Neuromyelitis Optica and Immune Thrombocytopenic Purpura Treated With Rituximab in a Patient With Combined Neurologic and Hematologic Disorder: A Case Report
Mary Remilenne E Rebanal-Ricafrente, Ma. Luisa Gwenn P Tiongson

TL;DR
A 56-year-old woman with both NMOSD and ITP showed improvement after treatment with Rituximab, highlighting its potential for combined neurological and hematologic disorders.
Contribution
This case report presents a rare coexistence of NMOSD and ITP successfully treated with Rituximab.
Findings
The patient's platelet count improved after methylprednisolone treatment for ITP.
Rituximab treatment led to improved neurological function as measured by the Expanded Disability Status Scale.
The patient's condition showed combined improvement in both neurological and hematologic symptoms.
Abstract
Neuromyelitis optica spectrum disorder (NMOSD) is a rare autoimmune inflammatory demyelinating disease of the central nervous system affecting the optic nerves and spinal cord. Immune thrombocytopenia (ITP), on the other hand, is an autoimmune disorder characterized by a platelet count of <100 in the absence of any known condition that could be associated with thrombocytopenia. This case report focuses on a 56-year-old female presenting with the unique coexistence of NMOSD and ITP. A 56-year-old woman of Russian descent had a sudden onset of right eye blindness at the age of 24 and was diagnosed with multiple sclerosis. She developed petechial rashes on both lower extremities two weeks before consultation with no associated findings. Cranial MRI revealed multiple nodular and patchy areas of hyperintense signals on T2-weighted/fluid-attenuated inversion recovery without restricted…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
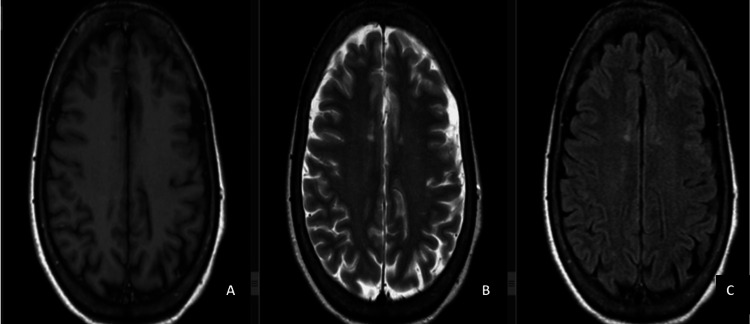 Figure 1
Figure 1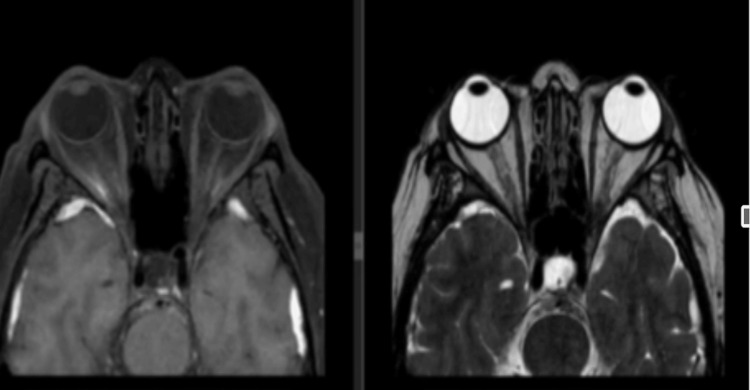 Figure 2
Figure 2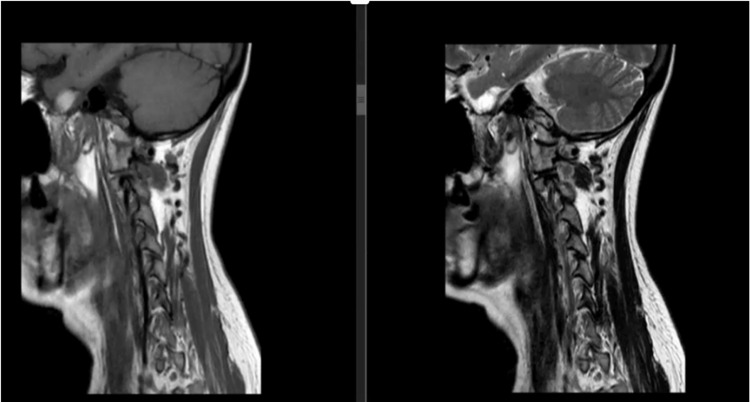 Figure 3
Figure 3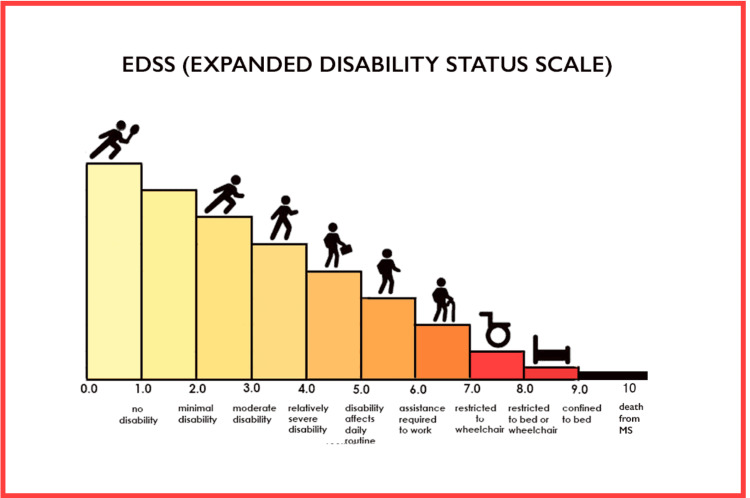 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Platelet Disorders and Treatments · Chronic Lymphocytic Leukemia Research
Introduction
Neuromyelitis optica (NMO) is a condition that predominantly targets the optic nerves, brainstem, and spinal cord, often leading to stepwise deterioration in affected individuals [1]. The progressive accumulation of visual, motor, and sensory deficits and bladder dysfunction due to recurrent attacks constitute the natural history of neuromyelitis optica spectrum disorder (NMOSD).
Immune thrombocytopenic purpura (ITP) is a hematologic disorder characterized by low platelet count. According to Dong et al., B-cell-depleting therapies such as rituximab have been widely used in ITP as second-line treatment due to the significant role of B cells in the pathogenesis of ITP [2].
