Pectoralis major muscle flap reconstruction after a total laryngectomy widened anteriorly: A case report
B. Saout Arrih, Y. Oukessou, W. Bijou, R. Abada, M. Mahtar

TL;DR
This case report shows successful use of a pectoralis major muscle flap for reconstructing a large defect after laryngeal cancer surgery.
Contribution
Demonstrates the continued effectiveness of pectoralis major flap in complex head and neck reconstructions despite advances in microsurgery.
Findings
Pectoralis major flap achieved excellent post-surgical outcomes in a complex laryngeal cancer case.
Flap's axial vascularization provides up to 98% viability rate in reconstructive procedures.
The flap remains a reliable option for cervicofacial reconstruction despite availability of free flaps.
Abstract
The pectoralis major flap is one of the leading regional pedicled flaps for reconstructive surgery of the head and neck, particularly in oncology after tumor resection. Despite the increasing use of free flaps, this type of flap is still highly recommended in defined indications. It is a highly reliable flap in terms of viability. We report the case of a man treated in our ENT department for a squamous cell carcinoma of the three laryngeal stages, anteriorly very extensive and requiring total laryngectomy extended to the skin and subcutaneous planes opposite, followed by reconstruction with a flap of the pectoralis major muscle. Post-surgical outcome was excellent. Aryan was the first person to describe the use of the pectoralis major muscle flap. Since then, several studies have demonstrated the great value of this flap in face and neck reconstruction, thanks to its wide indications…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1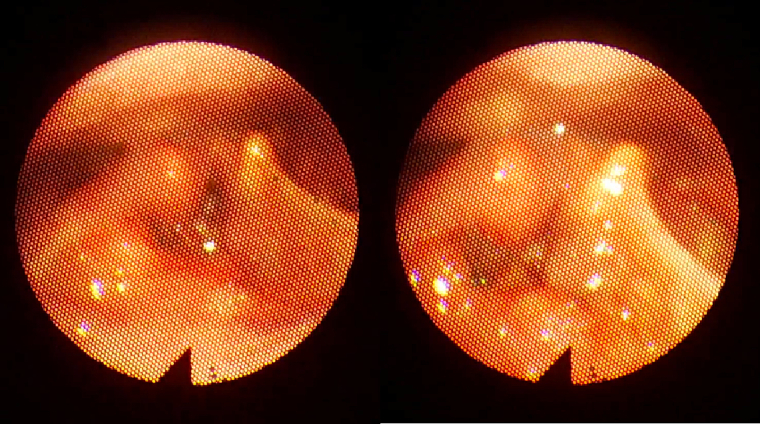 Figure 2
Figure 2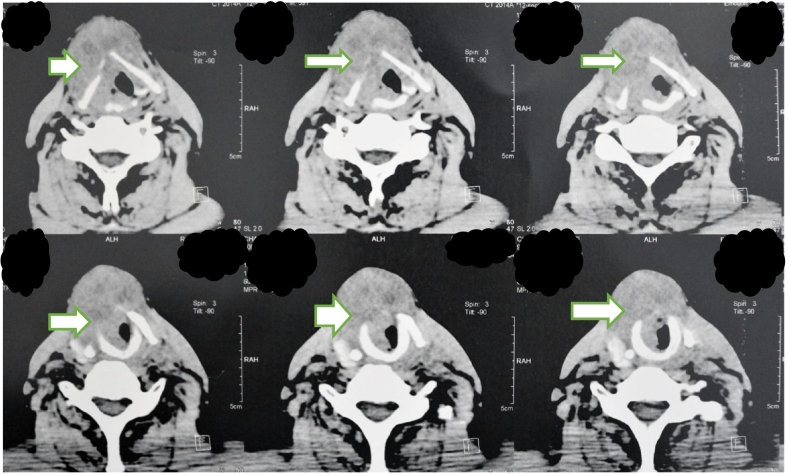 Figure 3
Figure 3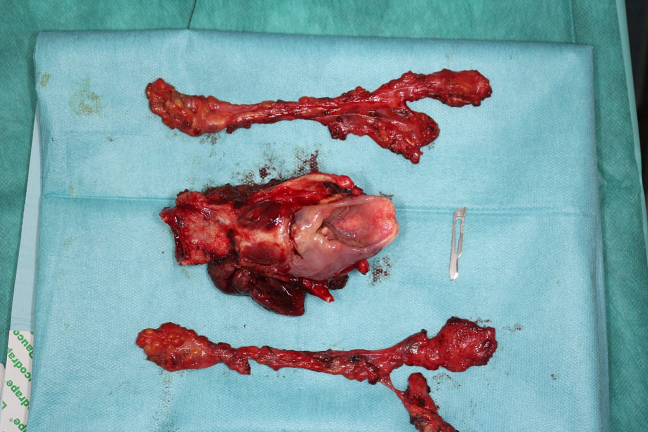 Figure 4
Figure 4 Figure 5
Figure 5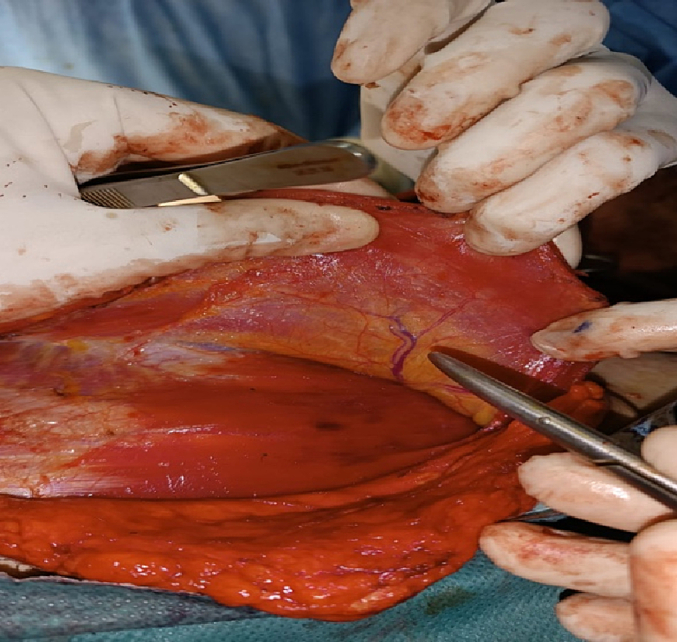 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReconstructive Surgery and Microvascular Techniques · Reconstructive Facial Surgery Techniques · Nerve Injury and Rehabilitation
Introduction
1
In general, three types of flaps can be differentiated. The local flap, which is a tissue harvested in the immediate vicinity of the defect to be repaired (e.g., advancement and transposition flaps). The pedicled flap, which does not originate from the immediate surroundings of the area to be covered. In fact, the tissue remains attached to its harvesting site by a pedicle that provides it with its blood supply, thus making reference to the “tunnelling” of the flap, which consists of passing the flap through a canal from the harvesting point. The free flap, which is completely excised from the distant donor site, requires reattachment to the recipient site via microvascular anastomoses.
