Symptomatic Cavum Vergae Cyst in a Geriatric Patient: A Report of a Rare Case and Conservative Management Approach
Plamen Penchev, Petar-Preslav Petrov, Vladislav Velchev, Andrey Velev

TL;DR
A 79-year-old woman with a rare symptomatic cavum vergae cyst showed improvement after conservative treatment, with no symptoms six months later.
Contribution
This paper reports a rare case of a symptomatic cavum vergae cyst in a geriatric patient and its successful conservative management.
Findings
The patient showed clinical improvement after conservative therapy for a symptomatic cavum vergae cyst.
Symptoms resolved completely six months post-treatment with no recurrence observed.
Conservative treatment may be an effective approach for managing symptomatic cavum vergae cysts in elderly patients.
Abstract
Cavum vergae (CV) cysts constitute a small proportion of intracranial cysts, and although generally asymptomatic, there are occasional cases where they might exhibit clinical manifestations. We present a clinical case of a 79-year-old female patient who had a clinical manifestation of headache on the occipital side of the head with irradiation to the shoulder girdle as well as numbness, dizziness, visual impairment, sleep disturbances, and tingling in the hands for three months. Vertigo and rightward staggering had been experienced for two weeks. On physical examination, it was discovered that there was smoothed physiological lordosis, restricted and painful movements, and paravertebral muscle rigidity in the cervical region. The patient had bilaterally reduced biceps and triceps reflexes, painful Erb’s points, and hypesthesia over the C5 and C6 dermatomes on the right side. The patient…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
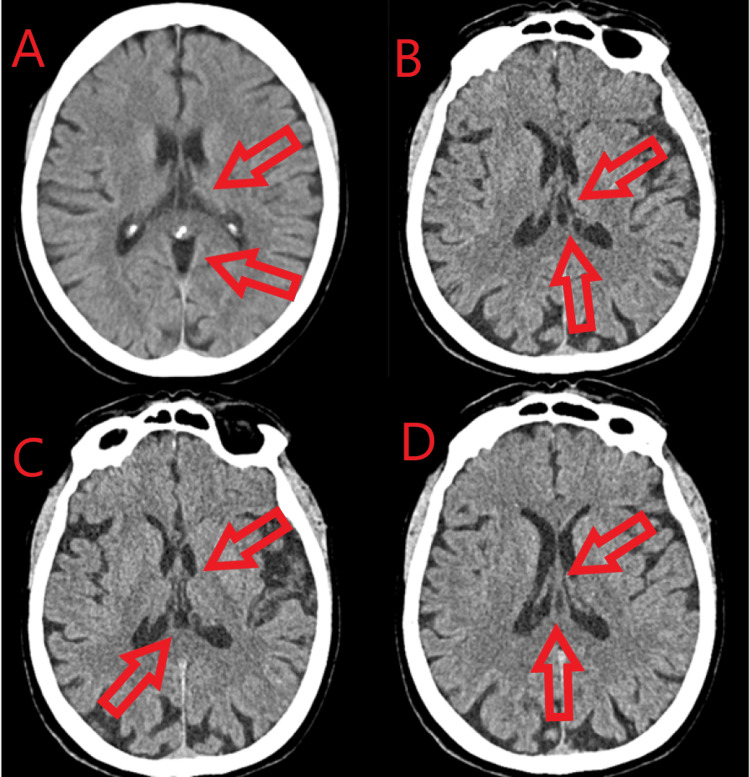 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFetal and Pediatric Neurological Disorders · Teratomas and Epidermoid Cysts · Urologic and reproductive health conditions
Introduction
The septum pellucidum (SP) is a thin, translucent, and triangular bilayer membrane that serves as a barrier between the right and left frontal horns and the lateral ventricles of the brain. The structure extends from the front part of the corpus callosum to the structure of the fornix, with a width ranging from 1.5 to 3.0 mm. The cavum SP (CSP) and cavum vergae (CV) are enduring membrane structures within the adult brain that arise due to the incomplete closure of the membranous leaves of the septum pylori. CV refers to the posterior extension of the SP [1].
