Korean Hospital Nurses’ Experiences with COVID-19: A Meta-Synthesis of Qualitative Findings
Suk-Jung Han, Hee-Jung Hong, Bok-Soon Shin

TL;DR
This study summarizes the experiences of Korean hospital nurses during the COVID-19 pandemic, highlighting their resilience and the challenges they faced.
Contribution
The study provides a meta-synthesis of qualitative findings on Korean nurses' experiences during the pandemic, offering insights for future preparedness.
Findings
Nurses overcame challenges through professional commitment and collaboration with colleagues.
Six major themes and thirteen subthemes were identified from 13 studies involving 219 nurses.
A multifaceted support system is needed to enhance nurses' resilience in future outbreaks.
Abstract
This study aims to provide a meta-synthesis of qualitative studies examining the perceptions and experiences of nurses who cared for patients in dedicated COVID-19 hospitals in South Korea. We searched key health databases (RISS, KISS, KMbase, NDSL, KoreaMed, DBpia, PubMed, CINAHL, and Cochrane) from September to November 2023. We reviewed and analyzed articles using a thematic synthesis approach. The quality of the studies was ascertained using the Critical Appraisal Skills Program checklist for qualitative research. Ultimately, 13 studies involving 219 nurses were included in the final review. Six major themes and thirteen subthemes emerged. During the unexpected COVID-19 pandemic, nurses were able to overcome difficult situations through their interactions with patients, sense of a professional mission, and commitment to nursing. Most importantly, they persevered through their…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
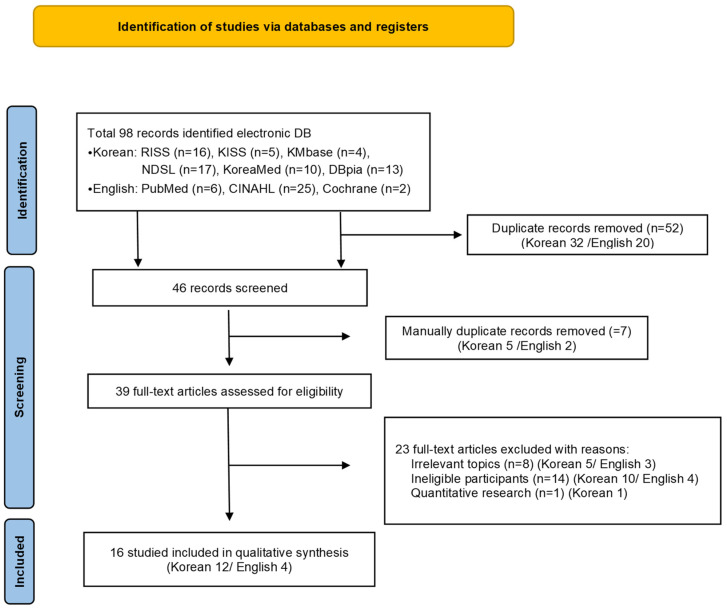 Figure 1
Figure 1- —National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and Mental Health · Disaster Response and Management · Posttraumatic Stress Disorder Research
1. Introduction
The 2019 Coronavirus disease (COVID-19) is an acute respiratory syndrome first reported in Wuhan, Hubei Province, China, on 8 December 2019. The World Health Organization (WHO) declared a global pandemic on 11 March 2020, which corresponds to the highest risk level among the WHO’s pandemic alert levels [1].
The WHO announced that it would declare COVID-19 a Public Health Emergency of International Concern (PHEIC) on 5 May 2023. This officially ended the PHEIC, which was in place for three years and four months since declared on 30 January 2020. According to the WHO’s Coronavirus Dashboard, as of 10 May 2023, the cumulative number of COVID-19 cases worldwide is close to 766 million. Deaths from the disease are reported to be close to 7 million [2].
A survey of healthcare workers infected with COVID-19 in Wuhan, China, found that nurses, who spend the most time with patients on the frontline, accounted for 52.1% of infected healthcare workers, compared to 33.6% of doctors and 14.3% of other healthcare workers [3]. Nurses are not only at risk of infection from caring for patients with infectious diseases, but also experience more mental and physical health issues than other healthcare workers [3,4,5,6,7].
In South Korea, the first case was reported on 20 January 2020, and as of 31 August 2023, the total cumulative number of cases was 34,572,554 (including 79,925 international arrivals) and 35,605 deaths [8].
COVID-19 is highly contagious and asymptomatic in its early stages. Thus, nurses were working under conditions of high anxiety and with a fear of infection. There were also conflicts and confusion about the stress of the pandemic, donning and doffing Level D protective clothing, and nursing roles [9]. These experiences may vary depending on the social, cultural, and situational context of the country, as well as COVID-19-related health policies, nurses’ social status, societal perceptions of nurses, and healthcare resources [10]. Certainly, the success of an infectious disease response depends on strategies to manage the human factors of the healthcare workforce, especially those with a direct and critical role in patient care [11]. Therefore, examining the experiences of healthcare workers who transitioned and operationalized hospital functions and systems in a short period is important in shaping policy for future infectious disease responses.