Improved microsurgical techniques have made free flaps more prevalent over the years. Yet failure of a free flap is sometimes unavoidable, especially in patients with underlying vascular conditions. This makes the selection of an appropriate reconstructive method to fill residual defects for these patients a challenging task. Pedicled flaps for such patients, like the pectoralis major myocutaneous flap, are useful options for cervical and maxillo-facial reconstruction [1]. The pectoralis major myocutaneous flap was first introduced by Aryan, and has been used extensively for reconstructive surgery of the head and neck, with a rather long pedicle that includes the thoracoacromial artery as an axial vessel reaching all the cervicofacial regions, and a high-volume flap allowing reconstruction of large loss of tissue, as is often the case when performing surgery on extended tumors of the face and neck [1,2]. In this context, we report the case of a reconstruction involving loss of cervical tissue using the pectoralis major muscle flap after a total laryngectomy extended to the skin and the infrahyoid muscles opposite.
This case report has been reported in line with the SCARE criteria [10].
Case report
2
This is a study of a 53-year-old male patient operated on for a laryngeal tumor in our ENT and cervico-facial surgery department. The patient was referred to us from another hospital. It should be noted that the patient was a chronic smoker and suffered from ischemic heart disease and high blood pressure.
The history of the disease dates back 2 years to the onset of chronic dysphonia complicated 1 year later by inspiratory dyspnea requiring emergency tracheotomy (Fig. 1). On physical examination, a median cervical ulcerating mass was noted, without other associated signs, notably the patient had no dysphagia and no lymphadenopathy (Fig. 1).Fig. 1. Image showing externalization of the laryngeal tumor.Fig. 1
Nasofibroscopy reveals a mass that obstructs totally the glottic airway, occupying the glottic and supraglottic stages of the larynx, with both vocal cords fixed (Fig. 2).Fig. 2. Image showing the endoscopic appearance of the laryngeal tumor.Fig. 2
The cervical CT scan revealed a voluminous laryngeal process occupying all laryngeal subunits (supraglottic, glottic, subglottic), measuring 7 cm in long axis and invading the anterior commissure, lysing the thyroid, cricoid and arytenoid cartilages (Fig. 3).Fig. 3. Cervical CT scan showing a laryngeal tumor occupying all three laryngeal stages.Fig. 3
After being stabilized, the patient underwent suspension laryngoscopy with tumor biopsy. This revealed a tumor of all three laryngeal stages, extending far forward, beyond the anterior commissure, invading the infrahyoid muscles, the subcutaneous layers and externalizing through the skin. The tumor did not extend into the piriform fossa or the post-cricoid region, and the entrance to the esophagus was unobstructed. The base of the tongue was not invaded.