The CSP cyst, the CV cyst, and the cavum velum interpositum cyst are some of the different types of benign midline anterior cerebral cysts. The cysts are considered pathological when they exhibit symptoms, which vary depending on their size. CV cysts are rare lesions with an incidence of 2.32% in adults. The majority of these cysts do not exhibit symptoms, although there are rare cases where they may manifest clinical symptoms. The most prevalent symptom is headache, although these lesions can present with a wide range of symptoms such as neurological deficit, ataxia, seizures, syncope, and visual and sensory irregularities [1-3].
The main purpose of this case report is to emphasize the significance of physicians considering a CV cyst as one of the various types of cystic lesions that may affect the SP. Moreover, we recommend selecting an initial conservative management approach as the preferable treatment plan if there is no blockage of CSF, compression of tissues, or changes in mental status. We could consider surgical intervention as a treatment option if conservative approaches prove ineffective.
Case presentation
We present a clinical case of a 79-year-old female patient who manifested headaches on the occipital side of the head, with irradiation to the shoulder girdle, as well as numbness, dizziness, visual impairment, sleep disturbances, and tingling in the hands for three months. No changes in mental status were observed. During this period, she received treatment with piracetam and betahistine, but the medications did not provide any effect. Over the past month, her movements became limited, and she tended to drop objects. Symptoms worsened in cold and damp weather with physical activity and prolonged standing, resulting in increased difficulty in performing daily activities. The patient experienced vertigo and rightward staggering for two weeks. Physical examination revealed smoothed physiological lordosis, restricted and painful movements, and paravertebral muscle rigidity in the cervical region. Bilaterally reduced biceps and triceps reflexes, painful Erb’s points, and hypesthesia over the C5 and C6 dermatomes on the right side were noted. The patient displayed decreased coordination and staggered movements to the right. A CT scan revealed dilated subarachnoid spaces of the convexity and a CV cyst (Figure 1).
CT scan (axial plane)(A, B, C, D) Dilated subarachnoid spaces of the convexity and a CV cystCV, cavum vergae
The patient was prescribed conservative therapy consisting of etoricoxib oral at a dosage of 2 × 60 mg for seven days, tolperisone hydrochloride orally at a dosage of 2 × 150 mg for seven days, pregabalin 75 mg, one pill in the evening for seven days, ozoid (a gel containing ozone) for external application, and vinpocetine 2 × 10 mg orally for two months. Following the conservative treatment, the patient exhibited improvement in her symptoms and no longer had challenges carrying out her daily tasks. Furthermore, six months after the therapy, the patient did not experience any symptoms. Long-term follow-up will be conducted in cases of symptom recurrence or cyst enlargement.
Discussion
Numerous studies fail to clearly state the duration of clinical progression for individual patients with CSP and/or CV cysts, according to Simonin and Lind. Nevertheless, the majority of cases exhibit a progression ranging from one month to three years [3]. Our patient’s clinical presentation demonstrated a three-month progression, aligning with the findings of Simonin and Lind.
In a recent meta-analysis with 368 patients conducted by Kryukov et al., the following symptoms were analyzed: headache (n = 184; 50%) and convulsive syndrome (n = 87; 23.6%); reduced intelligence/delayed psychomotor development (n = 74; 20.1%); mental disorders (n = 58; 15.8%); dizziness, nausea, and vomiting (n = 40; 10.9%); impaired consciousness (n = 36; 9.8%); gait disorders (n = 33; 9%); visual impairment (n = 31; 8.4%); optic nerve swelling (n = 17; 4.6%); cranial nerve dysfunction (n = 15; 4%); and hydrocephalus (n = 61; 16.6%) [4]. In the present study, the patient exhibited clinical manifestations including headache, dizziness, visual impairment, and sleep disturbances, therefore aligning with the findings of Kryukov et al.