Nurses reported that in the early stages, they overcame these challenges through psychological adjustment, life adjustment, altruistic behavior, team support, and rational thinking. In the later stages, they reported increased affection and gratitude, development of professional responsibility, and opportunities for self-reflection [12]. However, nurses also self-isolated out of fear of infecting others with COVID-19, which led to social isolation, depression, and physical, mental, and social stress [9].
Based on previous experience with infectious disease outbreaks such as the H1N1 influenza in 2009, Middle East respiratory syndrome (MERS) in 2015, and COVID-19 in 2019, humans can predict other emerging infectious disease outbreaks [13]. Therefore, the experience of nurses caring for COVID-19 patients in the context of a protracted pandemic needs to be more closely scrutinized [14].
A meta-analysis encompasses the knowledge that can be accessed by reviewing topics in a research area and the process by which that knowledge can be expanded. They guide new contributions that are important in understanding and advancing a research area [15].
Therefore, this study aims to compare, analyze, interpret, and synthesize the results of qualitative studies on the patient care experiences of hospital nurses in Korea during the COVID-19 pandemic. The purpose is to better understand the context and outcomes of meaningful common experiences and adaptations in nurses’ experiences. Furthermore, this study aims to provide a basis for the development of practical coping strategies for hospital nurses caring for patients with emerging infectious diseases in the future.
2. Materials and Methods
This research is a qualitative meta-synthesis study that analyzed and synthesized individual qualitative research results on the experiences of nurses during COVID-19.
The research question explored through each qualitative study is: “What are the experiences of hospital nurses in South Korea during the COVID-19 pandemic?”
This study adhered to the guidelines in “Enhancing Transparency in Reporting the Synthesis of Qualitative Research” (ENTREQ) [16].
2.1. Search Strategy and Selection Criteria
This study searched academic databases for qualitative studies on the experiences of Korean nurses during the COVID-19 pandemic published until 2023. All searches took place from the inception, with final searches taking place from September to November 2023.
The six major databases in Korea are the Research Information Sharing Service (RISS), Korean studies Information Service System (KISS), Korean Nursing Database (KMbase), National Digital Science Library (NDSL), KoreaMed, and DataBase Periodical Information Academic (DBpia). The three major international databases are PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), and Cochrane. These nine databases were used in the study.
The search was divided into domestic and international publications. Search expressions were constructed by concatenating keywords and MeSH terms with an “AND”. Repeated searches were conducted using nurse* or nurse (MeSH terms), COVID-19 (MeSH term), experience, and Korea (MeSH term). To meet the needs of different databases, the search strategy was tailored to each. For the international databases, we used only “Korea” as a search filter to ensure a comprehensive search (Appendix A).
2.2. Inclusion and Exclusion Criterion
The detailed inclusion and exclusion criteria used to select articles that would be useful as data for the meta-synthesis of nurses’ COVID-19 experiences are as follows.
Inclusion criteria for the study subjects were as follows: (1) The study population was limited to nurses who worked in hospitals in South Korea during the COVID-19 pandemic. (2) Only articles that specified the use of qualitative research, such as phenomenological and content analysis methods, and analyzed the results according to the specified data analysis methods were included. (3) Only articles published in Korean or English were included.
Articles were excluded if they (1) did not present specific qualitative research methods or presented only results without specifying the data collection and analysis process; (2) were not published in a journal, such as a thesis; and (3) were written in a language other than Korean or English.
2.3. Study Inclusion
The screening process adhered to the Preferred Reporting Items for Systematic Reviews (PRISMA) protocol [17]. Figure 1 shows a flowchart of the selection process.
In total, 98 articles were retrieved from the literature search, including 16 from RISS, 5 from KISS, 4 from KMbase, 17 from NDSL, 10 from KoreaMed, 13 from DBpia, 6 from PubMed, 25 from CINAHL, and 2 from Cochrane, and 52 duplicates were removed using EndNote. The titles and abstracts of each study were reviewed. Consequently, an additional 7 duplicates were removed, resulting in 39 primary extracts.
After reading and checking the full text of the 39 extracted articles, we found 8 studies that were not relevant to the topic. These focused on experience with a COVID-19 patient care education program (1), perinatal and neonatal nursing experiences (1), parenting experiences of nurses with elementary school children (1), experiences of hospice palliative care nurses (1), experiences of attending a graduate school for a nurse practitioner program (1), emergency nurse–patient communication (1), art-based narrative research (1), and experiences of wearing personal protective equipment (1). Furthermore, in 14 studies, participants were not nurses who directly cared for COVID-19 patients (ineligible participants). The participants in these studies were nurse managers (1), new nurses (2), nursing home nurses (4), volunteers (1), infection control nurses (1), health center nurses (1), nursing students (3), and airline nurses (1). Thus, 23 articles were removed, including 1 quantitative study. After a secondary screening, 16 studies were selected for the purposes of our study. Of these, 12 articles were written in Korean and 4 in English (Figure 1).