Pathological examination is consistent with undifferentiated squamous cell carcinoma.
The decision adopted at a multidisciplinary consultation meeting was to perform a total laryngectomy extended anteriorly to the infrahyoid muscles and the skin opposite, with bilateral cervical lymph node dissection and reconstruction of the tissue defect using a flap of the pectoralis major muscle, followed by adjuvant radiotherapy. The choice of this type of flap is based on the patient's cardiovascular condition and the large volume of the tumor, which may compromise the viability of a free flap (Fig. 4, Fig. 5).Fig. 4. Image showing the total laryngectomy specimen.Fig. 4. Fig. 5Image showing reconstruction of cervical tissue loss using a pectoralis major muscle flap.Fig. 5
The surgery was performed by an ENT specialist, performing a wide dissection of the peripheral skin and subcutaneous tissue over the skin paddle of the pectoralis major muscle up to the clavicle to expose the pectoralis major muscle and facilitate skin suturing, once the flap is made. The main objective when raising the flap was to clearly visualize the nourishing pedicle located on the deep surface of the pectoralis major muscle, and to preserve it during dissection and translation of the flap towards the cervical region (Fig. 6).Fig. 6. Image showing the nourishing pedicle of the pectoralis major muscle.Fig. 6
On definitive anatomopathological examination, we identified a squamous cell carcinoma of the larynx, invading the thyroid cartilage and infrahyoid muscles. Bilateral lymph node metastases were present, the largest measuring 2 cm on the right and 3 cm on the left. In the light of these data and the preoperative evaluation, we can classify this tumor as T4aN2cM0.
In the immediate postoperative period, we prescribed antibiotics, analgesics and cough suppressants to avoid infection and pressure on the flap's blood circulation. On the second postoperative day, the suction drains were removed. The patient stayed in our department for 7 days after surgery, with daily follow-up, where we checked the color and warmth of the flap to detect any incipient necrosis requiring our emergency intervention, and changed the dressing once a day, making sure it wasn't compressive.
Once the patient has left our department, the patient was advised to stop smoking, and to adopt regular physical activity along with a healthy diet, the aim is to achieve a satisfying blood circulation. We've established a follow-up plan involving consultations every 15 days for the first two months, then every month for the rest of the year. The sutures were removed by the doctor on the 15th postoperative day. All check-ups were favorable.
Discussion
3
The pectoralis major flap, as its name suggests, includes the pectoralis major muscle, with or without the skin opposite, and may even include the underlying ribs. It is one of the best-known regional pedicled flaps for reconstructive surgery of the head and neck, especially in oncology after tumor resection in the same operation [1]. It's a highly reliable flap, with a viability rate of up to 98 %, thanks to its axial vascularization based superiorly on the pectoral branch of the thoracoacromial artery. The principle is that a paddle of the pectoralis major muscle, with or without the skin opposite, is lifted and translocated to the cervico-facial region [2]. The pectoralis major muscle flap is a pedicled flap. Three main types can be differentiated. The first is the muscle flap completely covered by the skin paddle. The second is the island muscle flap, which requires dissection of the muscle upstream of the skin paddle, which may result in injury to the main pedicle, but does allow good mobility. The third is the type most commonly used today, with a long muscle paddle covered distally by a skin paddle, it allows reconstructing large losses of muscular and mucosal substance without an unusable volume of skin, this is the type used in the reported case [3,4]. Historically, Hueston in 1968 was the first to describe a technique combining pectoralis major muscle and skin, calling it a composite pectoral flap. But the basis of the pectoralis major muscle flap as we know it today was established by Aryan in 1979, whose technique used the skin of the anterior thorax overlying the pectoralis major muscle with its underlying axial vascular pedicle [5]. It is the flap to choose for patients with cancer requiring adjuvant radiotherapy. The volume of this flap is highly advantageous for musculocutaneous reconstruction of the neck and lower 1/3 of the face after major tumor resection, particularly of the buccal floor. Interestingly, the muscular surface becomes mucosialized even without the use of a skin paddle [6]. It is also indicated in patients with underlying cardiovascular conditions in whom the failure rate of free flaps is very high, as well as in salvage reconstruction after free flap failure. The only absolute contraindication is radical axillary lymph