Successful Management of Atypical Hemolytic-Uremic Syndrome in Pregnancy Using Eculizumab: A Case Review
Faryal Altaf, Mikail Khanzada, Abeer Qasim, Anandu M Anto, Asim Haider, Misbahuddin Khaja

TL;DR
A 36-year-old pregnant woman with atypical hemolytic-uremic syndrome (aHUS) was successfully treated with eculizumab after complications from placental abruption.
Contribution
This case highlights the successful use of eculizumab in managing aHUS during pregnancy, offering insights into treatment strategies for this rare condition.
Findings
The patient showed marked clinical improvement after eculizumab treatment following a cesarean section.
Initial plasmapheresis was suboptimal, but eculizumab led to sustained remission without disease relapse.
Abstract
Hemolytic-uremic syndrome (HUS) is a rare thrombotic microangiopathy characterized by the triad of microangiopathic hemolytic anemia (MAHA), thrombocytopenia, and acute kidney injury. The disease is pathologically marked by fibrinoid necrosis within renal arterioles and glomerular capillaries. HUS can be categorized into typical variants, often linked to Shiga toxin-producing Escherichia coli (STEC) infection, and atypical variants that stem from dysregulation in the alternative complement pathway. Pregnancy is a recognized predisposing condition for HUS due to the potential reduction in complement regulatory proteins and the possibility of heightened maternal immune response. This report illustrates the case of a 36-year-old woman who, at 36 weeks of gestation, faced a breech presentation and was diagnosed with atypical HUS (aHUS) after placental abruption. Following a cesarean…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
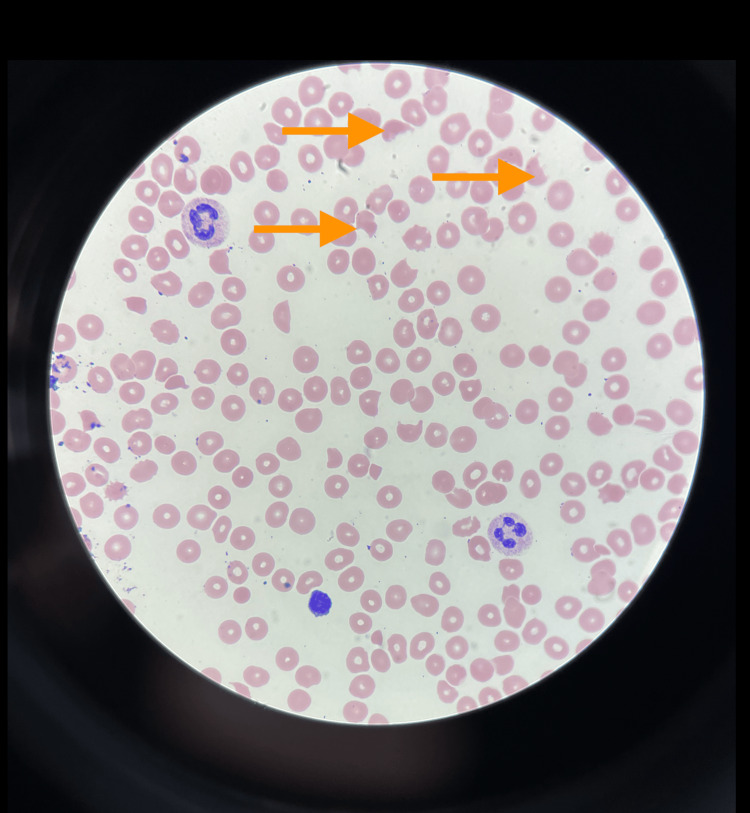 Figure 1
Figure 1 Figure 2
Figure 2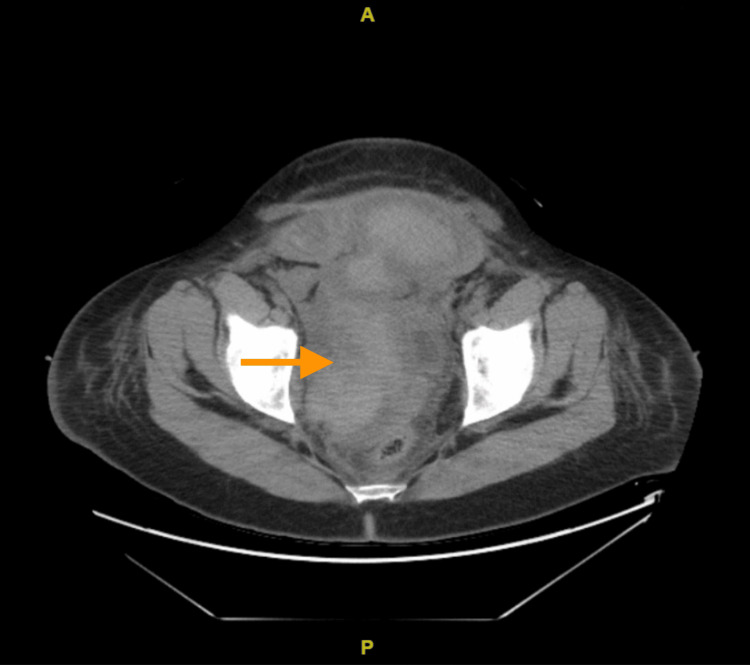 Figure 3
Figure 3 Figure 4
Figure 4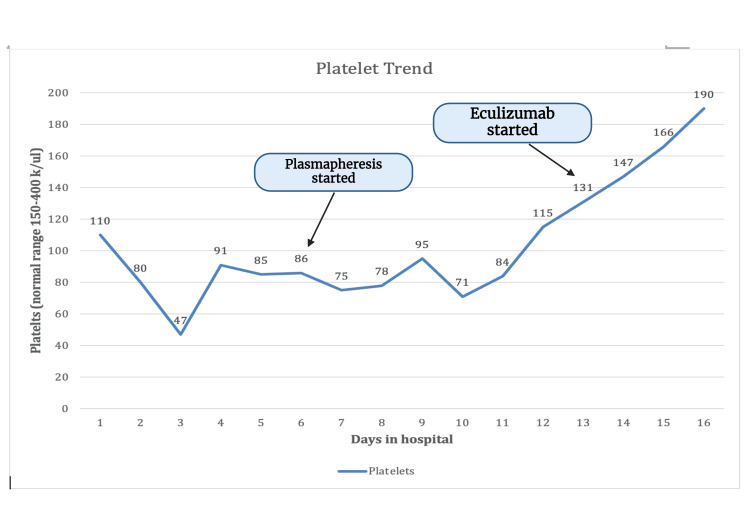 Figure 5
Figure 5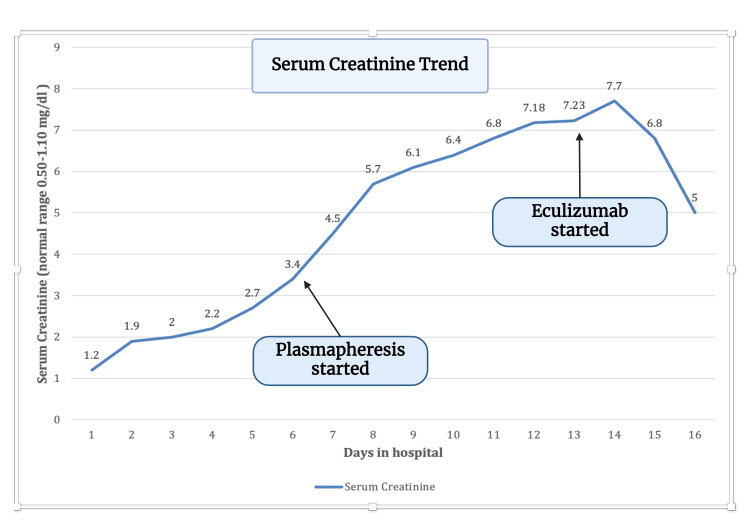 Figure 6
Figure 6| Laboratory test | Reference values | |
| Serum creatinine | 6.1 | 0.50-1.10 mg/dl |
| BUN | 78 | 8.0-26.0 mg/dl |
| Hemoglobin | 7.1 | 12-16 g/dl |
| White blood cell count | 8.9 | 4.8-10.8 k/ul |
| Platelet count | 84 | 150-400 k/ul |
| Prothrombin time | 14 | 9.9-13.3 seconds |
| INR | 1.19 | 0.85-1.14 |
| Total bilirubin | 1.6 | 0.2-1.2 mg/dl |