2.4. Study Selection
All articles found through the search were sent to Endnote20 (Clarivate Analytics, Philadelphia, PA, USA) and duplicates were removed. Two reviewers (Han, S.-J. and Hong, H.J.) screened the titles and abstracts of the articles against the inclusion and exclusion criteria, and then read the full text of articles to identify those that met these criteria.
Two researchers independently reviewed the data and decided on the selection. In the case of disagreement or uncertainty, the researchers exchanged opinions and reached a consensus, and the reasons for selection or deletion were recorded.
We removed some studies from the list because they were not relevant to hospital nurses, such as those about the experiences of nurses working for airlines, those that focused solely on the experience of wearing PPE, the experiences of nurse managers in nursing homes, the experiences of nurses working in drive-through screening centers, and other quantitative studies.
2.5. Quality Assessment
Three reviewers (Han, S-J., Hong, H.-J. and Shin, B.-S.) critically appraised the quality of the articles included in this study using the Critical Appraisals Skills Programme (CASP) [18]. Any disagreements about the quality assessment were discussed until a consensus was reached.
In this study, the 16 included articles were cross-appraised by three researchers using the CASP checklist items to assess their quality.
The quality assessment consists of 10 questions dealing with the following aspects: “Clarity of statements”, “appropriateness of qualitative research methods”, “appropriateness of research design”, “appropriateness of data collection”, “relationship between researcher and participants”, “consideration of ethical issues”, “rigor of data analysis”, “clarity of results statements”, and “value of the study”. Each representative question has a detailed description and can be answered with yes/no or state that no answer was provided.
The quality assessment is presented in Table 1.
The quality assessment resulted in 1 yes/no or no answer in 3 of the 13 studies. When researchers had different ratings for the same study, consensus was reached through discussion. While assessing the quality of individual articles for a synthesis is an important step, there is no consensus on its benefits. It has also been recommended that the results of the assessment should not be used as a criterion for deciding whether to include an article in the analysis [19]. Thus, we did not exclude qualitative studies from the analysis of the qualitative meta-synthesis based on their quality.
2.6. Characteristics of Included Studies
The research design of the included studies was as follows: nine used phenomenological methods, one used a grounded theory method, two used descriptive case studies, three used content analyses, and one used a focus group interview.
The sample size of the studies ranged from 10 to 30, with a total of 219 nurses participating. The data collection period of each study ranged from May 2020 to November 2021, and the results of each were summarized around the main theme.
Most workplaces were nationally designated COVID-19 hospitals, but university, secondary, and tertiary hospitals were also included. The workplaces included isolation wards, infection wards, intensive care units, and screening clinics for COVID-19 patients. The Seoul metropolitan area in South Korea had the largest number of participants, and they were evenly distributed across the country, except for Gangwon Province and Jeju Island.
The main characteristics of the studies included in this study-literature list Supplementary—as well as ‘aims of study’, and ‘the main theme identified’ are presented in Table 2.
2.7. Data Extraction and Synthesis
This study integrated and analyzed the experiences of nurses working in a dedicated COVID-19 hospital in Korea during the COVID-19 pandemic. The qualitative findings extracted for data synthesis were analyzed inductively using the thematic synthesis method of qualitative research developed by Thomas and Harden [20].
For this study, we used the six-step qualitative meta-synthesis procedure proposed by Noblit and Hare [21] and modified by Atkins et al. [22]. Step 1 identified nurses’ experiences during the COVID-19 pandemic as the area of interest. In step 2, we searched for and selected the literature relevant to step 1.
In step 3, we repeatedly read the selected articles for analysis within individual studies and summarized the study objectives, the main findings, and the central concepts and themes for each study.
In step 4, we continuously compared and analyzed the results of individual studies based on the tables created in steps 2 and 3, and the data, organized by study, to analyze the associations between individual studies. Analyzed.
In step 5, we identified the technical themes identified in step 4. Technical themes are the concepts, themes, and explanations presented by the authors of the analyzed papers, as well as themes based on interview quotes.
Finally, step 6 synthesizes the findings from the previous steps to explore new interpretations and theory generation. In this study, we applied a second level of synthesis to the results analyzed in step 5 to generate synthesized themes in order to draw expanded interpretations.
During the meta-synthesis process, the authors met seven times to review and discuss the results of the within-study and between-study association analyses and second-level synthesis from steps 3 through 6, coordinate their opinions, and make iterative revisions.