node dissection. Other contraindications that may limit the use of this flap include a history of breast surgery, which may reduce the quality and quantity of musculocutaneous perforating arteries. Poland syndrome, defined by the unilateral absence of the pectoralis major muscle. Morbid obesity with excessive adipose tissue that can compromise the survival of the skin palette. Also, smoking, diabetes and poor nutritional status are suspected of reducing flap survival. The major disadvantage of this flap is its unaesthetic appearance, especially for thin patients [7]. In addition to the advantage of being rapidly preformed, they are viable and reliable, and located close to the resection site in cases of reconstruction after enlarged total laryngectomy. They enable reconstruction in a single procedure, with low complication rates at the donor site. This avoids the need for salvage surgery if performed as a first-line procedure. However, it can also be used as a salvage procedure if the free flap fails [13]. This myocutaneous flap can reduce salivary fistula incidence rates from 24 % to 0 % according to Patel and Keni, and from 51 % to 20 % according to Righini. This goes well with the case reported, which has evolved excellently: the flap has not necrotized and no complications have occurred, especially no infection or salivary fistula despite advanced TNM tumor classification [11,12]. A study evaluated 220 patients and identified several risk factors directly linked to most of the complications that can occur. Hematomas are correlated with advanced tumor stage and, consequently, more radical surgery. Infections were more prevalent in patients with hemoglobin <10 g/dL, serum albumin <3 g/dL, and the presence of underlying systemic disease. Infections also increased significantly over the duration of hospitalization. The risk of fistula increased with more extensive resection, and with a bulky flap. Flap necrosis appears to be more frequent in women than in men, and in patients with underlying conditions [8]. Indeed, according to several studies, the rate of total flap necrosis remains very low, as in a study which reports a rate of only 2 % in a cohort of 500 cases [9].
Conclusion
4
In conclusion, we emphasize that the pectoralis major muscle flap still retains its indications despite the development of microsurgery and free flaps. This is mainly due to its high viability rate, the large musculocutaneous volume it offers for reconstructing large losses of substance, its rich vascular supply, its wide rotation arc and also its proximity to different areas of the face, oral cavity and cervical regions.
Provenance and peer review
Not commissioned, externally peer-reviewed.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval was provided by the authors institution.
Funding
None.
Guarantor
Saout Arrih Badr.
Research registration number
N/a.
CRediT authorship contribution statement
- Saout Arrih Badr: Study concept and writing the paper
- Oukessou Youssef: Study concept and correction of the paper
- Bijou Walid: Study concept and correction of the paper
- Rouadi Sami: Study concept and correction of the paper
- Abada Reda: Study concept and correction of the paper
- Mahtar Mohamed: Study concept and correction of the paper.
Declaration of competing interest
None.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Lean J.N.Carlson G.W.Losken A.The pectoralis major myocutaneous flap revisited: a reliable technique for head and neck reconstruction Ann. Plast. Surg.6420105705732035442910.1097/SAP.0b 013e 3181 c 51f 4a · doi ↗ · pubmed ↗
- 2Ariyan S.The pectoralis major myocutaneous flap. A versatile flap for reconstruction in the head and neck Plast. Reconstr. Surg.631979738137298810.1097/00006534-197901000-00012 · doi ↗ · pubmed ↗
- 3Sagayaraj, R P Deo, S M Azeem Mohiyuddin, G Oommen Modayil. Island Pectoralis Major Myocutaneous Flap: An Indian Perspective. 2011.10.1007/s 12070-011-0295-6PMC 343153223998034 · doi ↗ · pubmed ↗
- 4W P Magee Jr, J B Mc Craw, CE Horton, WD Mcinnis. Pectoralis “Paddle” Myocutaneous Flaps. The Workhorse of Head and Neck Reconstruction.10.1016/0002-9610(80)90201-97425233 · doi ↗ · pubmed ↗
- 5Kun Hwang. The Origins of Deltopectoral Flaps and the Pectoralis Major Myocutaneous Flap.10.1097/SCS.000000000000305727763977 · doi ↗ · pubmed ↗
- 6RD Keidan, J F Kusiak. Complications Following Reconstruction With the Pectoralis Major Myocutaneous Flap: The Effect of Prior Radiation Therapy.10.1288/00005537-199205000-000091573948 · doi ↗ · pubmed ↗
- 7Jakub Pazdrowski, Pawel Golusinski, Mateusz Szewczyk, Ewa. Pectoralis Major Myocutaneous Flaps vs. Revascularised Free Tissue Flaps Following Salvage Surgery for Recurrent Head and Neck Cancer.10.5604/01.3001.0015.950036622127 · doi ↗ · pubmed ↗
- 8Mehta, Sarkar, N Kavarana, I Bhathena, A Mehta. Complications of the Pectoralis Major Myocutaneous Flap in the Oral Cavity: A Prospective Evaluation of 220 Cases.10.1097/00006534-199607000-000068657786 · doi ↗ · pubmed ↗