NMOSD linked to aquaporin-4 immunoglobulin G antibodies (AQP4-IgG) necessitates serologic testing for accurate evaluations [3]. It is important to distinguish between seropositive and seronegative AQP4-IgG; however, it is noteworthy that the serological distinction between seronegative and seropositive NMOSD does not significantly impact relapse rates, disease severity, or long-term outcomes [3]. The intricate interplay between the immune system and hematopoietic processes in ITP raises intriguing questions regarding the potential connections between neurologic disorders and hematologic conditions.
Investigating such rare clinical scenarios is essential for unraveling the intricate mechanisms underlying the concurrence of these conditions and identifying potential treatment synergies that are yet to be discovered. By delving into our patient’s comprehensive clinical history, diagnostics, and therapeutic approach, we aim to shed light on the interrelationship between these two distinct yet interconnected disorders, offering insights that could potentially pave the way for innovative therapeutic strategies and improved patient care. In this report, we elucidate the clinical course, diagnostic challenges, and treatment outcomes of this intriguing case, thereby contributing to the evolving understanding of the complex nexus between neurologic and hematologic disorders.
Case presentation
We present the case of a 56-year-old woman of Russian descent who had experienced several autoimmune diseases. Her medical history included the onset of right eye blindness at the age of 24, following childbirth, and a subsequent diagnosis of multiple sclerosis (MS). Six months later, she developed right-sided weakness, which was exacerbated by stress. Treatment with intravenous methylprednisolone (1 g for five days) resulted in significant improvement. However, she continued to experience recurrent right eye blindness and bilateral lower extremity weakness over the next eight years, leading to her eventual reliance on a wheelchair.
Notably, the patient’s clinical course took an unexpected turn when she developed petechial rashes on both lower extremities two weeks before her consultation. These rashes appeared without any history of bleeding, vomiting, fever, cough, colds, or trauma. In 2018, the patient was diagnosed with multiple gastric ulcers, erosive gastritis, and a Helicobacter pylori infection. Additionally, she received a diagnosis of rectosigmoid adenocarcinoma stage I and underwent a sigmoidectomy with anastomosis.
Upon admission, the physical examination revealed the persistence of petechial rashes on both lower extremities. The neurologic evaluation showed reduced visual acuity (20/100 OD and 20/70 OS), with motor examination findings of 4/5 strength on neck flexion, shoulder elevation, shoulder abduction, elbow flexion, wrist and finger extension, as well as in the lower extremities. Sensory testing indicated 70% sensory intact on the right and left T7-L2 and 10% intact on L3-S1 bilaterally. The Expanded Disability Status Scale (EDSS) score upon admission was 7.0.