Three researchers (Han, S-J., Hong, H.-J., and Shin, B.-S.) read the results of each article individually and summarized the author’s name, year of publication, purpose of the study, research method, participants, department, data collection period, type, and location of the hospital. The results are shown in Table 1.
For the meta-synthesis, each researcher repeatedly and carefully read all the content, including the title, topic, categories, and citations, and extracted and organized all the codes to be analyzed. The organized codes were repeatedly reviewed based on the commonalities, differences, and similarities of each content type, and the reviewed content was categorized into subthemes. The categorized codes were continuously reviewed against other codes and revised if necessary. Finally, themes were inductively synthesized around the final classified subthemes.
3. Results
The synthesis of Korean hospital nurses’ experiences of caring for patients with COVID-19 resulted in 6 themes and 13 subthemes. The six themes are as follows: “The crisis of a pandemic that suddenly appeared”, “challenges in nursing patients with infectious diseases”, “a struggle in an unknown time due to a prolonged infectious disease”, “ethical dilemmas in the face of infectious diseases”, “duality of the social support system”, and “professional growth for nurses regarding infectious diseases”. Next, each topic and subtopic are described with illustrative quotes. Each major topic and subtopic are shown in Table 3.
The crisis of a pandemic that suddenly appeared
Participants felt the “crisis of a pandemic that suddenly appeared” as an initial emotion when COVID-19 first appeared. This manifested as a vague fear of the virus and of the rapid spread of this uncertain infectious disease. Nurses struggled during the COVID-19 pandemic without any preparation.
(1)Vague fear about COVID-19
There was a ‘vague fear of COVID-19’ in the nursing environment that none of the participants had ever experienced before.They felt the fear of being thrown into an unknown world where they had to provide nursing care without much knowledge.
Participants described it as being like World War III, where everything felt threatening and uncertain, leading to a sense of panic in the midst of the crisis (A2, A4, A6, A7, A8, A9, A10, A11).
(2)Fear of spreading infection
Participants experienced concern and anxiety regarding the possibility of contracting COVID-19 and of spreading it to others. Fear was a physical, mental, and social stress that led to the development of a catatonic fever. They also felt socially isolated, and their daily routines were disrupted as they chose to self-isolate to avoid spreading the infection to others (A1, A2, A3, A4, A5, A7, A8, A10, A11, A16).
2.Challenges in nursing patients with infectious diseases
This aspect dealt with providing care for patients with infectious diseases, which differs from that provided through conventional nursing. In this case, the difficulties caused by the confusion generated by the response guidelines for COVID-19, an unprepared-for infectious disease, and the work overload experienced by nurses emerged.
(1)The chaos of providing nursing care for an unprepared for infectious diseas
Participants experienced much confusion in their daily tasks and had difficulty understanding and implementing the often-changing guidelines and instructions. Conflicting tasks, ambiguous instructions, and unclear standards due to the quarantine situation led to confusion. This confusion escalated and was compounded when following instructions.
Participants endured uncomfortable physical pain and discomfort from wearing personal protective equipment (PPE), and experienced poor working conditions and a lack of skilled labor (A1, A2, A4, A5, A6, A7, A8, A9, A10, A11, A13, A16).
(2)Taking on the unique and distant tasks of nursing
Participants felt overwhelmed and exhausted as they were delegated tasks outside their purview, including cleaning and disinfection, excessive demands from carers and patients (deliveries, errands), and the work of other healthcare staff (caregiving, X-rays, drawing blood). These tasks were in addition to their own nursing duties and were further complicated by minimal staffing and restricted access to outsiders for fear of infection (A2, A6, A10, A13, A16).
(3)Specialized care for people with COVID-19
The COVID-19 pandemic has changed the perception that nurses can provide special nursing care for patients. Instead, they must provide holistic nursing care, which may differ from traditional nursing care. Unlike the previous task-oriented nursing care, nurses were closer to patients’ lives and practiced patient-centered nursing care. Participants talked about their daily lives with the patients and played games with them, viewing these as moments in which to fight and beat the disease together (A1, A3, A7, A8, A11, A12).
3.A struggle in an unknown time due to a prolonged infectious disease
This theme is a story of professionalism in the time of uncertainty that still remains.
(1)Burnout in sacrifice
Behind the scenes, participants who cared for patients with COVID-19 were experiencing sacrificial burnout. Despite the sacrifices made by their families and the high intensity of their work as nurses, they felt relatively deprived due to inadequate treatment (A2, A3, A4, A8, A9, A16).
(2)Having a sense of professional mission as a nurse
Participants felt a sense of pride and reward in their professional mission as nurses during COVID-19 that they had not yet felt before and considered it a valuable experience. The pride and sense of a professional mission, of being on the frontline during the pandemic, increased their motivation and self-esteem regarding nursing. Here, participants found the support of patients, family, and friends very rewarding (A2, A3, A4, A5, A6, A7, A8, A9, A10, A11, A12, A16).
