Primary Tubercular Chorioretinitis Without a Pulmonary Focus: A Case Report
Tyfur Rahman, Uma Gupta, Urmi Das, Tanzima Afrin, Tahmina Akter

TL;DR
A rare case of eye tuberculosis without lung involvement is reported, highlighting the challenges of diagnosing extrapulmonary TB in resource-limited settings.
Contribution
This case report presents a rare instance of primary tubercular chorioretinitis without pulmonary TB in a resource-limited setting.
Findings
The patient showed marked improvement in vision after starting antitubercular therapy.
The case illustrates the diagnostic challenges of extrapulmonary TB in areas with limited access to advanced tools.
It emphasizes the need for increased awareness of TB as a cause of ocular symptoms.
Abstract
Ocular tuberculosis (TB) can affect various eye structures and may manifest independently of systemic TB. Typically, it arises from hematogenous dissemination from a primary focus; however, in exceptional instances, it may originate as a primary infection after epithelial injury. Diagnosing TB in an extrapulmonary site presents a significant clinical challenge. We present the case of a 33-year-old Bangladeshi female who presented with a deteriorating loss of vision in her left eye. A thorough neurologic examination and serological tests, the tuberculin skin test, a CT scan of the chest, ocular fundus photography, and optical coherence tomography were performed. Based on the clinical features and the outcome of appropriate tests, a presumptive diagnosis of ocular TB was made and later confirmed after initiating antitubercular therapy, which resulted in a marked improvement in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
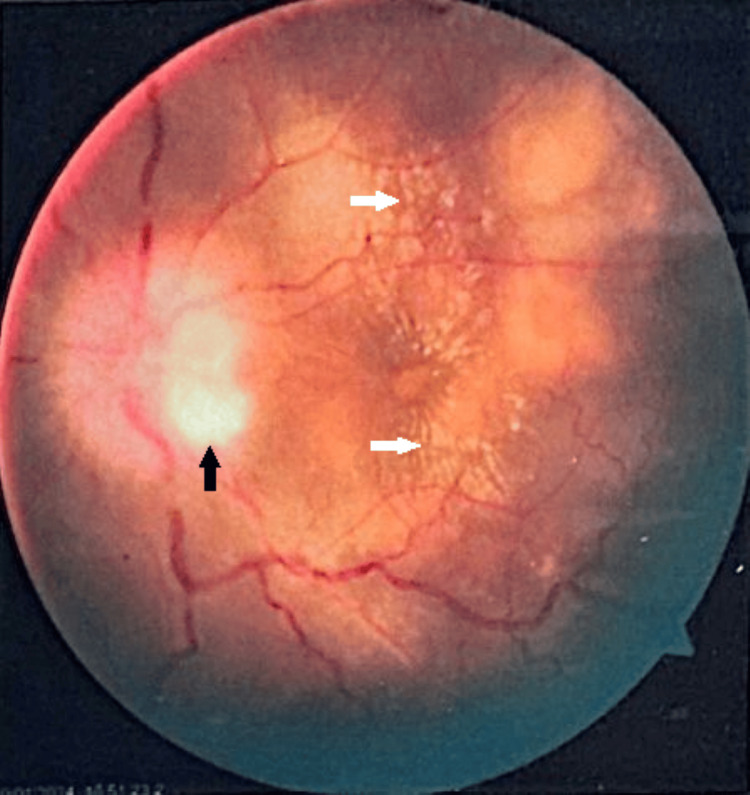 Figure 1
Figure 1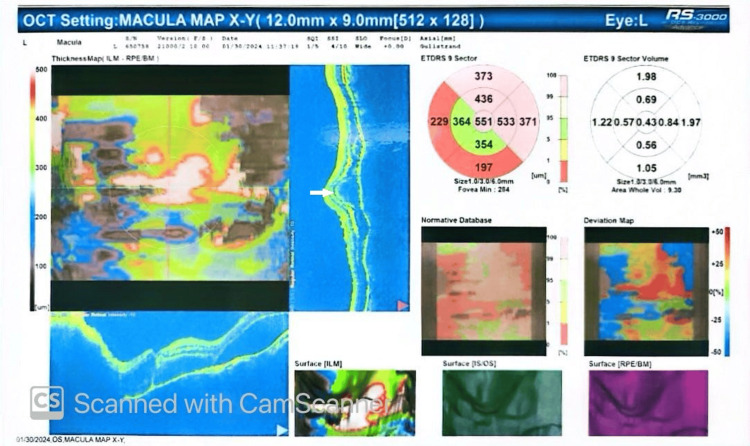 Figure 2
Figure 2| Test | Results | Reference value |
| Serum sodium | 141 mmol/L | 135–148 mmol/L |
| Serum potassium | 4.3 mmol/L | 3.5–5.3 mmol/L |
| Serum chloride | 103.0 mmol/L | 98–107 mmol/L |
| Serum bicarbonate | 21.0 mmol/L | 22–29 mmol/L |
| Serum creatinine | 0.48 mg/dL | 0.6–1.4 mg/dL |
| Hemoglobin | 11.7 g/dL | Female = 12–15 g/dL; male = 13–17 g/dL |
| ESR | 45 mm | At the end of the first hour: male = 0–10 mm; female = 0–15 mm |
| CRP | 11.8 mg/L | <3.0 mg/dL |
| Serological tests | ||
| HIV | Negative | - |
| HBsAg | Negative | - |
| Anti-HCV | Negative | - |
| VDRL | Non-reactive | - |
| TPHA | Titer <1:80 | - |
| Opinion: negative | - | |
| Test | Result |
| Date of injection | January 30, 2024, 02:06 PM |
| Dose of injection | 10 T.U. of PPD |
| Date of observation | February 2, 2024, 11:28 AM |
| On observation | Induration present |
| Diameter | 14 mm |
| Interpretation | Positive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOcular Diseases and Behçet’s Syndrome · Infectious Diseases and Tuberculosis · IgG4-Related and Inflammatory Diseases
Introduction
Tuberculosis (TB) is a global health problem. Around 2 billion people, or a quarter of the world’s population, could have TB, with 10.6 million falling ill each year. TB remains deadly despite being preventable and treatable, claiming over 3,500 lives daily and totaling 1.3 million deaths annually. Additionally, approximately 30% of TB cases are missed by healthcare screenings and diagnostics, leading to poor health outcomes and further TB spread in communities. Untreated individuals can infect 10 to 15 others per year, with 10% developing active TB in their lifetimes [1]. TB is an infectious disease that can affect various organs in the body, including the eye. The infections inflicted by TB can occur with or without evidence of systemic TB. The infection can develop following hematogenous spread, but can also occur following direct