Advanced imaging studies were conducted to elucidate the underlying pathologies. Cranial MRI with contrast revealed extra-axial crescentic signals in the left occipital and bilateral temporal convexities. Nodular and patchy areas of hyperintense signals on T2-weighted/fluid-attenuated inversion recovery without restricted diffusion were observed in the bilateral centrum semiovale and periventricular white matter of the frontal and parietal lobes, left cerebral peduncle, and pons (Figure 1).
Cranial MRI with T1W (A) and T2W/FLAIR (B, C) hyperintense signals in the left occipital and bilateral temporal convexities. Nodular and patchy areas of T2W/FLAIR hyperintense signals in the centrum semiovale, periventricular white matter, cerebral peduncle, and pons. Small CSF-like signals in the medial temporal lobes.A: T1W. B: T2W. C: FLAIR.T1W: T1-weighted; T2: T2-weighted; FLAIR: fluid-attenuated inversion recovery; CSF: cerebrospinal fluid
Small cerebrospinal fluid (CSF)-like signals were noted in the bilateral medial temporal lobes. There was no evidence of acute infarct or abnormal contrast enhancement. Orbital MRI showed no distinct mass or enhancing lesions, (Figure 2), and cervical MRI displayed normal findings with intrinsically normal cervical cord without areas of enhancement (Figure 3).
Orbital MRI revealing no distinct mass or enhancing lesions, normal extraconal, intraconal, preseptal, and inferior or infraorbital regions; symmetrical extraocular muscles; and normal-sized optic nerves.Right: T2-weighted. Left: FLAIR: fluid-attenuated inversion recovery.
Cervical MRI displaying straightening of the normal cervical lordosis and intrinsically normal cervical cord without abnormal areas of enhancement.Right: T2-weighted. Left: FLAIR: fluid-attenuated inversion recovery.
A thoracolumbar MRI performed in 2021 revealed long segment foci of intramedullary cord non-enhancing abnormal hyperintense signal from T2 to T11, accompanied by mild volume loss. These findings raised the possibility of demyelinating diseases such as NMO rather than MS.
Additionally, the patient’s complete blood count indicated thrombocytopenia with a platelet count of 4 × 10^9^/L, with peripheral blood smear showing few normal-shaped platelets.
CSF testing for CSF AQP4-IgG and anti-myelin oligodendrocyte glycoprotein returned negative results. Given these findings, the patient was managed as a case of double seronegative NMO, with consideration for an underlying diagnosis of ITP.
The patient was promptly referred to a hematologist for co-management and was initiated on pulse therapy with intravenous methylprednisolone (1,000 mg/day) for five days. Remarkably, her platelet count improved from 4 to 50, then to 70, and eventually 100. The petechial rashes on all extremities resolved on the seventh day post-completion of pulse therapy. Subsequently, rituximab treatment was initiated at a dose of 1 g on day 1 and day 15. The patient also exhibited improvement in motor strength, with a transition from 4/5 to 4+/5 in all extremities. On the 18th day of hospitalization, her EDSS improved to 6.0 from the initial score of 7.0 upon admission.
Discussion
The diagnostic challenges in this case were multifaceted. Initially misdiagnosed with MS due to the clinical presentation of optic neuritis and subsequent central nervous system (CNS) involvement, the patient’s condition did not respond to traditional MS treatments such as azathioprine. Rituximab is a well-established preventive therapy for NMOSD [1]. However, the persistence of neurologic symptoms coupled with the emergence of petechial rashes on both lower extremities raised the suspicion of an underlying hematologic disorder, necessitating further investigation.
A comprehensive search for randomized controlled trials reporting the use of low-dose (100 mg) or standard-dose (375 mg/m^2^) rituximab in ITP treatment was conducted [2]. The administration of rituximab, a chimeric monoclonal antibody targeting CD20-positive B lymphocytes, marked a turning point in this patient’s treatment. The treatment of acute and recurrent attacks in NMOSD is based upon the evidence that humoral autoimmunity plays a role in the pathogenesis of NMOSD [4]. It was initiated at a dose of 1 g on day 1 and day 15, as commonly employed in induction treatment for NMOSD. NMOSD is a rare autoimmune inflammatory demyelinating disease of the CNS [4].