4.Ethical dilemmas in the face of infectious diseases
Participants experienced ethical conflicts at both the personal and client levels during the COVID-19 pandemic. At the personal level, nurses were constrained in their behavior by their obligation to care for patients with a severe infectious disease despite the risk of exposure to infection, and by their family members due to their contact with patients with the virus. They also experienced strong ethical conflicts regarding their patients, especially feelings of grief and helplessness about not being able to ensure the dignified death of their charges.
(1)Agony over lost human dignity
Participants experienced guilt and distress due to their inability to protect human freedom and dignity during the COVID-19 pandemic, including end-of-life care and CCTV installation. They had to control their caregivers to prevent the spread of infection before a patient’s end-of-life. They could also not provide proper aftercare because they were at risk of becoming a source of infection, preventing them from enabling a patient to die with dignity. They experienced a sense of helplessness in their professional role as they were unable to deliver the deceased patient’s belongings to their families because they were infected. They also experienced ethical conflicts such as forced hospitalization and isolation against the free will of patients or their guardians, and the observation of patients through CCTV, which invaded their privacy (A2, A3, A6, A8, A9, A11, A13).
(2)Conflict between nursing principles and uncontrollable situations in infectious disease situations
The time of COVID-19 was chaotic, and nurses were challenged by the frequent changes in the beliefs regarding infection and conflict between patients and careers who were unable to accept these challenges (A9, A15, A16).
5.Duality of the social support system
This theme embodies a social campaign to thank nurses for protecting the public’s health in the difficult period of COVID-19. However, it also had another meaning, in which nurses were stigmatized as “infected” and isolated based on the perception that they were in direct contact with patients who were infected, and thus at high risk of infection themselves. It was also a collaboration between colleagues who supported each other and held the frontline of COVID-19 under difficult circumstances.
(1)Heroes in the media and stigma in the real world
While the media promoted nurses caring for patients with COVID-19 as heroes, participants who encountered those who were infected were stigmatized as carriers of infection, leading to avoidance and social isolation. Participants’ personal lives were sacrificed when they became infected, as they had to self-isolate and stay in confined spaces. They also experienced the duality of nurses being forced to make social sacrifices while hidden behind the image of being a “hero” (A1, A4, A6, A9, A14).
(2)Community of practice through peer-to-peer collaboration
As difficult as the COVID-19 pandemic has been, participants have found solace in sharing their challenges with their colleagues and encouraging each other. In the isolation ward, which felt like an island, they helped each other with protective gear, and communication between colleagues became smoother and more collaborative. Even though they had different backgrounds and experiences, they relied on each other, sharing common goals to provide quality care and form a quarantine community (A2, A4, A5, A6, A11, A14, A16).
6.Professional growth for nurses regarding infectious diseases
Participants aspired to emulate Nightingale, a nurse on a battlefield doing her best to provide care under adverse conditions. As a nurse, she gained professional knowledge and skills in infectious diseases, improved her ability to respond to infectious diseases, and gained personal growth and a sense of responsibility and mission.
(1)Improved response to infectious diseases
Participants reported that the experience of nursing during COVID-19 provided them with practical training in infectious diseases, which enhanced their professional nursing skills in terms of preparedness and response systems for future outbreaks of new infectious diseases (A1, A5, A12, A16).
(2)Promote pride in being a nurse
Participants reported that although their nursing experience during COVID-19 was challenging, they felt proud to be able to care for patients. They also felt a great sense of accomplishment when their patients improved and were discharged, safe from death’s door. These experiences made them feel rewarded by the profession and gave them a sense of responsibility and calling. It was also an opportunity to gain social recognition, and they experienced pride and growth as nurses (A2, A3, A5, A6, A7, A9, A11, A12, A15, A16).
4. Discussion
4.1. Summary
This study is a meta-synthesis of existing qualitative research on Korean hospital nurses’ experiences of caring for patients with COVID-19. Based on these findings, we suggest the need for a practical response strategy for the emergence of new infectious diseases in the future and suggest ways to improve the response. This study also provides directions for future research to better understand nurses’ experiences with COVID-19 and to develop practical interventions for hospital nurses caring for patients with emerging infectious diseases.
4.2. Comparisons with Existing Knowledge and Implications for Practice
Since the 2000s, the healthcare community has experienced numerous infectious diseases of national disaster proportions, including Severe Acute Respiratory Syndrome (SARS) in 2003, Influenza A virus subtype H1N1 in 2009, and MERS in 2015. This study aims to compare the holistic nursing experience of these infectious diseases and that of COVID-19.