epithelial injury. Ocular manifestations of TB can mimic those of other inflammatory diseases. Establishing the diagnosis of ocular TB is a clinical challenge, as most tubercular infections affect the pulmonary system first, and primary infection of the eye is extremely rare, with an incidence of about 1% to 2% [2]. The diagnosis of ocular TB warrants a combination of ocular inflammatory signs and the demonstration of mycobacterial culture or DNA amplification of the ocular samples. A presumptive diagnosis can be proved by a combination of ophthalmologic findings consistent with TB and tests that can confirm a TB infection, such as the interferon-gamma release assay (IGRA) or the tuberculin skin test (TST) [3]. Ocular TB remains undiagnosed due to the absence of ocular biopsies, and biopsy of the retina is generally not possible. We report a case of tubercular chorioretinitis, choroidal tubercles, a very rare finding of extrapulmonary TB, diagnosed based on clinical features, optical coherence tomography (OCT) imaging findings, and a positive TST in a highly endemic setting.
Case presentation
A 33-year-old female with no previous history of diabetes or hypertension presented with blurred vision in the left eye associated with redness and pain for one month. She had a history of subjective, intermittent low-grade fever for three months, accompanied by anorexia and weight loss. While she lacked an evident contact history, she hailed from a region endemic to TB. Her immunization status was unknown. On examination of the respiratory system, there were no abnormalities. The examination of other systems was also unremarkable. Her ophthalmologic examination showed significantly decreased visual acuity in the left eye to light perception. The visual acuity in her right eye was 6/6. Regarding the field of vision, the direct and consensual light reflex was lost and absent in the left eye, which was dilated. Additionally, her accommodation was normal. On further examination, the vitreous was normal, with no signs of anterior segment inflammation. Both the intraocular pressure and anterior chamber angle were within normal limits. Initially, pupil dilation was observed as a medication-induced effect. Subsequent examinations revealed no abnormalities. An indirect funduscopic examination showed a hyperemic disc with blurred margins and an obliterated cup-to-disk ratio due to disc edema in the left eye. There were no abnormalities on the oculomotor examination.
Her complete blood count was significant for hemoglobin of 11.7 g/dL, erythrocyte sedimentation rate of 45 mm in the first hour, and C-reactive protein of 11.8 mg/dL. Her serum electrolytes, creatinine, hepatitis B surface antigen, hepatitis C virus antibody test, Venereal Disease Research Laboratory test, Treponema pallidum hemagglutination assay, and human immunodeficiency virus were unremarkable (Table 1). A CT scan of the chest showed no evidence of consolidation, collapse, or fibrosis. No hilar lymphadenopathy was observed, the cardiac shadow exhibited a normal outline, and the trachea was centrally positioned. A CT scan of the head showed no abnormalities. Her Mantoux test was positive with an induration of 14 mm (Table 2). Fundoscopy in the left eye showed papilledema with exudates around the macula (Figure 1). Her OCT showed a choroidal tubercle and a choroidal granulomatous lesion (Figure 2). Based on her demographic characteristics, clinical examination, positive TST, fundoscopy, and OCT findings, she was diagnosed with ocular TB. She was initiated on standard antitubercular therapy (ATT): rifampicin 150 mg, isoniazid 75 mg, pyrazinamide 400 mg, ethambutol HCL 275 mg, along with systemic corticosteroids (30 mg PO daily).