Further complicating the diagnosis was the patient’s history of other medical conditions, including gastric ulcers from H. pylori infection and rectosigmoid adenocarcinoma. H. pylori infection has been implicated in the pathogenesis, including cardiovascular, hematologic, and autoimmune diseases [5]. One hypothesis regarding the mechanism by which H. pylori induces the development of ITP is the cross-reactive antibodies that are produced that react with both H. pylori components and platelet surface antigens through molecular mimicry [5]. Other malignancies that were recorded to be related to NMOSD are the breast and ovary in women, while in men, lung, and prostrate predominate [6]. These comorbidities added a layer of complexity to the clinical picture and underscored the importance of a comprehensive assessment to unravel the interplay between neurologic and hematologic disorders.
The hematologic aspect of this case became apparent when thrombocytopenia was identified, with platelet counts as low as 4 × 10^9^/L.
ITP emerged as a plausible diagnosis, although the etiology remained elusive, as is often the case with ITP. The patient’s rapid and remarkable response to pulse therapy with intravenous methylprednisolone, leading to a significant increase in platelet counts and resolution of petechial rashes, provided crucial diagnostic and therapeutic insights.
The first study of rituximab showed that most peripheral blood B cells were depleted until 14 months [7]. Notably, the patient exhibited improved motor strength in all extremities following rituximab therapy, leading to a reduction in her EDSS score from 7.0 to 6.0.
The Expanded Disability Status Scale (EDSS) focuses mainly on the patient’s ability to walk.
Conclusions
This unique case underscores the challenges and complexities associated with the diagnosis and management of combined neurologic and hematologic disorders. The coexistence of NMOSD and ITP in this patient, along with the absence of AQP4-IgG seropositivity, highlights the clinical heterogeneity of NMOSD and the necessity of a broad diagnostic approach.
Prompt recognition of the hematologic component, namely, ITP, was pivotal in this case. The subsequent initiation of rituximab therapy not only resulted in hematologic improvement but also contributed to enhanced motor function.
The case sheds light on the evolving treatment landscape for NMOSD and highlights the potential utility of rituximab in managing this complex disorder. Further research and case studies are warranted to better understand the underlying mechanisms and optimal treatment strategies for patients with similar presentations, ultimately improving their quality of life and prognosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Recommendations for the use of rituximab in neuromyelitis optica spectrum disorders Rev Neurol (Paris) Ciron J Audoin B Bourre B 2552641742018 https://doi.org/10.1016/j.neurol.2017.11.0052960632010.1016/j.neurol.2017.11.005 · doi ↗ · pubmed ↗
- 2The efficacy and safety of different dosages of rituximab for adults with immune thrombocytopenia: a systematic review and meta-analysis Biomed Res Int Dong Y Yue M Hu M 999208620212021 https://doi.org/10.1155/2021/99920863466080710.1155/2021/9992086 PMC 8514896 · doi ↗ · pubmed ↗
- 3Neuromyelitis Optica Spectrum Disorder (NMOSD) Shumway CL Patel BC Tripathy K De Jesus O Treasure Island, FL Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 572108/34283474 · pubmed ↗
- 4Neuromyelitis optica spectrum disorder (NMOSD): treatment and prognosis Up To Date Glisson CC Philadelphia, PA Wolters Kluwer 2023 https://www.uptodate.com/contents/neuromyelitis-optica-spectrum-disorder-nmosd-treatment-and-prognosis
- 5Helicobacter pylori-associated immune thrombocytopenia: clinical features and pathogenic mechanisms World J Gastroenterol Kuwana M 714723202014 https://doi.org/10.3748/wjg.v 20.i 3.7142457474510.3748/wjg.v 20.i 3.714PMC 3921481 · doi ↗ · pubmed ↗
- 6Neuromyelitis optica spectrum disorder (NMOSD) associated with cancer: a systematic review Mult Scler Relat Disord Shahmohammadi S Doosti R Shahmohammadi A Azimi A Sahraian MA Fattahi MR Naser Moghadasi A 103227562021 https://doi.org/10.1016/j.msard.2021.1032273453677410.1016/j.msard.2021.103227 · doi ↗ · pubmed ↗
- 7Neuromyelitis optica spectrum disorder coinciding with hematological immune disease: a case report Mult Scler Relat Disord Patejdl R Wittstock M Zettl UK Jost K Grossmann A Prudlo J 10110392016 https://doi.org/10.1016/j.msard.2016.07.0062764535310.1016/j.msard.2016.07.006 · doi ↗ · pubmed ↗