The first theme, “the crisis of a pandemic that suddenly appeared”, was the vague fear of uncertainty and of spreading infection participants experienced while caring for patients with COVID-19. This was consistent with previous studies of nurses’ experiences with a similar infectious disease, MERS, which found that anxiety and fear were heightened by concerns regarding contagion and uncertainty about how the situation would evolve in the future [23,24]. Studies have also found that the threat of the COVID-19 pandemic was represented as a war, and that the world shared a climate of fear [25]. As nurses were in the closest contact with patients during the COVID-19 pandemic, they experienced anxiety about the possibility of infection and the transmission thereof to their families [26,27]. Thus, it is necessary to monitor their mental and psychological state and provide appropriate emotional support. In a study of SARS, an infectious disease similar to COVID-19, nurses’ negative emotions decreased and their positive attitudes increased as their knowledge of the disease increased, reducing anxiety and stress [28].
Therefore, this suggests that it is necessary to secure specialized nursing personnel who can provide sufficient education and accurate information and respond quickly, and to have a nursing system that can support a multifaceted support system.
The second theme, “challenges in nursing patients with infectious diseases” represents the confusion in infectious disease care and nurses’ overwhelming workload, caused by a lack of guidance on how to respond to the virus. Inadequate facilities, ambiguous standards, and insufficient training added to the confusion, while the physical discomfort of wearing protective equipment and the intensive workload faced by nurses led to victimization and burnout. Although the COVID-19 pandemic is different due to its prolonged duration, Korea developed guidelines and improved its epidemic prevention system in response to the risk of the transmission of a new infectious disease following the 2015 MERS outbreak [29]. Nevertheless, inadequate standards and guidelines for infectious diseases added to the confusion. Consistent with our study, research on Taiwanese nurses during an outbreak of SARS abroad found that they were confused by the lack of information, lacked adequate support (PPE, staffing), and experienced occupational stress due to a heavy workload and the operation of numerous types of equipment during nursing care [30].
Therefore, based on the experience of COVID-19, it is necessary to improve the ability to cope with future epidemics and establish a clear reference point and system to improve the quality of nursing care. An empirical study on the work of nurses in hospitals dedicated to COVID-19 showed that the principles, methods, and effects of staffing support need to be evaluated in the future, and that staffing guidelines and systems that can be used to determine appropriate assignments, numbers, and timing, considering the content and difficulty of tasks, must be established [31]. Therefore, the government and domestic medical institutions should prepare standardized guidelines regarding nursing patients with infectious diseases in advance. Furthermore, additional support such as regular infectious disease education and settling into the work environment should be provided so that medical staff can perform their tasks according to the guidelines in the event of an infectious disease outbreak [32].
On the other hand, nursing experiences during COVID-19 changed the perception of traditional nursing work. Viewing patients as human beings and interacting with them reaffirmed the value and meaning of nursing in providing holistic care for patients with COVID-19. This is similar to previous studies that showed that the pandemic led to authentic nursing [9], and that such experiences enhance the responsibility and motivation for patient care [33]. Therefore, it is necessary to promote positive emotions and adaptation so that healthcare workers can fulfill their responsibilities while being recognized as valuable human resources in a national disaster situation.
The third theme, “a struggle in an unknown time due to a prolonged infectious disease”, dealt with nurses enduring a difficult time with a sense of their mission but while experiencing burnout due to work overload in the real world. Nurses’ work overload refers to the demands of multiple conflicting roles, and the conflict between roles is known to exacerbate emotional burnout [34]. In addition, policies that minimize social contact with patients impose an additional workload on nurses, leading to burnout [35].
Healthcare systems will need to develop strategies to create a work environment that allows nurses to focus on caring for patients and to establish a clear scope of practice. In addition, to prevent burnout in the nursing workforce, nurses’ dedication should be recognized and adequately rewarded. Furthermore, the government should provide comprehensive policy support to address the wage gap between nurses, as the unequal economic rewards and inadequate treatment despite the high intensity of their work can lead to conflict among members.
In this study, nurses had a sense of professional mission during the COVID-19 pandemic, as reported in previous studies. They felt pride in providing care and fulfilling their responsibilities during a national disaster [36]. This is consistent with the pride of nurses who cared for patients with COVID-19 in Wuhan, China [37]. Support from patients, family, and friends was a source of strength and motivation, allowing nurses to endure difficult situations with a sense of a professional mission and belief that they could do this because they were nurses. Given the findings that nursing care is driven by a sense of mission [38], it is necessary to create a positive nursing environment by recognizing the importance of social support systems in overcoming infectious diseases.