| APTT | 26 | 25.1-36.5 seconds |
| Coombs test | Negative | Negative |
| SRA | Negative | Negative |
| Direct bilirubin | 0.5 | 0.0-0.3 mg/dl |
| LDH | 2856 | 100-190 unit/l |
| Complement 3 | 147 | 90-150 mg/dl |
| Complement 4 | 30 | 16-47 mg/dl |
| G6PD | <10 | 30-200 mg/dl |
| ADAMTS13 | 81 | 68-163 |
| D-dimer | 10392 | 0-230 ng/ml |
| Fibrinogen | 237 | 185-450 mg/dl |
| HIV ½ antibody | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsComplement system in diseases · Renal Diseases and Glomerulopathies · Blood groups and transfusion
Introduction
Hemolytic-uremic syndrome (HUS) is a rare thrombotic microangiopathy characterized by microangiopathic hemolytic anemia (MAHA), thrombocytopenia, and acute kidney injury (AKI). Fibrinoid necrosis may also be seen in renal arterioles and glomerular capillaries [1]. HUS is classified into typical and atypical variants, commonly associated with Shiga toxin-producing Escherichia coli (STEC), and atypical variants due to alternate complement pathway dysregulation. Common triggers of atypical HUS (aHUS) include malignancy, autoimmune disease, infection, transplantation, and certain drugs [2]. Pregnancy is one such condition that may predispose an individual to HUS due to diminished complement regulator proteins being produced and the possibility of an exaggerated maternal response [3]. Most cases of pregnancy-induced HUS have occurred in individuals harboring mutations of membrane cofactor protein, factor H or factor I, all part of the alternate pathway.
While only affecting one in 25,000 pregnancies, HUS is mainly seen in the postpartum period and is associated with high rates of end-stage renal disease (ESRD), with up to 70% of ESRD patients requiring long-term dialysis [3,4]. Relapse of HUS has been seen in patients having undergone renal transplantation [4]. While plasma therapy has long been a mainstay of treatment, newer studies support the use of eculizumab, a monoclonal antibody that binds to and inhibits complement C5 [5]. Eculizumab has proven more effective in preventing long- and short-term renal outcomes and reducing relapse rates [6,7]. In this report, we detail the case of a 36-year-old woman who presented at 36 weeks of gestation with breech presentation and HUS triggered by placental abruption. The patient was admitted for a Caesarian section (C-section) with post-op complications of pelvic hematoma and bilateral hydronephrosis. The patient improved on treatment with eculizumab after poor response to plasmapheresis and showed no signs of relapse.
