021.e 01091 PMC 804745733889491 · doi ↗ · pubmed ↗