The fourth theme, “ethical dilemmas in the face of infectious diseases”, deals with the multiple ethical conflicts participants faced in the chaotic healthcare setting of COVID-19. Their personal ethical values clashed with their expected roles as professional nurses in the face of an infectious disease. We explore these situations according to the four principles of ethics outlined in the 1979 Belmont Report. First, the dilemma regarding the principle of autonomy is that patients infected with COVID-19 were forcibly admitted and isolated by the government, regardless of their autonomy. Restraints were applied in uncontrollable situations, their guardians could not be with them, the doors to their rooms were locked from the outside, and there was no guarantee of privacy as patients were monitored through CCTV. Second, the dilemma of the principle of doing good is that the COVID-19 medical field did not have proper guidelines and the policies changed daily, causing inconvenience to patients who were not infected. Third, the dilemma of the principle of non-maleficence is that nurses became infected and self-isolated, leaving them unable to provide adequate care to patients due to staff shortages. Finally, the dilemma of the principle of justice was that participants were led to discriminate against the infected, as they were concerned about becoming carriers of the infection and causing harm to their families by providing nursing care for COVID-19 patients. These results were consistent with the findings of Park’s [39], who found that the principles of autonomy and of doing good were significantly influenced by the principle of justice. In Torda’s [40] study on SARS, healthcare workers were found to provide care despite the infringements on personal freedom, difficulties in maintaining privacy, and personal risk to them. Sperling’s [41] found that nurses involved in the COVID-19 response were more influenced by clinical ethics, which focuses on the values and rights of the individual client, than public health ethics, which is based on utilitarianism and focuses on the population and public good.
The fifth theme, “duality of the social support system”, is consistent with the findings of this study, as nurses’ experiences of caring for MERS patients showed they were performing important roles and functions in society as a profession. However, they also perceived themselves as victims of infection and risk factors for disease transmission [42]. In the COVID-19 pandemic, which was new to everyone, participants realized the importance of sharing knowledge and collaborating with their colleagues [43]. They described this as “comradeship” [44] and became “comrades”, sharing a sense of closeness and identification [45]. According to Chiang et al. [46], nurses who cared for patients with SARS expressed the bond between colleagues as stemming from their “being in the same boat”. This positively impacted the care provided for patients with SARS due to the improved collaboration between colleagues, which is consistent with the results of this study. In addition, the experience of patients with MERS also reflected the successful collaboration between colleagues [44,45]. In the COVID-19 pandemic, nurses’ solidarity with their colleagues was found to be a complementary positive relationship, consistent with the results of this study [47]. For nurses, the interaction between colleagues who shared the difficulties and problems in caring for patients and co-operation with each other increased their work efficiency and improved the quality of care, which positively affected patient health outcomes and made them feel more confident in their work [48].
Finally, the sixth theme, “professional growth as a nurse regarding infectious diseases”, was consistent with previous research on the MERS epidemic, which found that participants expanded their awareness of nursing by working on a new infectious disease outside their normal duties as nurses [24]. In addition, participants experienced professional growth as nurses in infectious diseases through their COVID-19 nursing experience. These findings were consistent with previous research on the MERS outbreak, which found that nurses realized their previously unrecognized roles as nurses and vowed to engage with patients with infectious diseases in the future [24,49].
In conclusion, Korean hospital nurses’ experiences of COVID-19 were consistent with the concept of resilience, which is the ability to grow and develop through the adversity arising from a new infectious disease. Resilience is a personal characteristic that enables a person to cope effectively with adversity, providing them with the positive power and strength to overcome difficulties or stressful situations, resulting in positive outcomes [50]. Nurses with such resilience can overcome the difficulties and stresses experienced in their work and enhance their professional self-identity and competence through their ability to adapt quickly to difficult tasks [51].
Polk’s [52] mid-range theory of resilience consists of a temperamental pattern, which is an individual’s internal characteristics; a relational pattern, which is about social connections and trusting relationships; a situational pattern, which is the interaction between internal characteristics and external factors to mediate risk factors; and a philosophical pattern, which includes an individual’s beliefs and life values. Of the four patterns that make up the theory of resilience, the nurses in this study experienced COVID-19 in a relational pattern, meaning that they coped with the pandemic through their relationships with family, friends, and coworkers.
Support from family, friends, and significant others increased nurses’ psychological resilience during the pandemic [53]. Support from fellow nurses enhanced their coping skills [54]. For nurses, peer support can help them handle their work more effectively and deal with difficult situations [55,56]. These experiences lead to personal growth and increased confidence in one’s own resilience [57]. Thus, resilience is the process of emerging from the life challenges that arise in a crisis, transforming the external environment into a protective environment through potential and positive forces and converting these challenges into opportunities for growth [58]. Nurses have also found that recognition of their ability to respond to infectious diseases and pride in their role has been a source of resilience [59] and enhanced their professional competence [60], and the unique experience of the COVID-19 pandemic has led to greater resilience in well-resourced and well-organized health systems [61].
4.3. Strengths and Limitations
This study applied Lincoln and Guba’s [62] evaluation criteria to identify the strengths and limitations of the meta-synthesis.