Case presentation
We present the case of a 36-year-old female with a medical history of recurrent miscarriages, elective abortion, negative anti-phospholipid syndrome, chronic obstructive pulmonary disease (COPD), vitamin B12 deficiency, and a history of provoked pulmonary embolism (PE), who presented to the emergency department for a C-section following premature rupture of membranes (PROM) due to breech presentation. She had previously undergone bilateral tubal ligation three years prior. Other than her pregnancy, her physical examination was unremarkable. Post-C-section, she developed complications including pelvic hematoma and bilateral hydronephrosis. Severe anemia developed as a result of these complications, necessitating 15 blood transfusions, multiple platelet transfusions, fresh frozen plasma (FFP), and cryoprecipitate. To manage her condition, she underwent the placement of bilateral nephrostomy tubes and an inferior vena cava (IVC) filter. Due to the severity of her anemia and the need for transfusions, anticoagulation therapy was discontinued.
The patient's laboratory tests indicated low haptoglobin levels. Tests for heparin-induced thrombocytopenia (HIT)/serotonin release assay (SRA) and direct and indirect Coombs were negative. Detailed results of the patient's laboratory tests can be found in Table 1. The patient's peripheral blood smear, presented in Figure 1, revealed the presence of schistocytes. In addition to these findings, the patient was experiencing hematuria, likely due to the nephrostomy tube, thrombocytopenia, and skin bruising. Additionally, a chest X-ray was performed, the results of which were normal, as can be seen in Figure 2. It is important to note that the patient has a history of a provoked PE from a year ago, which occurred during her last pregnancy following knee surgery and a long-distance flight. Following this event, a thorough thrombophilia workup was conducted to assess her risk of blood clots. This included tests for lupus anticoagulant, homocysteine, and anti-thrombin III which were all negative.