Das and Dossani recommend surgical intervention when there is a blockage of CSF flow in the foramen of Monro, direct compression of adjacent tissues, or alterations in mental state [5]. Our case did not show any indications of CSF blockage, compression of nearby tissues, or alterations in mental state.
Several studies state that CSP and CV cysts are typically regarded as accidental observations; however, certain ones may have pathogenic effects. Several mechanisms can be used to justify this phenomenon. These mechanisms include the obstruction of the interventricular foramen, which can lead to hydrocephalus and/or increased intracranial pressure. Additionally, compression of the hypothalamic-septal triangle can result in neuropsychiatric symptoms, while compression of the optic chiasm and its pathways can also contribute to this condition. Furthermore, chronic deep venous involvement can cause progressive focal deficits [6-9]. Despite being congenital, we were unable to identify any etiological factor that could account for its clinical manifestation in the elderly.
Conclusions
This case report emphasizes the importance of considering CV cysts in the differential diagnosis of intracranial cystic lesions appearing on the SP, especially in older individuals who exhibit neurological symptoms. Although these cysts tend to be accidental findings, they might result in substantial morbidity if they exhibit symptoms. In instances where there is an absence of cerebrospinal fluid blockage or compression of nearby tissues, conservative therapy, as seen in our patient, has proven to be effective in reducing symptoms without requiring surgical intervention. The long-term follow-up of symptom recurrence or cyst expansion is of paramount significance. Additional investigation is necessary to have a more comprehensive understanding of the natural progression and most effective approaches for the management of CV cysts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cavum septum pellucidum and vergae cyst: a symptomatic case with intracranial hypertension and multiple nerve involvement Surg Neurol Int Ferreira DB Medeiros JW Cwajg E Ferreira-Pinto PH de Carvalho LU Nigri F 5641320223660073910.25259/SNI_822_2022 PMC 9805640 · doi ↗ · pubmed ↗
- 2Symptomatic cavum septum pellucidum cyst: a rare presentation Cureus Pillai B Farooque U Sapkota M Hassan SA Mechtler LL 012202010.7759/cureus.10395 PMC 755003133062515 · doi ↗ · pubmed ↗
- 3Surgical management of symptomatic cavum septum pellucidum cysts: systematic review of the literature Neurosurg Rev Simonin A Lind CR 242524324420213334005310.1007/s 10143-020-01447-4PMC 8490266 · doi ↗ · pubmed ↗
- 4Cysts of septum pellucidum, cavum vergae and cavum veli interpositi. Meta-analysis of 368 cases [Article in Russian]Zh Vopr Neirokhir Im N N Burdenko Kryukov EV Stanishevsky AV Gavrilov GV Gizatullin SK 1111188420203275993410.17116/neiro 202084041111 · doi ↗ · pubmed ↗
- 5Cavum septum pellucidum Stat Pearls [Internet] Das JM Dossani RH Treasure Island (FL)Stat Pearls Publishing 2024 https://pubmed.ncbi.nlm.nih.gov/30725733/30725733 · pubmed ↗
- 6Prevalence of cavum septum pellucidum and/or cavum vergae in brain computed tomographies of Taiwanese Acta Neurol Taiwan Chen JJ Chen CJ Chang HF Chen DL Hsu YC Chang TP 4954232014 https://pubmed.ncbi.nlm.nih.gov/26035920/26035920 · pubmed ↗
- 7Headache profiles in patients with a dilatated cyst of the cavum septi pellucidi Cephalalgia Wang KC Fuh JL Lirng JF Huang WC Wang SJ 8678742420041537731810.1111/j.1468-2982.2004.00760.x · doi ↗ · pubmed ↗
- 8Cava septi pellucidi et vergae: their normal and pathogical states Brain Shaw CM Alvord EC Jr 213223921969577402910.1093/brain/92.1.213 · doi ↗ · pubmed ↗