To establish reliability, we used a comprehensive systematic review methodology and transferred it to Endnote20 (Clarivate Analytics, Philadelphia, PA, USA) to remove duplicates. We searched, extracted, and analyzed qualitative data from various databases to maintain the reliability of our findings. We also used the ENTREQ checklist [16] to increase transparency during the review. However, the applicability may be limited by several factors. First, the nurses in this study experienced COVID-19 in a variety of healthcare settings, including dedicated COVID-19 wards, emergency departments, intensive care units, and screening clinics, and their experiences may vary depending on their practice. Second, the heterogeneity of data on Korean nurses’ experiences with COVID-19 may limit our ability to understand the experiences of the pandemic in other countries. It is also important to note that the subjective nature of the analysis makes it difficult to generalize, the analysis may be at risk of bias, and the analysis may not be representative of all nurses.
To ensure reliability, we examined and agreed on the reliability of the findings based on the original texts that were included. A logical thematic analysis process was used, and the research process was documented. In addition, three experienced qualitative researchers participated in the analysis process and analyzed the data inductively using the thematic synthesis method to generate overarching themes, subthemes, examples, and quotes through a consensus process.
The strengths of this study include the use of the CASP checklist to critically appraise the included studies and the absence of potential bias, as 5 of the 16 studies did not disclose the relationship between researchers and participants. However, there may be publication bias in this meta-synthesis, as we only included studies published in Korean and studies published in English on Korean nurses.
4.4. Future Research
As a qualitative meta-synthesis study of Korean nurses’ experiences of the COVID-19 pandemic, this study was able to provide an in-depth understanding of the Korean context. However, future studies need to identify and generalize the comprehensive perspectives of nurses who have experienced infectious diseases abroad.
As it was found that the drive to overcome the COVID-19 pandemic was nurtured through relational interactions, it is suggested that future research develops programs related to overcoming difficulties in nurses’ response to the pandemic.
There is also a need for comparative analytical studies to identify differences in healthcare organizations that experienced national-disaster-level infectious diseases, including COVID-19, and the perceptions and experiences of each discipline in the nursing workforce.
5. Conclusions
This study synthesized the COVID-19 nursing experiences of Korean hospital nurses in the context of their developmental process, and found that there were problems, such as confusion regarding work identity, ethical dilemmas, and the duality of nursing support systems. Nevertheless, the nursing experience of interacting with patients, the professional mission and commitment of nurses, and the deep intimacy of colleagues working together enabled them to overcome the challenges presented by the pandemic in a positive way.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization (WHO) World Health Organization Coronavirus Disease (COVID-19)2020 Available online: https://covid 19.who.int(accessed on 4 March 2021)
- 2International Institute for Sustainable Development (IISD) SDG Knowledge Hub(News): WHO Declares End to COVID-19 as Global Health Emergency Available online: https://sdg.iisd.org/news/who-declares-end-to-covid-19-as-global-health-emergency/(accessed on 10 May 2023)
- 3Zheng L. Wang X. Zhou C. Liu Q. Li S. Sun Q. Wang W. Analysis of the infection status of the health care workers in Wuhan during the COVID-19 outbreak: A cross-sectional study Clin. Infect. Dis.202015 ciaa 58810.1093/cid/ciaa 58832409825 PMC 7239233 · doi ↗ · pubmed ↗
- 4Shaukat N. Ali D.M. Razzak J. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review Int. J. Emerg. Med.2020134010.1186/s 12245-020-00299-532689925 PMC 7370263 · doi ↗ · pubmed ↗
- 5Lai J. Ma S. Wang Y. Cai Z. Hu J. Wei N. Wu J. Du H. Chen T. Li R. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019 JAMA Netw. Open 20203 e 20397610.1001/jamanetworkopen.2020.397632202646 PMC 7090843 · doi ↗ · pubmed ↗
- 6Hao Q. Wang D. Xie M. Tang Y. Dou Y. Zhu L. Wu Y. Dai M. Wu H. Wang Q. Prevalence and risk factors of mental health problems among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis Front. Psychiatry 20211256738110.3389/fpsyt.2021.56738134211406 PMC 8239157 · doi ↗ · pubmed ↗
- 7Kunz M. Strasser M. Hasan A. Impact of the Coronavirus Disease 2019 Pandemic on Healthcare Workers: Systematic Comparison between Nurses and Medical Doctors Curr. Opin. Psychiatry 20213441310.1097/YCO.000000000000072134001698 PMC 8183249 · doi ↗ · pubmed ↗
- 8Yang S.C. Jang J.H. Park S.Y. Ahn S.H. Kim S.S. Park S.B. Ryu B.Y. Lee S.Y. Shin E.J. Kim N.Y. COVID-19 outbreak report from January 20, 2020 to January 19, 2022 in the Republic of Korea Public Health Wkly. Rep.202215796805 Available online: https://www.phwr.org/journal/view.html?pn=vol&uid=278&vmd=Full(accessed on 1 October 2023)