Peripheral smear showing schistocytesArrow shows schistocytes
X-ray of the chest with no significant findings
The patient underwent a CT scan of the abdomen and pelvis, which showed bilateral nephrostomy tube placement with a resolution of hydronephrosis, renal cortical enhancement likely acute tubular necrosis (ATN), given recent contrast, and pelvic hematoma as shown in Figure 3 and Figure 4. The patient had worsening renal failure, thrombocytopenia, and MAHA, leading to a significant concern regarding thrombotic microangiopathies. One week after the patient's presentation, a renal biopsy was done which showed acute diffuse thrombotic microangiopathy involving glomeruli and vessels. It also indicates acute tubular injury, interstitial fibrosis, and atrophy with moderate arteriolar thrombi and mucoid degeneration of arteries. The biopsy findings suggested eclampsia vs. aHUS.
CT scan of the abdomen and pelvis showed bilateral nephrostomy tube placement with a resolution of hydronephrosis, renal cortical enhancement, and pelvic hematomaArrow shows pelvic hematoma
CT scan of the abdomen and pelvis showed bilateral nephrostomy tube placement with a resolution of hydronephrosis, renal cortical enhancement, and pelvic hematoma.Arrow shows pelvic hematoma
The patient's differential diagnosis for MAHA includes thrombotic thrombocytopenic purpura (TTP), HUS, disseminated intravascular coagulation (DIC), as well as rheumatologic disease, hemolysis, elevated liver enzymes, and low platelets (HELLP), and drug-induced TMA. Normal levels of ADAMTS13 ruled out TTP. aHUS was on high differential due to renal failure, and renal biopsy supported this diagnosis. The patient was seen by hematology and diagnosed with pregnancy-induced aHUS. The patient's ADAMTS13 levels were within normal limits. Complements C3 and C4 and factor H were within normal limits. The patient had low vitamin B12 levels, for which intramuscular injections were started.
Without improvement, the patient was started on plasmapheresis on the fourth day of presentation for a total of five days. After plasmapheresis, the patient's platelets stabilized, but she continued to have schistocytes on the peripheral smear. The patient was transferred to a tertiary center for close monitoring. She was given the first dose of eculizumab two days after finishing plasmapheresis, which did not result in much improvement. The patient underwent a second dose of eculizumab, which resulted in massive improvement. The trend of platelets and creatinine is shown in Figure 5 and Figure 6. The patient's hemoglobin and platelet started to improve. Her creatinine, AKI, and potassium have begun to improve as well. Hydronephrosis improved on repeat imaging, and percutaneous nephrolithotomy (PCN) was removed after two weeks. The patient was discharged home with follow-up eculizumab doses to complete the course. The plan was to do eculizumab 900 mg weekly for four weeks and then 1200 mg on week 5, followed by 1200 mg every two weeks until seen by hematology and decided to stop. The patient was vaccinated against meningococcal with eculizumab due to the risk of meningitis.
Trend of platelets during the hospital stay
Trend of serum creatinine during the hospital stay
Discussion
We report a case of aHUS associated with pregnancy in the antepartum period in a 36-year-old woman who underwent C-section delivery due to breech presentation. In this instance, C-section delivery was further complicated by hydronephrosis and pelvic hematoma. While Fakhouri et al. found 80% of pregnancy-associated aHUS cases to occur in the postpartum period, our case is unique in that it occurred antepartum (36 weeks of gestation) [8]. Another study by Fakhouri et al. reported a mean time to diagnosis of 1.4 months, whereas our patient began treatment within six days [9].
Eculizumab has become more common in treatment protocols, primarily as a second- or third-line agent after intravenous (IV) corticosteroids, hemodialysis, and plasma exchange [10]. Plasma exchange remains the standard of care in cases where TTP, STEC HUS, or secondary microangiopathies haven't been ruled out [11]. It exerts a therapeutic effect by replacing deficient complement regulators and removing autoantibodies. Eculizumab has been found to lower rates of renal failure, dialysis, and death and to increase rates of disease remission [10]. While no protocols for eculizumab use in pregnant patients are available, the recommended dose for a 70 kg adult is 1200 mg twice weekly [12]. Adverse effects include an increased susceptibility to meningococcal infections, requiring patients to receive meningococcal vaccination two weeks before starting the drug; however, the benefits of treatment still outnumber the risks [13]. Treatment with longer-acting C5 inhibitors such as ravulizumab is recommended for six weeks with a lower treatment burden [14,15].
