Subintimal intravascular lithotripsy to optimize external crush stenting
Alexandru Achim, Zoltan Jambrik, Ferenc Nagy, Zoltan Ruzsa

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
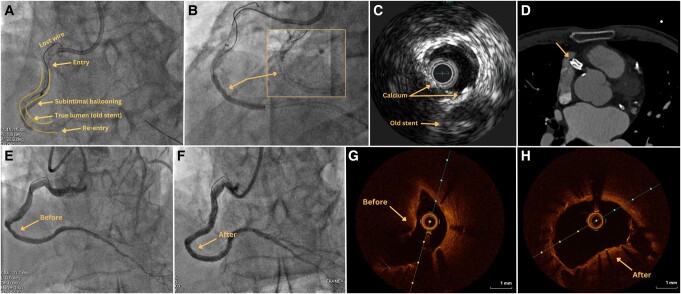 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Vascular Procedures and Complications · Peripheral Artery Disease Management
A 72-year-old male patient with a medical history marked by coronary artery disease and multiple triple-vessel stenting presented to our department due to pronounced angina and dyspnoea during minimal exertion, stemming from a long in-stent right coronary artery chronic total occlusion (CTO).
Employing an antegrade wire escalation technique, the wire could be advanced in the true lumen of the postero-descending artery, but with a long subintimal tracking, behind the old stent, as shown by intravascular ultrasound (IVUS). Contrary to prevailing beliefs advocating intentional subintimal tracking as a way to evade calcification,^1^ the new stent (parallel to the old one) could not expand or post-dilate at high pressures (Figure 1A and B; Supplementary material online, Video S1). This can be attributed to a dual challenge: the original stent, now in place for 5 years, had stiffened and accrued calcific neoatherosclerosis. Furthermore, IVUS revealed substantial extraplaque calcification, positioned opposite the initial stent (Figure 1C).
The patient was referred 3 months later for intravascular lithotripsy (IVL) at this level. Eighty pulsations were administered using a 3.5 mm balloon. The optical coherence tomography showed a well-endothelialized vessel, but with segments of under-expanded stent caused by a protruding calcified plaque [minimal stent area (MSA) 5.3 mm2]. Being a large vessel, the interrogation could not capture the depth of the old stent, but the computed tomography offered an evocative ‘double-barrel’ image (Figure 1D). Post-IVL and subsequent non-compliant 3.5 mm balloon dilation, an MSA of 10.1 mm^2^ was achieved (50% increase) (Figure 1E–H; Supplementary material online, Video S1). Finally, a 3.5 mm drug-eluting balloon (DEB) was applied.
In the context of in-stent CTO percutaneous coronary intervention (PCI) within heavily calcified vessels, subintimal IVL can modify the extraplaque calcium and improve vessel compliance to facilitate external crush stenting.^2^ This report not only re-affirms the safety of subintimal IVL post-endothelialization but also underscores the importance of incorporating plaque modification technologies in navigating through challenging calcified lesions, potentially superseding aggressive subintimal dilation methods. While the use of coronary IVL in the extraplaque space has been previously reported,^2^ it is still relatively rare due to the uncommon occurrence of significant extraplaque calcification. Given the potential risk of perforation associated with ad hoc extraplaque IVL,^3^ adopting a methodical stepwise strategy may be a more prudent approach, particularly when allowing the stent to undergo endothelialization. Given that the polymer of the stent remains unaffected by IVL shocks,^4^ but complete drug release occurs within 1–3 months, the recommendation is to incorporate a DEB at this stage. Chronic total occlusion PCI expertise remains essential when navigating such devices within the subintimal space.
Supplementary Material
ytae229_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mashayekhi KA , Pyxaras SA, Werner GS, Galassi AR, Garbo R, Boudou N, et al Contemporary issues of percutaneous coronary intervention in heavily calcified chronic total occlusions: an expert review from the European CTO Club. Euro Intervention 2023;19:e 113–e 122.36971414 10.4244/EIJ-D-22-01096 PMC 10240733 · doi ↗ · pubmed ↗
- 2Garbo R , Di Russo C, Sciahbasi A, Fedele S. The last resort during complex retrograde percutaneous coronary chronic total occlusion intervention: extraplaque intracoronary lithotripsy to externally crush a heavy calcified occluded stent. Catheter Cardiovasc Interv 2022;99:497–501.34939737 10.1002/ccd.30050 · doi ↗ · pubmed ↗
- 3Martín-Moreiras J , Trejo-Velasco B, Diego-Nieto A, Herrero-Garibi J, González-Ferreiro R, Cruz-González I. Coronary perforation after intracoronary lithotripsy in a chronic total coronary occlusion. REC: Interv Cardiol (English Edition)2021;2:159–160.
- 4Achim A , Alampi C, Krivoshei L, Leibundgut G. In vitro effect of intravascular lithotripsy on the polymer of a drug-eluting stent. Euro Intervention 2022;18:e 333–e 334.35775926 10.4244/EIJ-D-22-00300 PMC 9980395 · doi ↗ · pubmed ↗