Fundus photograph showing papilledema and irregular optic cup-to-disk ratio (black arrow) with macular exudates (white arrows).
Optical coherence tomography showing an intraretinal lesion (white arrow).
A week after her treatment, a notable enhancement in her visual acuity to 6/9 was observed, accompanied by reduced optic disc swelling, as evidenced by indirect fundoscopy. The ocular examination findings, along with documented imaging during the follow-up period, demonstrated a significant improvement in visual acuity. We assessed visual acuity and funduscopic findings as indicators of improvement. Subsequently, a referral was made to a vitreo-retina specialist for a three-month follow-up. A repeat IGRA yielded a positive result. She responded well to ATT with steroids, confirming the diagnosis of ocular TB.
Discussion
Early diagnosis and treatment of ocular TB are vital to preserve vision and limit its spread. The documented occurrence of tubercular uveitis (TBU) shows considerable variation globally. It ranges from 0.2%-2.7% in regions where TB is not widespread, like the United States, Europe, or Japan, to 5.6%-10.5% in highly affected areas such as India [4,5]. We diagnosed our case in Bangladesh, a highly endemic region for TB. The demographic setting and densely populated area provided us with a high level of suspicion for extrapulmonary TB, which prompted further evaluation. We advised relevant investigations that allowed us to reach our presumptive diagnosis, and a positive TST made ocular TB the most probable diagnosis. The Collaborative Ocular Tuberculosis Study-1 group indicated that positive or negative test outcomes do not impact the treatment approach for the condition in real-world situations. This is because of the low sensitivity and absence of standardization [6]. Tubercular posterior uveitis (TPU), specifically tubercular choroiditis, is the most common form of TBU [7,8]. Tubercular serpiginous-like choroiditis appears as multiple, yellowish lesions with slightly raised edges that are not connected to the optic disc [8-11]. In the hematogenous spread of Mycobacterium tuberculosis (MTB), tubercles typically manifest as multiple, small, grayish-yellowish nodules. In our case, the patient presented with a choroidal tubercle and choroidal granulomatous lesion consistent with tuberculous granuloma associated with papilledema and macular exudates. The primary support for the direct involvement of MTB in the development of ocular TB lies in the positive impact of ATT on resolving inflammation or preventing its recurrence [12,13]. Conversely, the indirect influence of MTB is primarily backed by the absence of microbiological or molecular evidence of MTB in ocular fluid samples and the therapeutic effectiveness of corticosteroid therapy alone in clinically diagnosed ocular TB cases [12]. Similarly, in our case, the initiation of treatment with marked improvement of vision further confirmed the diagnosis of ocular TB in our patient.
Conclusions
We highlight the importance of a comprehensive clinical approach to facilitate diagnosing ocular TB. Following ATT (treatment protocol), the patient improved which prevented irreversible loss of vision. Our report emphasizes the need for increased awareness to alleviate the impact of any debilitating outcome. Further research and follow-up are important to enhance our understanding and treatment of ocular TB globally.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global TB overview 3 2024 2024 https://www.cdc.gov/globalhivtb/who-we-are/about-us/globaltb/globaltb.html
- 2Ophthalmologic experience in a tuberculosis sanatorium Am J Ophthalmol Donahue HC 742748641967606153210.1016/0002-9394(67)92860-7 · doi ↗ · pubmed ↗
- 3Spectral domain optical coherence tomography imaging of tubercular chorioretinitis and intraretinal granuloma. Intraretinal tuberculosis: a case report Int Ophthalmol Pirraglia MP Tortorella P Abbouda A Toccaceli F La Cava M 4454503520152581337510.1007/s 10792-015-0061-y · doi ↗ · pubmed ↗
- 4Controversies in ocular tuberculosis Br J Ophthalmol Ang M Chee SP 6910120172781527010.1136/bjophthalmol-2016-309531 · doi ↗ · pubmed ↗
- 5Tuberculous uveitis Int Ophthalmol Clin Abu El-Asrar AM Abouammoh M Al-Mezaine HS 19395020102037586010.1097/IIO.0b 013e 3181 d 2ccb 9 · doi ↗ · pubmed ↗
- 6The Collaborative Ocular Tuberculosis Study (COTS)-1 report 3: polymerase chain reaction in the diagnosis and management of tubercular uveitis: global trends Ocul Immunol Inflamm Agarwal A Agrawal R Gunasekaran DV 4654732720192926108910.1080/09273948.2017.1406529 · doi ↗ · pubmed ↗
- 7Classification of intraocular tuberculosis Ocul Immunol Inflamm Gupta A Sharma A Bansal R Sharma K 7132320152531436110.3109/09273948.2014.967358 · doi ↗ · pubmed ↗
- 8Standardization of nomenclature for ocular tuberculosis - results of Collaborative Ocular Tuberculosis Study (COTS) Workshop Ocul Immunol Inflamm Agrawal R Agarwal A Jabs DA 74842820203182109610.1080/09273948.2019.1653933 · doi ↗ · pubmed ↗