HUS is mainly a diagnosis of exclusion. In our patient, HUS was confirmed based on history and laboratory results. Our patient displayed all the hallmarks of HUS, including MAHA (4-7 schistocytes on peripheral smear and hemoglobin 7.1 g/dl), thrombocytopenia (platelets 84,000 per microliter), and signs of end-organ damage confirmed via a CT scan of the abdomen and pelvis.
Further confirmation of HUS came from the patient's normal ADAMTS13 score of <10. C3 complement levels are usually reduced; however, in this case, they were normal, making this an abnormal finding. A common finding in aHUS includes gene encoding factor H mutations. However, factor H levels in our patient were also normal [15,16]. Additional testing would be required to rule out genetic predisposition. While plasma exchange was started early, it failed to improve symptoms. The patient was then treated with eculizumab, which improved symptoms and remission [17,18].
It is unclear when to consider future pregnancies for our patient; measures such as a renal biopsy may be prudent to assess the degree of renal injury. Australian guidelines recommend a treatment duration of 24 months [16]. Considering complement regulation disorders are prevalent in 70% of HUS cases in pregnancy, genetic analysis such as exome sequencing should be considered to assess the risk of relapse and help plan future treatment strategies [15,19]. aHUS is a rare but life-threatening condition that should be considered in patients presenting with thrombocytopenia and acute renal injury. This report may help physicians consider the possibility of HUS in patients presenting with similar presentations in the antepartum period for timely diagnosis and treatment.
Conclusions
This case report highlights the critical role of timely recognition and intervention in the management of aHUS during pregnancy. The administration of eculizumab showed a remarkable improvement in the maternal condition without adverse fetal outcomes, underlining its potential as a lifesaving and effective treatment strategy. Clinicians must consider aHUS in the differential diagnosis of pregnant patients presenting with MAHA and renal impairment. Early consultation with a multidisciplinary team, including nephrology, hematology, and maternal-fetal medicine specialists, is vital to optimize outcomes. Moreover, this case adds to the growing body of evidence supporting the safety and efficacy of eculizumab in pregnancy, which may pave the way for more robust, future prospective studies. Ensuring the availability of eculizumab and developing protocols for its use in similar clinical scenarios could significantly improve maternal and fetal prognoses. We advocate for including eculizumab in treatment guidelines for aHUS in pregnancy, supported by further research to strengthen and validate our findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Complement disorders and hemolytic uremic syndrome Curr Opin Pediatr Joseph C Gattineni J 2092152520132339957010.1097/MOP.0b 013e 32835 df 48a PMC 3758882 · doi ↗ · pubmed ↗
- 2Consensus regarding diagnosis and management of atypical hemolytic uremic syndrome Korean J Intern Med Lee H Kang E Kang HG 25403520203193531810.3904/kjim.2019.388PMC 6960041 · doi ↗ · pubmed ↗
- 3Obstetric nephrology: pregnancy and the kidney--inextricably linked Clin J Am Soc Nephrol August P 20712072720122322109710.2215/CJN.09450912 · doi ↗ · pubmed ↗
- 4The complement system and adverse pregnancy outcomes Mol Immunol Regal JF Gilbert JS Burwick RM 56706720152580209210.1016/j.molimm.2015.02.030PMC 4447554 · doi ↗ · pubmed ↗
- 5Plasmatherapy in atypical hemolytic uremic syndrome Semin Thromb Hemost Loirat C Garnier A Sellier-Leclerc AL Kwon T 6736813620102086564510.1055/s-0030-1262890 · doi ↗ · pubmed ↗
- 6Eculizumab in STEC-HUS: a paradigm shift in the management of pediatric patients with neurological involvement Pediatr Nephrol Wildes DM Harvey S Costigan CS Sweeney C TwomeyÉ Awan A Gorman KM 3153243920243749151910.1007/s 00467-023-06102-w · doi ↗ · pubmed ↗
- 7Eculizumab for paediatric patients with atypical haemolytic uraemic syndrome: full dataset analysis of post-marketing surveillance in Japan Nephrol Dial Transplant Ito S Hataya H Ashida A 4144243820233543879010.1093/ndt/gfac 150PMC 9923705 · doi ↗ · pubmed ↗
- 8Pregnancy-associated hemolytic uremic syndrome revisited in the era of complement gene mutations J Am Soc Nephrol Fakhouri F Roumenina L Provot F 8598672120102020315710.1681/ASN.2009070706 PMC 2865741 · doi ↗ · pubmed ↗